CD is a rare lymphoproliferative disorder with heterogenous clinical and pathological features. It is so rare that reputed textbooks on lymph node pathology do not mention its prevalence [1]. Estimates of 6500-7700 new cases of all variants of CD being detected among the entire United States population are mentioned on the CD collaborative network website [2]. CD is of such low prevalence that it has been mentioned as one of the rare disease in orphanet with an identity of orpha number160 and ICD -10:D47.4 [3].
It can present as unicentric or multicentric disease. Unicentric disease can involve single lymphnode or single group of lymph nodes without systemic symptoms. Multicentric disease present with diffuse lymphnode enlargement with systemic symptoms and various laboratory abnormalities [3-5]. Unicentric disease is more common than multicentric disease though there is no consensus regarding exact proportion of the two subtypes [5,6].
Hyaline Vascular Variant (HV-CD) and Plasma Cell Variant (PCD) are the two major pathological subtypes. Hyaline vascular subtype is characterised by lymphoid follicles scattered in a mass of lymphoid tissue with increased vascular proliferation and hyalinization of germinal centres [7]. Plasma cell subtype show increased plasma cells in interfollicular region [7]. Presence of overlapping histological features is seen in mixed subtypes. Hyaline vascular variant being the most common histological subtype, accounts for nearly 80% to 90% of unicentric cases [8].
Histopathological classification is preferred over classification based on clinical presentation [9]. CD is a pathological diagnosis in most of the cases. It is very rare to have a clinical differential diagnosis of CD due to its varied clinical presentation. Hyaline vascular variant of CD is the most common subtype of CD. Two subcategories are described in this subtype based on relative morphologic changes in follicular and interfollicular region. Follicular hyaline vascular variant of CD show predominantly follicular abnormalities which compose more than 50% of the lymphnode. Whereas stroma rich subtype show predominantly interfollicular changes like presence of numerous sclerotic blood vessels. Interfollicular region with proliferating blood vessels constitute more than 50% of lymph node [10].
Broad morphologic spectrum with varying combination of microscopic features leads to wide differential diagnosis even on histopathological evaluation. It is important to diagnose CD among the non neoplastic lymphadenopathy as it can mimic infectious conditions and non Hodgkin lymphoma clinically. Thus, the histomorphology based diagnosis is a first step in the management of CD. In this study, we attempt to study these morphological features in detail to ferret out the most consistent and reliable features in diagnosis of CD.
Materials and Methods
Retrospective cross-sectional, observational study was undertaken in Kasturba Medical College, Mangaluru, Karnataka, India, from the archival data between January 2009 and April 2015. Only 10 cases of hyaline vascular CD were identified after studying the histomorphological characteristics. Diagnosis of hyaline vascular variant of CD based on the consensus of two pathologists was taken as inclusion criteria. Cases with reactive lymphoid hyperplasia, tumour reactive lymphadenopathy, lymphadenopathies due to infections and HIV associated lymphadenopathy were excluded from the study.
The clinical details including age, gender and lymph nodes involved were retrieved from the case files. Categorization into unicentric and multicentric disease was done based on single or multiple groups of lymphnodes involved. The tissue was processed by the routine paraffin embedding technique. Haematoxylin and eosin stained slides were studied. Histomorphological features in follicular and intefollicular regions were studied in detail. More than 50% of lymphnode occupied by follicles was taken as follicle predominant change. Stroma rich variant had more than 50% of interfollicular region in affected lymphnodes.
Follicle distribution pattern and uniformity of follicles were studied in affected lymphnodes. Germinal centre features like decreased size, increased vascularity, prominence of follicular dendritic cells and twinning of germinal centre were evaluated among lymphoid follicles. Tingible body macrophages and dysplastic follicular dendritic cells were searched in cases evaluated. Increased thickness of mantle zone with onion skin appearance was taken as broad mantle zone.
Presence of vascular proliferation and sclerosis of blood vessels were studied along with types of cells in interfollicular region. Presence of cells like plasma cells and eosinophils other than mature small lymphocytes and macrophages was taken as polymorphous population of cells. Thickening of post capillary high endothelial venules with plump endothelial cells is considered as prominent venules in inter follicular region. Hyalinised blood vessels penetrating mantle zone giving appearance of lollipop lesions were studied. Number of cases with the above mentioned features was tabulated and most constant features seen in majority of cases were taken as reliable features in hyaline vascular variant of CD.
