Spontaneous Intra-Parenchymal Rupture of Craniopharyngioma – A Rare Phenomenon
Vivakaran Thanga Tirupathi Rajan1, Asogan Vaishnavi Janani2, Aiyappan Senthil Kumar3, Ilangovan Vijay Sundar4
1 Assistant Professor, Department of Neurosurgery, Saveetha Medical College, Thandalam, Kancheepuram, Tamil Nadu, India.
2 Resident, Department of Radiodiagnosis and Imaging, Saveetha Medical College, Thandalam, Kancheepuram, Tamil Nadu, India.
3 Associate Professor, Department of Radiodiagnosis and Imaging, SRM Medical College, Kancheepuram District, Tamil Nadu, India.
4 Assistant Professor, Department of Neurosurgery, Saveetha Medical College, Thandalam, Kancheepuram, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Asogan Vaishnavi Janani, Resident, Department of Radiodiagnosis and Imaging, Saveetha Medical College, Thandalam, Kancheepuram-602105, Tamil Nadu, India.
E-mail: drjananimd@gmail.com
Craniopharyngioma is a relatively benign intracranial tumour that involves sellar and supra-sellar regions. Spontaneous rupture of craniopharyngioma into the sub-arachnoid space or into the ventricles is a rare phenomenon and few cases are reported in literature. We hereby report a case of sellar-suprasellar craniopharyngioma with focal intra-parenchymal rupture into brain causing aggravation of headache in a 12-year-old female child. This complication is a relatively rare phenomenon, which requires attention for early intervention. This was managed by trans-nasal endoscopic trans-sphenoidal surgery. Usually rupture of craniopharyngioma causes chemical meningitis or it can be asymptomatic. Sometimes rupture can cause complete resolution of cyst and symptoms. In the present case, there was only focal rupture and it was into brain parenchyma causing brain oedema with aggravation of headache. Magnetic Resonance Imaging (MRI) in intra-parenchymal rupture of craniopharyngioma has been emphasized in this case report.
Chemical meningitis, Cholesterol cleft, Giant cells, Machinery oil of craniopharyngioma
Case Report
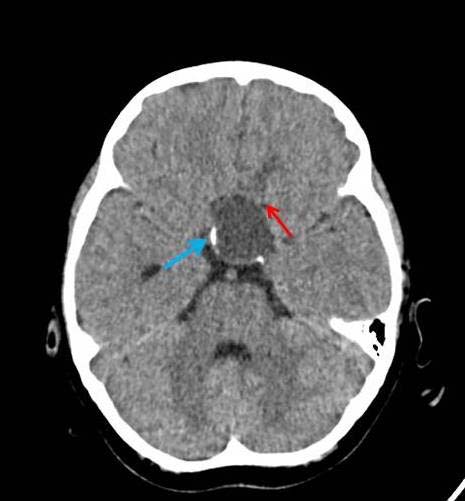
A 12-year-old girl presented with complaints of severe headache associated with vomiting for four days. She also gave a history of reduction in vision (Left>Right) and occasional mild headache of six months’ duration. She had no meningeal signs, fever nor neurological deficit. On examination, she was of short stature and Tanner Stage II [1]. Her ophthalmologic examination revealed a vision of 6/36 in the left eye and 6/6 in the right. Her lateral skull radiograph showed an enlarged sella turcica. Non-contrast enhanced CT showed a cystic lesion measuring 35 x 26 x 22 mm in supra-sellar region with presence of peripheral curvilinear calcification and oedema in left basifrontal region adjacent to cyst [Table/Fig-1]. Contrast enhanced CT revealed a larger peripherally enhancing cystic component in supra-sellar region with mild enhancement of intra-sellar solid component. T1 weighted MR imaging showed hyperintense cyst in supra-sellar location with isointense solid component in sellar location. There was also a hyperintense signal in the brain parenchyma antero-superior to cyst (left basifrontal region) [Table/Fig-2]. T2 weighted MR imaging revealed a well-defined cystic lesion in sellar-suprasellar location with oedema of left basifrontal lobe and adjacent discontinuity in cyst wall due to intra-parenchymal focal rupture of cyst [Table/Fig-3]. Compression and splaying of optic chiasma and optic tracts were also noted. The history, X-Ray, CT and MR imaging findings were suggestive of sellar-suprasellar craniopharyngioma with focal intra-parenchymal rupture of the cyst antero-superiorly into left basifrontal lobe. This rupture of the craniopharyngioma cyst intra-parenchymally causing excruciating headache is the unique presenting feature of this case.
