Introduction
Scoliosis is lateral curvature of the spine greater than 100 accompanied by vertebral rotation. The prime risk factors for curve progression are a large curve magnitude, skeletal immaturity and female gender. The curve progression can be recorded by measuring the curve magnitude using the Cobb’s method on radiographs.
Aim
To assess the effect of task oriented exercises based on ergonomics on Cobb’s angle and pulmonary functions on one year outcome of Adolescent Idiopathic Scoliosis(AIS) (defined as curves < 150 for thoracolumbar region and < 200 for thoracic region).
Materials and Methods
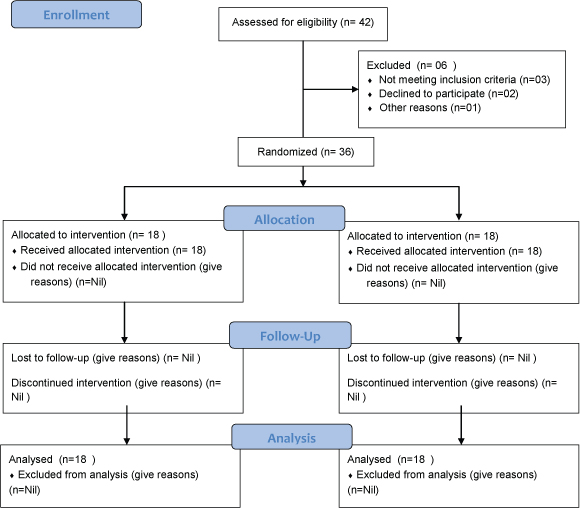
A total of 36 patients were enrolled in the study and 18 patients in each group (experimental and control group) were allocated randomly. The subjects in control group underwent spinal strengthening exercises, active self-correction and breathing exercises, whereas subjects in the experimental group followed task oriented exercises based on ergonomics in addition to exercises for conventional group for one year. Chi square test was used to compare the categorical/ dichotomous variables between the groups. Unpaired t-test was used to compare continuous variables between the groups at pre and post intervention. Paired t-test was used to compare the changes in continuous variables from pre to post intervention within the group.
Results
Forced Vital Capacity (FVC) was found to be significantly (p=0.001) higher in experimental group (2.68±0.37) than control group (2.20±0.41) at post-intervention. Force Expritatory Volume 1 (FEV1) (p=0.01) and Vital Capacity (VC) (p=0.002) were also found to be significantly higher in experimental group compared to control group at postintervention. Also, there was significant (p=0.001) mean reduction in Cobb’s angle from pre to post intervention in both the groups being higher in Experimental group than control group.
Conclusion
The task oriented exercise protocol benefited patients with AIS which had a significant improvement of their pulmonary functions and Cobb’s angle.
Adam’s forward bend test, Lateral curvature, Spinal strengthening
Introduction
AIS is a most common form of scoliosis which is seen in children aged at least 10 years. Scoliosis is defined as a lateral curvature of the spine greater than 100 accompanied by vertebral rotation [1]. Cause is usually unknown but it is thought to be a multigene dominant condition with variable phenotypic expression [2]. Adam’s forward bend test is helpful in identifying scoliosis during physical examination [3]. Secondary causes of spinal deformity are severe pain, a left thoracic curve or an abnormal neurologic examination findings pointing to speciality consultation. Of adolescents diagnosed with scoliosis, only 10% have curves that progress and require medical intervention [4]. Larger curve magnitude, skeletal immaturity and female gender are the prime risk factors for curve progression. The curve progression can be recorded by measuring the curve magnitude using the Cobb’s method on radiographs.
There is need to differentiate patients with stable or minimally progressive scoliosis who can be isolated from patients with scoliosis that is at high risk for progression. It is therefore needed to determine the patients so that they can follow referral to an orthopaedic surgeon. Referrals of cases of AIS with minor curves with low risk of progression may lead to marked anxiety and loss of time from school and work [5].
Idiopathic scoliosis occurs due to lateral displacement and rotation of vertebral bodies during process of skeletal maturity attainment and it has also adverse effects on respiratory function. It can cause restrictive lung disease [6], decrease of lung volumes and also the movement of ribs is disturbed [7], affecting the working of the respiratory muscles. The chest wall is disorganized and the lung compliance is impaired which may result in laborious breathing during rest, exercise and sleep [8].
The primary goal of rehabilitation for AIS is to reduce the progression of curves thereby decreasing the risk of secondary impairment, including back pain, breathing problems, cosmetic deformities, and improve the quality of life [9,10].