Results
All 10 cases were of hyaline vascular subtype. Seven out of 10 cases were female. Age of presentation ranged from 17 years to 61 years. Site of presentation included cervical, inguinal and intrabdominal. Cervical lymphadenopathy was the commonest clinical presentation. Intra-abdominal cases included two in the retroperitoneum and one, subhepatic location. In cervical region, upper cervical group of lymphnodes including submandibular region was commonly involved. The clinical features are summarised in [Table/Fig-1].
Clinical details of patients with CD.
| Age | Gender | Clinical presentation | Site |
|---|
| 29 | Female | Unicentric | Abdominal |
| 28 | Female | Unicentric | Abdominal |
| 46 | Male | Unicentric | Cervical |
| 46 | Female | Unicentric | Abdominal |
| 59 | Male | Unicentric | Inguinal |
| 17 | Female | Unicentric | Cervical |
| 61 | Male | Unicentric | Mediastinal |
| 34 | Female | Unicentric | Cervical |
| 17 | Female | Unicentric | Cervical |
| 19 | Female | Multicentric | Cervical |
Nine cases had unicentric disease with swelling in single site as the only presenting clinical feature. Only one case had multicentric disease. It was a 19-year-old female presenting with massive ascites and bilateral cervical lymphadenopathy. She had raised ESR and low haemoglobin.
Six cases showed predominance of follicular abnormalities. Two cases of stroma rich variant were observed. Follicular and interfollicular abnormalities were seen in equal proportion in two cases. Morphological features observed in the present study are tabulated in [Table/Fig-2,3].
Histomorphological features observed in follicles of CD.