Axial NECT showing cystic lesion measuring 3.5 x 2.6 x 2.2 cm in suprasellar region with presence of curvilinear calcification (blue arrow) with mild oedema of left basifrontal lobe (red arrow).
T1WI MR sagittal section showing hyperintense cyst in suprasellar location with isointense solid component in sellar location. Also, note hyperintense signal in brain parenchyma antero-superiorly indicating irritation from leaking cystic fluid due to intra-parenchymal focal rupture (white arrow).

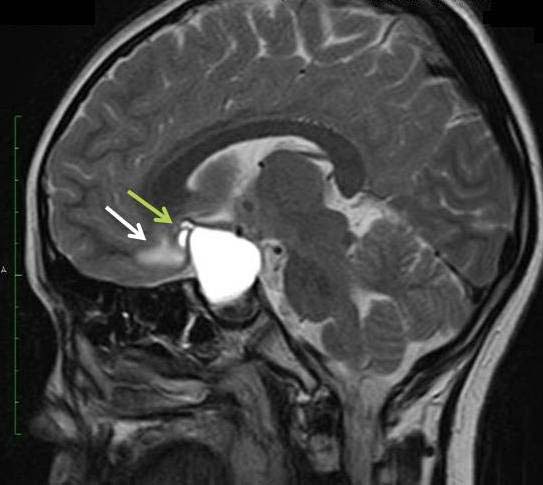
T2WI MR sagittal section showing well defined cystic lesion in sellar-suprasellar location with disruption of cyst wall antero-superiorly associated with mild oedema of left basifrontal lobe (white arrow) due to focal rupture (green arrow) antero-superiorly.
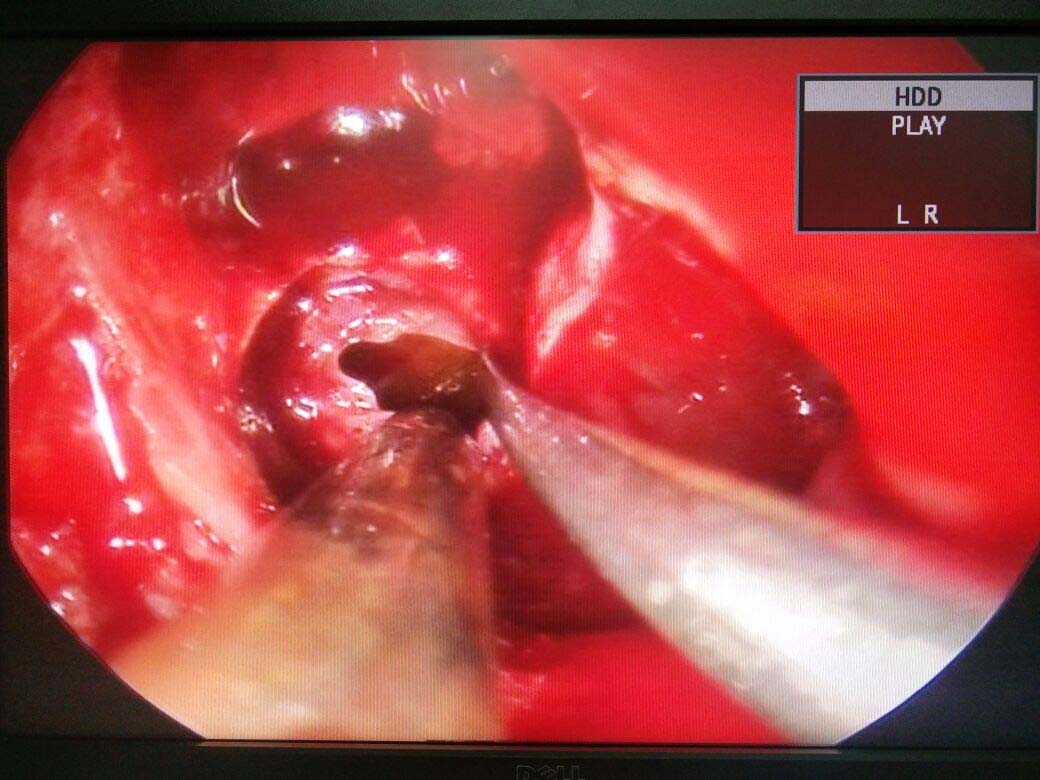
She was hospitalized and started on steroids initially. A full hormonal workup was done (prolactin - 2.54 ng/ml, cortisol - 2.50 μg/dL, growth hormone - 4.4 μg/ml, free T3 - 4.94 pg/ml, free T4 - 6.05 ng/ml) and hormonal replacement therapy was initiated. Patient underwent trans-nasal endoscopic trans-sphenoidal excision of both solid and cystic components [Table/Fig-4]. Postoperatively, the patient recovered well. On seventh postoperative day her headache subsided completely and vision of left eye improved to 6/24. Postoperative MR imaging showed resolution of brain oedema [Table/Fig-5]. The histological examination confirmed the adamantinomatous pattern of craniopharyngioma [Table/Fig-6a,b]. She was later referred to the endocrinologist for further hormonal management.