Scoliosis affects pulmonary function in many ways as it can be usually painless and asymptomatic at an early stage but the resultant lung function abnormalities are mainly of the restrictive type and the duration of scoliosis correlates with the patient’s degree of disability [11].
Conservative measures of treatment for AIS are exercises, braces and postural education. The usual protocol followed in King George’s Medical University, Uttar Pradesh, India (KGMU, the institute where the study was conducted), is that patients of AIS are advised for spinal exercises and braces for those who are having greater curve and also if they do not respond to conservative measures. The exercises prescribed are active exercises and breathing exercises. The active exercises prescribed are self-correction, spinal strengthening and spinal mobilization exercises.
There are reports that adding task oriented exercises have improved outcome measured as progression of the curve measured by Cobb’s method, functional outcome [12]. However, the study did not assess the effect of task oriented exercises based on ergonomics on the respiratory function. Other studies have also not focused on respiratory function as an outcome measure.
There should be an approach to diagnosing and treating scoliosis that allows physicians to lessen the adverse psychological, medical and economic effects of over referral or delayed referral of adolescents to orthopaedic subspecialists [13].
There are several exercise approaches such as Scoliosis Specific Exercise (SSE) recommended by Scientific Society on Scoliosis Orthopaedic Rehabilitation and Treatment (SOSORT), Scientific Exercises Approach to Scoliosis (SEAS) Italy, Barcelona Scoliosis Physical Therapy Approach (BASPT), Dobomed (Poland) and Lyon approach (France), confirming the effectiveness of exercises in AIS by improving the rib cage alignment and pelvic balance and bring them to normal anatomical postures but still these need to be confirmed by advance research approaches [14].
This study was focused to find out the effects of special exercise program on Cobb’s angle and pulmonary functions in AIS. It assess the effect of task oriented exercises based on ergonomics on one year outcome of AIS.
Materials and Methods
Study design was Randomized Control Trial (RCT) and the study duration was from April 2015 to March 2016. The ethical approval was taken from the Institutional Ethics Committee, KGMU and the RCT was being registered with Clinical trial registry of India (Registration no. CTRI/2017/02/007901). The consent was taken from each participant after explaining the objective of the study and ensured them about the confidentiality.
Inclusion Criteria
Eligible subjects were between the age group of 10-15 years diagnosed as fixed AIS with Cobb’s angle <20° for thoracic curves and <15° for thoracolumbar curves subject to written informed consent. Subjects who were having AIS with correctable deformity, any pathology and/or deformity of lower limbs disturbing spinal posture, systemic illness or cardio-respiratory dysfunction, who had undergone spinal surgery or rehabilitation elsewhere and cognitive impairment were excluded from the study.
A total of 36 patients of AIS were selected as per sample size calculation through formula by Hayes RJ and Bennett S 1999 [15]:
n=7.84 X [σ02+σ12)/(µ0-µ1)2
n=sample size per group which is 18
All the selected subjects were those who reported to OPD of Physical Medicine and Rehabilitation (PMR) and Orthopaedic Surgery, KGMU. Screening was conducted prior to enrolment to ensure eligibility by Physiotherapist who was not associated with study and patients were divided in two groups i.e., experimental and control group according to random number table generated from Microsoft XL. Randomization and blinding were ensured by allocation concealment. Patients were not aware of the group to which they were being allocated. All patients enrolled in the study were assessed for baseline data that included- age, sex, Cobb’s angle measurement and pulmonary functions test.
Intervention
All the subjects in control group underwent spinal strengthening exercises, active self-correction and breathing exercises whereas subjects in the experimental group followed task oriented exercises based on ergonomics in addition to exercises for conventional group for one year.
Control group:
Spinal extension (upper and lower) exercises- 10 times for 5 mintues each.
Spinal strengthening of convex side muscles by lying on concave side and upper trunk raising up- 10 times for 5 mintues.
Active self-correction:
- Lying on convex side with towel roll placed under apex – 10 mintues;
- Side shift on medicine ball toward convexity- 10 times for 5 mintues;
- Hip hitch exercise – 10 times for 5 mintues.
Breathing exercises:
- Chest expansion exercises with emphasis on concave side- 5 mintues;
- Diaphragmatic breathing exercises- 5 mintues.
Experimental group:
All exercises prescribed in control group and
Task oriented exercises:
1- Lying on concave side and lifting upper trunk to touch a target through stretched hand- 10 times for 5 minutes;
2- Walking 10 m with sand bag of 2 kg placed overhead- 5 minutes;
3- Sitting to standing and stretching both upper limbs to touch uppermost bar of ladder placed in front- 10 times for 5 minutes;
4- Picking up the ball placed on a table on concave side and throwing it on a tub placed on the other side- 10 times for 5 minutes;
5- Putting the basketball in the overhead net through hand of concave side curve- 10 times for 5 minutes.