| Follicular changes | Number of Cases |
|---|
| Small GC* with depleted lymphocytes | 10 |
| Broad mantle zone | 10 |
| Vascular proliferation in follicles | 9 |
| Follicular dendritic cells in GC | 9 |
| Follicles in cortex and medulla | 8 |
| Uniform size of follicles | 7 |
| Twinning of germinal centre | 2 |
GC-Germinal centre
Histomorphological features observed in interfollicular region of CD.
| Interfollicular features | Number of cases |
|---|
| Increased vascularity | 10 |
| Prominent high endothelial venules | 9 |
| Admixture of polymorphous cells | 4 |
| Hyalinized blood vessels | 4 |
| Thickening of capsule | 2 |
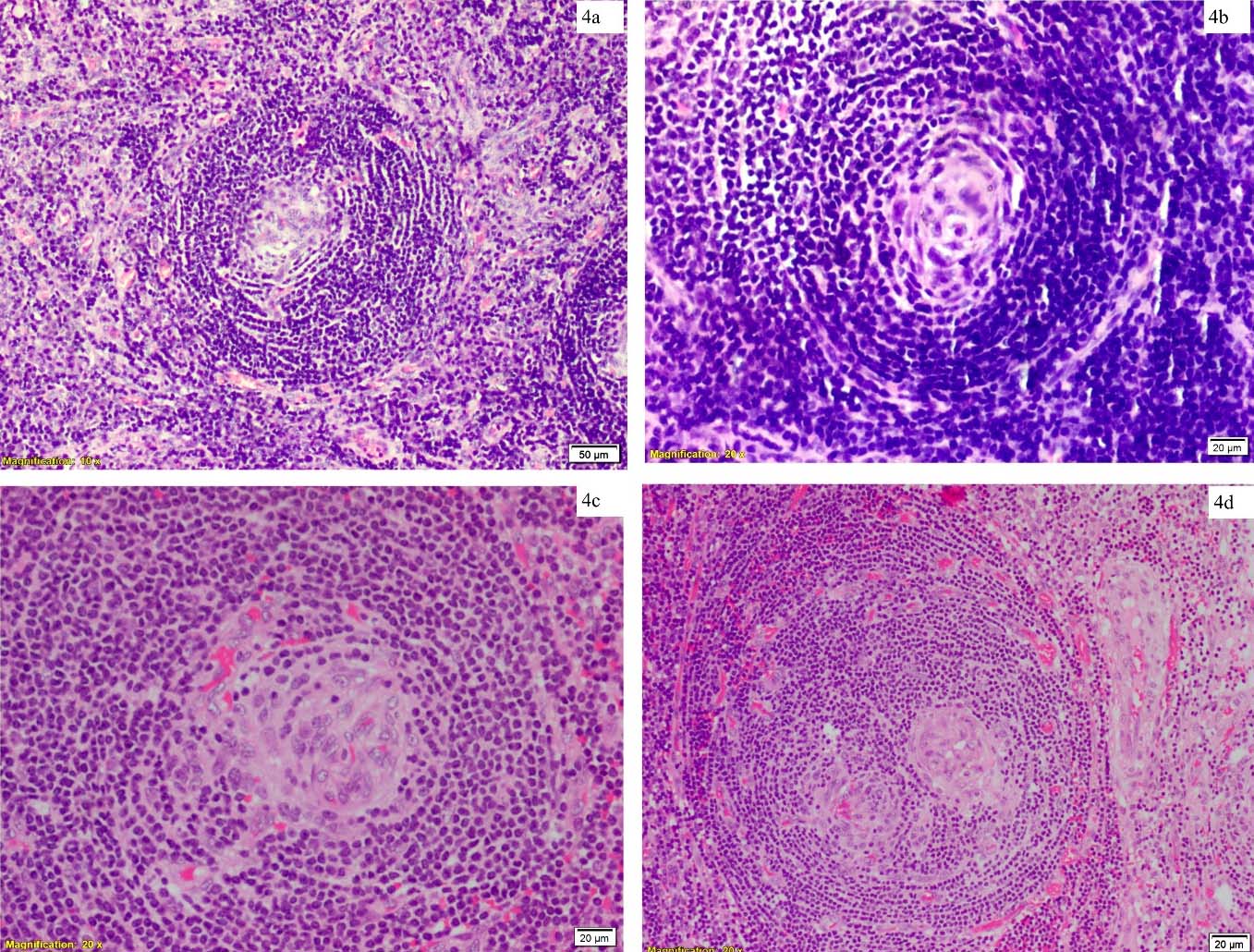
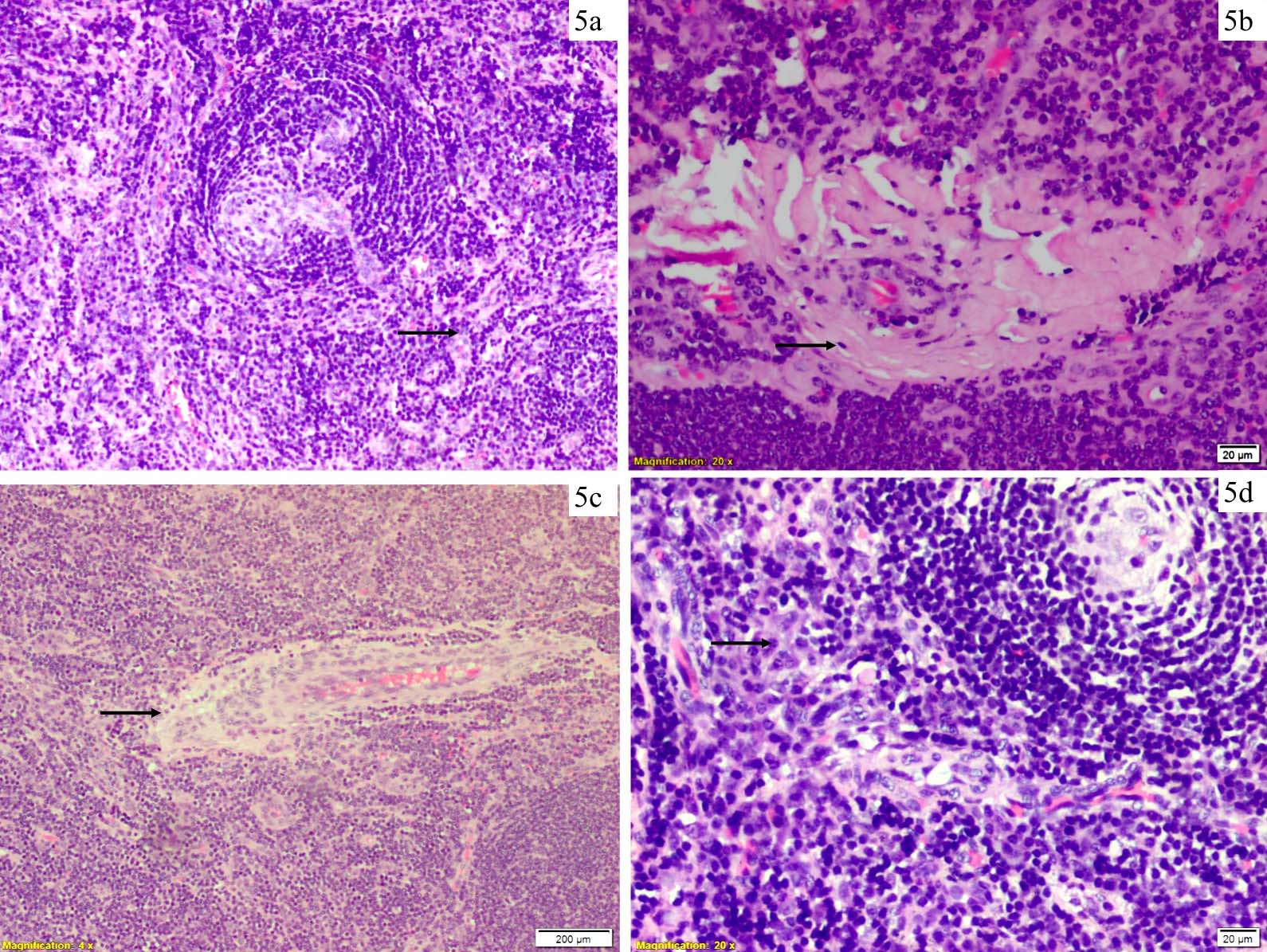
Follicular histomorphologic features like depleted germinal centre with increased vasculature and twinning of germinal centre are seen in [Table/Fig-4a-d]. Interfollicular morphological features like proliferating blood vessels, hyalinization and prominent high endothelial blood vessels are seen in [Table/Fig-5a-c].
a) Proliferating blood vessels in interfollicular region(black arrow) with germinal centre depleted follicle (red arrow) (10X H&E); b) Depleted germinal centre in follicle (20X H&E); c) Increased vasculature in germinal centre (20X H&E); d) Twinning of germinal centre (20X H&E).
a) Proliferating blood vessels in interfollicular region (10X H&E); b) Hyalinized blood vessel (20X H&E); c) Prominent high endothelial vessels (4X H&E); d) Plasma cells in interfollicular region (20X H&E).