Transnasal endoscopic trans-sphenoidal approach of the lesion showing cyst filled with thick oily yellow coloured fluid of machinery oil appearance.
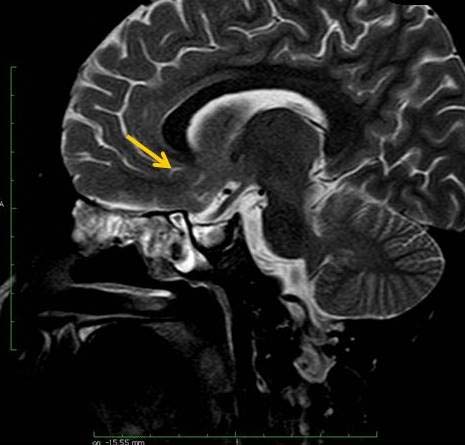
Postoperative (trans-nasal endoscopic trans-sphenoidal excision of the lesion) T2W MR sagittal section showing resolution of brain oedema (yellow arrow).
Histopathological examination (H&E Staining, x100 magnification) showing: a) Cholesterol clefts (green arrow) and fragments of reactive squamous appearing epithelium (blue arrow); b) Cholesterol clefts associated with multinucleate giant cells (green arrow) and non-caseating granulomatous inflammation (blue arrow).

Discussion
Craniopharyngiomas constitute 3%-5% of all primary brain tumours of intracranial origin. Being the most common non-glial brain tumour in paediatric age group they also constitute 50% of all supra-sellar masses in children [2]. Few cases of spontaneous rupture of craniopharyngiomas have been reported in literature. From our review of literature, using keywords “craniopharyngioma” “sellar supra-sellar” “spontaneous rupture” “chemical meningitis” in pubmed and google scholar, 26 cases have been reported on spontaneous rupture of cystic craniopharyngiomas [3-21] [Table/Fig-7].
Cases of rupture of cystic craniopharyngioma.