Outcome measures:
Both the groups were assessed by a blinded observer at six monthly follow up for[Table/Fig-1]:
1) Cobb’s angle measurement;
2) Pulmonary function test.
Statistical Analysis
The results were presented in mean±SD and percentages. Chisquare test was used to compare the categorical/dichotomous variables between the groups. Unpaired t-test was used to compare continuous variables between the groups at pre and post intervention. Paired t-test was used to compare the changes in continuous variables from pre to post intervention within the group. The p-value<0.05 was considered significant. All the analysis was carried out on SPSS 16.0 version (Chicago, Inc., USA).
Results
There was no significant (p>0.05) difference in the age and sex between the groups showing comparability of the groups in terms of age and sex [Table/Fig-2].
Age and sex distribution between the groups.
| Age and sex | Experimental group (n=18) | Control group (n=18) | p-value1 |
|---|
| No. | % | No. | % |
|---|
| Age in years | | | | | |
| <12 | 7 | 38.9 | 9 | 50.0 | 0.50 |
| ≥12 | 11 | 61.1 | 9 | 50.0 |
| Mean±SD | 12.17±1.72 | | 11.56±1.46 | |
| Sex | | | | |
| Male | 11 | 61.1 | 10 | 55.6 | 0.73 |
| Female | 7 | 38.9 | 8 | 44.4 |
Chi-square test
There was no significant (p>0.05) difference in the pulmonary function tests at pre-intervention between the groups [Table/Fig-3].
Comparison of pulmonary function tests between the groups at pre intervention.
| Pulmonary function tests | Experimental group (n=18) | Control group (n=18) | p-value1 |
|---|
| FVC | 1.69±0.21 | 1.80±0.46 | 0.34 |
| FEV1 | 1.52±0.22 | 1.69±0.48 | 0.19 |
| FEV1/FVC | 84.88±12.03 | 84.31±11.99 | 0.88 |
| PEF | 3.99±1.03 | 4.17±1.29 | 0.65 |
| VC | 1.89±0.20 | 2.08±0.48 | 0.13 |
Unpaired t-test
FVC was found to be significantly (p<0.001) higher in experimental group (2.68±0.37) than control group (2.20±0.41) at post-intervention. FEV1 p=0.01 and VC (p=0.002) were also found to be significantly higher in experimental group compared to control group at post-intervention. There was no significant difference (p>0.05) in FEV1/FVC and PEF between e xperimental group and control group at post-intervention [Table/Fig-4].
Comparison of pulmonary function tests between the groups at post intervention.
| Pulmonary function tests | Experimental group (n=18) | Control group (n=18) | p-value |
|---|
| FVC | 2.68±0.37 | 2.20±0.41 | <0.001* |
| FEV1 | 2.30±0.50 | 1.92±0.39 | 0.01* |
| FEV1/FVC | 83.79±8.23 | 85.95±6.52 | 0.39 |
| PEF | 5.79±1.49 | 5.90±1.91 | 0.85 |
| VC | 2.75±0.32 | 2.35±0.39 | 0.002* |
1Unpaired t-test,
Significant
There was significant (p<0.01) change in all the pulmonary function tests except FEV1/FVC from pre to post intervention in both the groups. However, mean change was observed to be higher in experimental group than control group [Table/Fig-5].
Comparison of mean change in pulmonary function tests from pre to post intervention within group.
| Pulmonary function tests | Experimental group (n=18) | Control group (n=18) |
|---|
| Mean change | p-value1 | Mean change | p-value1 |
|---|
| FVC | 0.99±0.34 | 0.0001* | 0.39±0.43 | 0.001* |
| FEV1 | 0.78±0.37 | 0.0001* | 0.23±0.32 | 0.006* |
| FEV1/FVC | 1.08±11.22 | 0.68 | 1.63±14.38 | 0.63 |
| PEF | 1.80±1.24 | 0.0001* | 1.73±1.77 | 0.001* |
| VC | 0.86±0.33 | 0.0001* | 0.27±0.27 | 0.001* |
1Paired t-test,
Significant
There was no significant (p>0.06) difference in Cobb’s angle at preintervention between the groups. A significant (p<0.001) difference was found in Cobb’s angle at post intervention between the groups. There was significant (p<0.001) mean change in Cobb’s angle from pre to post intervention in both the groups being higher in experimental group than control group [Table/Fig-6].