Thickening of capsule and hyalinization of vessels was more evident in stroma rich variant. Tingible body macrophages were not evident in any of the cases studied. Lollipop pattern was relatively rare feature seen in only two cases. Dysplastic follicular cell was not seen in any of the cases studied.
Small lymphocytes were the predominant cells in interfollicular region. Plasma cells seen in two cases are shown in [Table/Fig-5d]. Eosinophil was not seen in interfollicular region.
Discussion
The most common subtype of CD is hyaline vascular variant. Unicentric disease is the commonest clinical presentation for hyaline vascular variant CD [5]. Nine out of ten cases in the present study involved localised group of lymphnodes. Predilection for females was seen with seven out of 10 cases being female in our study. Most of the studies show equal distribution among both gender [11]. Age range was broad and included young adults. However, mean age of 35 years in our study is nearly a decade less than the age mentioned in previously published articles [11].
Most of the cases in our study showed follicular and interfollicular changes in variable proportion. However, predominance of follicular changes was more noticeable. These cases showed less sclerosis of blood vessels compared to stroma rich variant. But increased vascularity in interfollicular region was uniform finding seen in all cases of hyaline vascular variant of CD [Table/Fig-4a].
Uniformity in both distribution and size of follicles was observed throughout the lymphnode in most cases with smaller germinal centre compared to that of reactive follicular hyperplasia of lymphnode, which is described in previously published data [1].