| Study | No. of cases, Age/Sex | Presenting Symptoms | Site | Management |
|---|
| Russel RW and Pennybacker JB [3] | 1 (67, F) | Visual disturbance | Subarachnoid space | Patient expired |
| Kaemmerer E et al., [4] | 1 (46/M) | Headache | Subarachnoid space | Conservative |
| Patrick BS et al., [5] | 1 (21/M) | Headache | Subarachnoid space | Surgical |
| Scully RE et al., [6] | 1 (60/M) | Meningism | Subarachnoid space | Conservative |
| Ravindran M et al., [7] | 1 (12/M) | Intermittent headache associated with vomiting | Intra ventricular rupture | Patient expired |
| Tokiwa K et al., [8] | 1 (43/M) | Visual field defect, transient disturbed consiousness | Subarachnoid space | Surgical |
| Okamoto H et al., [9] | 1 (17/M) | Headache | Subarachnoid space | Surgical |
| Maier HC [10] | 1 | Intermittent headache for many years | Rupture into sphenoid sinus | Radiation therapy and conservative |
| Satoh H et al., [11] | 3 | Meningism | Subarachnoid space | Surgical |
| Satoh H et al., [11] | 1 | Visual disturbance | Subarachnoid space | Surgical |
| Satoh H et al., [11] | 1 | Headache | Subarachnoid space | Conservative |
| Shinohara O et al., [12] | 1 (8/F) | Meningism, visual disturbance | Subarachnoid space | Conservative |
| Shida N et al., [13] | 1 (36/F) | Aphasia and drowsiness | Subarachnoid space | Surgical |
| Kulkarni V et al., [14] | 1 (38/F) | Personality change, behavioural disturbance, urinary incontinence, gait ataxia | (Intra-ventricular rupture)- | Surgical followed by radiotherapy |
| Takahashi T et al., [15] | 2 (70/F,69/F) | Headache, visual disturbances | Subarachnoid space | Conservative |
| Hadden D and Allen I [16] | 1 (34/M) | Headache | Subarachnoid space | Patient expired |
| John-Kalarickal M et al., [17] | 1 (61/F) | Headache, blurred vision | Subarachnoid space | Conservative |
| Yasumoto Y and Ito M [18] | 2 (4/F,47/M) | Asymptomatic | Subarachnoid space | Conservative |
| Kumar A et al., [19] | 1 (13 years old child) | Asymptomatic | Subarachnoid space | Conservative |
| Rajput D et al., [20] | 2 (17/F, 16/M) | Headache, vomiting, visual disturbances, meningism | Subarachnoid space | Surgical |
| Patnaik A et al., [21] | 1 (13/F) | Headache, loss of vision | Subarachnoid space | Surgical |
| Present case | 1 12/F | Headache, vomiting, visual disturbances | Intra-parenchymal | Surgical |
It may be asymptomatic, associated with chemical meningitis or in some cases reduction in cyst size leading to improvement of neurological symptoms. The ruptured cyst fluid has been reported to cause vasospasm causing infarction. So far no case has been reported in literature on spontaneous rupture of craniopharyngioma into brain parenchyma as seen in our case. Among the reported cases rupture of craniopharyngioma is common among adult males [11]. In our case the spontaneous rupture occurred in a female child. Patient had a history of sudden increase in severity of headache for four days prior to hospitalization which may be due to the spontaneous focal intra-parenchymal rupture of the cyst. Spontaneous rupture of craniopharyngioma into the ventricle or subarachnoid space may cause neurological deterioration. Lateral skull radiography may reveal amorphous sellar and suprasellar calcifications, sellar enlargement, dorsum sella and clinoid erosion. CT and MR imaging have complementary roles in the diagnosis of craniopharyngiomas i.e., CT is superior to MR imaging in the detection of calcification while MR imaging is superior to CT for determining tumour extent and provides valuable information about the relationships of the tumour to surrounding structures. In the present case, intraparenchymal rupture caused severe headache but no neurological worsening, this may be due to focal nature of rupture. Methods of primary treatment include radical surgery, which is gross total resection (complications are hypothalamic injury, endocrine symptoms, vasavasorium injury and pseudoaneurysm) and limited surgery which is subtotal resection along with radiation therapy. Patient had no meningeal signs. Prompt surgery and steroids relieved the headache. The parenchymal oedema resolved in the post-operative MRI indicating the clearance of the irritant. Treatment for residual or recurrent tumour includes surgery, radiation therapy or cyst aspiration, cyst instillation with intra-cavitary radioisotopes, bleomycin or other sclerosing agents. This is the first documented intraparenchymal spontaneous rupture of craniopharyngioma and prompt surgery is the logical step to reduce the parenchymal irritation and oedema, worsening of which may cause neurological deterioration.
Conclusion
We report a case of spontaneous rupture of craniopharyngioma cyst which was focal and into brain parenchyma, without chemical meningitis, which is a very rare phenomenon. This is the first documented intra-parenchymal spontaneous rupture of craniopharyngioma and prompt surgery was the logical step to reduce the parenchymal irritation and oedema, worsening of which may cause neurological deterioration.