Comparison of Cobb’s angle between the groups across time periods.
| Groups | Pre intervention | Post intervention | Mean change | p-value1 |
|---|
| Experimental group | 12.61±1.81 | 6.83±1.72 | 5.77±1.35 | <0.001* |
| Control group | 12.72±1.40 | 9.67±1.32 | 3.05±0.80 | <0.001* |
| p-value1 | 0.83 | <0.001* | | |
1Paired t-test, 2Unpaired t-test,
Significant
Discussion
In our study, we found a significant improvement in pulmonary functions in experimental group rather than control group as there was significant increase in FVC, FEV1 and VC in experimental group higher than control group.
dos Santos Alves VL et al., in their study found that there was an improvement in FVC, inspiratory capacity; FEV1, expiratory reserve volume, and performance assessed by 6 Minute walk test (6MWT) were observed after physical rehabilitation [16]. They suggested that global conditioning improved after the rehabilitation program. This was expressed by both PFT and 6MWT results.
In another study, by dos Santos Alves VL et al., suggested that exercise is beneficial to patients with AIS, who have shown significant increases in respiratory muscle strength after physical therapy [17]. There was no correlation between respiratory pressure and spine deformity.
Shneerson JM and Madgwick R et al., showed that exercises can significantly improve the lung functions and activity level and thereby can be helpful in reducing the rate of surgical interventions in cases of AIS [18]. Smyth RG et al., suggested that when training provides control of breathing pattern, increased strength and inspiratory muscle endurance can translate into clinical improvement of the respiratory system functional status of patients with chronic lung disease, as it was observed in their study with AIS patients [19].
In this study, the exercises have shown significant reduction in Cobb’s angle suggesting that the exercises are helpful in arresting the progression of curve and reducing the deformity in AIS.
In a review, Negrini et al., reported that exercise had beneficial effects on the rate of progression and Cobb’s angle [20]. They also found positive effects of exercise in reducing brace prescriptions.
Negrini S et al., in their systematic review concluded that there is absence of sufficient evidence against effectiveness of physical exercises for prevention of curve progression in AIS [21]. In another study, Mordecai SC and Dabke HV suggested that there is poor quality evidence in support of exercise in the management of AIS [22].
There are studies confirming the effectiveness of exercises in adolescent scoliosis patients who are at high risk of progression [23,24]. Negrini S et al., found and suggested in the study that specific and personalized exercise treatment appears to be more effective than usual physiotherapy in reducing the progression of scoliosis [25].
Zapata K et al., concluded in their study that a year after performing exercises, unsolicited corrective exercises resulted in a significantly improved Cobb’s angle compared to relaxed standing for the curve primarily targeted by the exercise program [26]. Improved exercise ability and spinal flexibility may have contributed to the improved Cobb’s angle. Wearable technology is needed to better understand how much time patients are spending in their corrected versus relaxed postures.
Limitation
One of the limitations of this study was small sample and less duration. The studies with larger sample size and longer duration are required for robust conclusions.
Conclusion
The therapy protocol benefited patients with AIS, which had a significant improvement of their pulmonary functions and Cobb’s angle, as compared to patients with AIS who did not undergo the specific exercise protocol allocated in control group.
1Chi-square test
1Unpaired t-test
1Unpaired t-test,
*Significant
1Paired t-test,
*Significant
1Paired t-test, 2Unpaired t-test,
*Significant
[1]. Cobb JR, Edwards JW, Outline for the study of scoliosisAAOS, Instructional Course Lectures 1948 5Ann ArborThe American Academy of Orthopaedic Surgeons:261-75. [Google Scholar]
[2]. Miller NH, The role of genetic factors in the etiology of idiopathic scoliosisSpine: State Art Rev 2000 14:313-17. [Google Scholar]
[3]. Roach JW, Adolescent idiopathic scoliosisOrthop Clin North Am 1999 30:353-65. [Google Scholar]
[4]. Reamy Brian V, Slakey Joseph B, Adolescent idiopathic scoliosis: review and current conceptsAm Fam Physician 2001 64(1):111-17. [Google Scholar]