Depletion of germinal centre lymphocytes resulting in Follicular Dendritic Cell (FDC) prominence with increased vasculature was a uniform feature observed in the study [Table/Fig-4b,c]. FDC is considered to have a key role in the pathogenesis of CD. It probably plays more important role in HV-CD subtype as FDC networks are more enlarged and disrupted in contrast to normal expression in PCD [12]. Prominent follicular dendritic cell was one important feature seen in all cases. Follicular cells can be highlighted by CD21, CD23, CD35 and epidermal growth factor [1]. Dysplastic follicular cells are known to be seen in HV-CD [9]. Risk of developing neoplasm arising from follicular dendritic cells cannot be understated. Follicular cell sarcoma is seen in a known case of hyaline vascular variant of CD [13].
Duplication of germinal centre is one of the histomorphological feature seen in hyaline vascular variant of CD [10]. Twinning of germinal centre seen in two cases of our study was not a reliable feature [Table/Fig-4d]. Concentric ring of lymphocytes with onion skin appearance was a consistent feature seen in all cases [Table/Fig-4b]. Appearance of this pattern was quiet evident in all cases, being one of the first few features observed during evaluation of these cases. This feature was quiet evident even under scanner magnification. This feature of mantle zone lymphocytes is described in subset of CD cases [10].
Proliferating blood vessels were seen in expanded interfollicular region in all cases studied [Table/Fig-5a]. This turned to be one of the important consistent feature in our study. Both hyalinized and non hyalinized blood vessels were seen [Table/Fig-5b]. This was a very evident feature which is difficult to overlook. Stroma rich variant can have a nodular overgrowth of interfollicular region with proliferating blood vessels [14].
High endothelial vessels are predominant in all the cases evaluated [Table/Fig-5c]. This was one more important and consistent histomorphological feature evaluated. Hyalinization of vessels was more evident in stroma rich variant compared to cases with predominant follicular changes. Vascular endothelial growth factor is linked for the proliferation of these vessels [1]. Coincidence of CD with vascular neoplasm is seen in few case series and reports [15,16]. However, association is seen with multicentric variant of CD and Human Herpes Virus 8 (HHV8) [17]. HHV8 is a common aetiological agent for both multicentric CD and vascular neoplasm.
Small lymphocytes were predominant cell in interfollicular region with polymorphous population of cells. However, plasma cells and eosinophils were not commonly seen. Scattered plasma cells were seen [Table/Fig-5d].
Follicular hyperplasia of any cause show large follicles with prominent germinal centre and tingible body macrophages. Small germinal centre with depleted lymphocytes was one of the consistent features observed in hyaline vascular CD with increased vascularity and prominent high endothelial vessel in interfollicular region. These features are not seen in reactive follicular hyperplasia, follicular lymphoma and mantle cell lymphoma [1].
Increased association of CD, particularly multicentric cases and non-Hodgkin lymphoma has been observed [18]. Rare cases of Hodgkin lymphoma is seen in these cases. But none of our cases showed any dysplastic FDCs. However, markedly dysplastic FDCs are not to be mistaken for Reed-Sternberg cells. Immunohistochemistry has key role in such cases to differentiate CD from lymphoma.
CD can sometimes be very difficult to distinguish morphologically from HIV lymphadenitis, Hodgkin lymphoma, follicular and mantle cell lymphoma. HIV lymphadenitis, particularly in pattern C can show sclerotic follicles with vascular proliferation in the interfollicular region [1]. However, prominent features like concentric ring of lymphocytes in mantle zone and distinct follicular dendritic cell will be missing. Hodgkin lymphoma particularly the nodular sclerosis type can show prominent sclerosis and a reactive background while CD shows prominent vascular proliferation in germinal centre and interfollicular region [7]. The interfollicular vascular proliferation and depletion of germinal centre helps to distinguish from follicular and mantle cell lymphomas as well [1].
Limitation
Follow up data of these patients is not available. Immunohisto-chemistry could have been used as an adjunct to morphology to highlight the blood vessels and follicular dendritic cells. Further studies can be done to evaluate differential expression of these markers along with follow up data.
Conclusion
Follicular changes in hyaline vascular variant of CD predominate over interfollicular changes. The most reliable morphological features are small germinal centre with lymphocyte depletion, prominent follicular dendritic cells, predominance of high endothelial vessels in interfollicular region and onion skin or concentric arrangement of mantle zone lymphocytes. The first three of these histopathological features help in differentiating CD from most of the other differential diagnoses.
*GC-Germinal centre