[1]. Marshall WA, Tanner JM, Variations in pattern of pubertal changes in girlsArch Dis Childhood 1969 44(235):291-303. [Google Scholar]
[2]. Hoffman HJ, De Silva M, Humphreys RP, Drake JM, Smith ML, Blaser SI, Aggressive surgical management of craniopharyngiomas in childrenJ Neurosurg 1992 76:47-52. [Google Scholar]
[3]. Russell RW, Pennybacker JB, Craniopharyngioma in the elderlyJ Neurol Neurosurg Psychiatry 1961 24:1-13. [Google Scholar]
[4]. Kaemmerer E, Ein Fall von Spontanheilung eines craniopharyngeomsNervenartz 1964 35:42-44. [Google Scholar]
[5]. Patrick BS, Smith RR, Bailey TO, Aseptic meningitis due to spontaneous rupture of craniopharyngioma cyst. Case reportJ Neurosurg 1974 41:387-90. [Google Scholar]
[6]. Scully RE, Galdabini JJ, McNeely BU, Case records of the Massachusetts General HospitalNEJM 1980 302:1015-23. [Google Scholar]
[7]. Ravindran M, Radhakrishnan VV, Rao VRK, Communicating cystic craniopharyngiomaSurg Neurol 1980 14:230-32. [Google Scholar]
[8]. Tokiwa K, Nakayama K, Miyasaka Y, Matsumori K, Beppu T, Asao T, Cystic craniopharyngioma with spontaneous shrinkage of the cyst- Case reportNeurol Med Chir 1984 24:954-57. [Google Scholar]
[9]. Okamoto H, Harada K, Uozumi T, Goishi J, Spontaneous rupture of a craniopharyngioma cystSurg Neurol 1985 24:507-10. [Google Scholar]
[10]. Maier HC, Craniopharyngioma with erosion and drainage into the nasopharynx: An autobiographical case reportJ Neurosurg 1985 62:132-34. [Google Scholar]
[11]. Satoh H, Uozumi T, Arita K, Kurisu K, Hotta T, Kiya K, Spontaneous rupture of craniopharyngioma cysts. A report of five cases and review of the literatureSurg Neurol 1993 40:414-19. [Google Scholar]
[12]. Shinohara O, Shinagawa T, Kubota C, Oi S, Spontaneous reduction of a recurrent craniopharyngioma in an 8-year-old female patient: case reportNeurosurgery 1997 41(5):1188-90. [Google Scholar]
[13]. Shida N, Nakasato N, Mizoi K, Kanaki M, Yoshimoto T, Symptomatic vessel narrowing caused by spontaneous rupture of craniopharyngioma cyst-Case reportNeurol Med Chir 1998 38:666-68. [Google Scholar]
[14]. Kulkarni V, Daniel RT, Pranatartiharan R, Spontaneous intraventricular rupture of craniopharyngioma cystSurg Neurol 2000 54:249-53. [Google Scholar]
[15]. Takahashi T, Kudo K, Ito S, Suzuki S, Spontaneously ruptured craniopharyngioma cyst without meningitic symptoms- Two case reportsNeurol Med Chir 2003 43:150-52. [Google Scholar]
[16]. Hadden D, Allen I, Chemical meningitis due to rupture of a craniopharyngioma cystJ R Soc Med 2004 97:585-86. [Google Scholar]
[17]. John-Kalarickal JM, Carlson HE, Davis RP, Rupture of a craniopharyngioma cyst following trauma- a case reportPituitary 2007 10(1):103-06. [Google Scholar]
[18]. Yasumoto Y, Ito M, Asymptomatic spontaneous rupture of craniopharyngioma cystJ Clin Neurosci 2008 15(5):603-06. [Google Scholar]
[19]. Kumar A, Kasliwal MK, Suri A, Sharma BS, Spontaneous asymptomatic rupture of cystic craniopharyngioma in a child: Case report and review of the literatureJ Child Neurol 2010 25:1555-58. [Google Scholar]
[20]. Rajput D, Srivastva A, Kumar R, Mahapatra A, Recurrent chemical meningitis in craniopharyngioma without reduction in size of cyst: case report of two cases and review of the literatureTurkish Neurosurgery 2012 22(2):233-36. [Google Scholar]
[21]. Patnaik A, Mahapatra AK, Sarkar S, Samal DK, Spontaneous leaking craniopharyngioma causing preoperative chemical meningitisSurg Neurol Int 2016 7:41 [Google Scholar]