[5]. Screening for adolescent idiopathic scoliosis. Policy statement. US Preventive Services Task ForceJAMA 1993 269(20):2664-66. [Google Scholar]
[6]. Praud Jaen-Paul Canet E, Chernick V, Boat TF, Wilmott RW, Bush A, Chest wall function and dysfunctionKendig’s Disorders of the Respiratory Tract in Children 2006 7 editionPhiladelphiaSaunders Elsevier:733-46. [Google Scholar]
[7]. Redding GJ, Praud J-P, Mayer OH, Pulmonary function testing in children with restrictive chest wall disordersPediatric Allergy, Immunology, and Pulmonology 2011 24(2):89-94. [Google Scholar]
[8]. Striegl A, Chen ML, Kifle Y, Song K, Redding G, Sleep-disordered breathing in children with thoracic insufficiency syndromePediatr Pulmonol 2010 45(5):469-74. [Google Scholar]
[9]. Weinstein SL, Dolan LA, Cheng JC, Danielsson A, Morcuende JA, Adolescent idiopathic scoliosisLancet 2008 371(9623):1527-37. [Google Scholar]
[10]. Goldberg MS, Mayo NE, Poitras B, Scott S, Hanley J, The Ste-Justine adolescent idiopathic scoliosis cohort study. Part II: Perception of health, self and body image, and participation in physical activitiesSpine (Phila Pa 1976) 1994 19(14):1562-72. [Google Scholar]
[11]. Koukourakis I, Giaourakis G, Kouvidis G, Kivernitakis E, Blazos J, Koukourakis M, Screening school children for scoliosis on the island of CreteJ Spinal Disord 1997 10(6):527-31. [Google Scholar]
[12]. Monticone M, Ambrosini E, Cazzaniga D, Rocca B, Ferrante S, Active self-correction and task-oriented exercises reduce spinal deformity and improve quality of life in subjects with mild adolescent idiopathic scoliosis. Results of a randomised controlled trialEur Spine J 2014 23(6):1204-14. [Google Scholar]
[13]. Tsiligiannis T, Grivas T, Pulmonary function in children with idiopathic scoliosisScoliosis 2012 7(1):07 [Google Scholar]
[14]. Saltikov J B, Cook T, Rigo M, Mauroy J C D, Romano M, Negrini S, Physical therapy perspectives in the 21st century – challenges and possibilities April 2012 UKIntech PublishingISBN 978-953-51-0459-9 [Google Scholar]
[15]. Hayes RJ, Bennett S, Simple sample size calculation for cluster-randomized trialsInt J Epidemiol 1999 28(2):319-26. [Google Scholar]
[16]. dos Santos Alves VL, Stirbulov R, Avanzi O, Impact of a physical rehabilitation program on the respiratory function of adolescents with idiopathic scoliosisChest 2006 130(2):500-05. [Google Scholar]
[17]. d os Santos Alves VL, Avanzi O, Respiratory muscles strength in idiopathic scoliosis after training programActa Ortop Bras 2016 24:6 [Google Scholar]
[18]. Shneerson JM, Madgwick R, The effect of physical training on exercise ability in adolescent idiopathic scoliosisActa Orthop Scand 1979 50(3):303-06. [Google Scholar]
[19]. Smyth RJ, Chapman KR, Wright TA, Crawford JS, Rebuck AS, Pulmonary function in adolescents with mild idiopathic scoliosisThorax 1984 39(12):901-04. [Google Scholar]
[20]. Negrini S, De Mauroy JC, Grivas TB, Knott P, Kotwicki T, Maruyama T, Actual evidence in the medical approach to adolescents with idiopathic scoliosisEur J Phys Rehabil Med 2014 50(1):87-92. [Google Scholar]
[21]. Negrini S, Antonini G, Carabalona R, Minozzi S, Physical exercises as a treatment for adolescent idiopathic scoliosisA systematic review. Pediatr Rehabil 2003 6(3-4):227-35. [Google Scholar]
[22]. Mordecai SC, Dabke HV, Efficacy of exercise therapy for the treatment of adolescent idiopathic scoliosis: a review of the literatureEur Spine J 2012 21(3):382-89. [Google Scholar]
[23]. Lenssinck ML, Frijlink AC, Berger MY, Bierman-Zeinstra SM, Verkerk K, Verhagen AP, Effect of bracing and other conservative interventions in the treatment of idiopathic scoliosis in adolescents: a systematic review of clinical trialsPhys Ther 2005 85(12):1329-39. [Google Scholar]
[24]. Negrini S, Aulisa L, Ferraro C, Fraschini P, Masiero S, Simonazzi P, Italian guidelines on rehabilitation treatment of adolescents with scoliosis or other spinal deformitiesEura Medicophys 2005 41(2):183-201. [Google Scholar]
[25]. Negrini S, Zaina F, Romano M, Negrini A, Parzini S, Specific exercises reduce brace prescription in adolescent idiopathic scoliosis: a prospective controlled cohort study with worst-case analysisJ Rehabil Med 2008 40(6):451-55. [Google Scholar]
[26]. Zapata K, Parent EC, Sucato D, Immediate effects of scoliosis-specific corrective exercises on the Cobb angle after one week and after one year of practiceScoliosis and Spinal Disorders 2016 11(Suppl 2):36 [Google Scholar]