A Rare Case of Genital Malformation with Omphalocele, Exstrophy of Bladder, Imperforate Anus and Spinal Defect Complex-Autopsy Findings
K. Mamatha1, B. R. Yelikar2, Varsha R. Deshpande3, B. S. Disha4
1 Assistant Professor, Department of Pathology, BLDEU’s Shri B.M. Patil Medical College, Vijayapur, Karnataka, India.
2 Professor and Head, Department of Pathology, BLDEU’s Shri B.M. Patil Medical College, Vijayapur, Karnataka, India.
3 Postgraduate Student, Department of Pathology, BLDEU’s Shri B.M. Patil Medical College, Vijayapur, Karnataka, India.
4 Postgraduate Student, Department of Pathology, BLDEU’s Shri B.M. Patil Medical College, Vijayapur, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. K. Mamatha, Assistant Professor, Department of Pathology, BLDEU’s Shri B.M. Patil Medical College, Vijayapur, Karnataka, India.
E-mail: mamath2007@gmail.com
Omphalocele, Exstrophy of cloaca, Imperforate anus and Spinal defects (OEIS) is a severe manifestation of exstrophy-epispadias sequence with a combination of defects including OEIS. It results from improper closure of anterior abdominal wall and defective development of cloaca and urogenital septum due to defect in blastogenesis during the 4th week of gestation. Identification of this complex is important through foetal autopsy as this condition can recur in siblings. Prenatal diagnosis also helps to prevent foetal death with appropriate management in the less severe cases. In severe cases, termination of pregnancy is considered. A primigravida with 28 weeks of gestation had delivered a live baby with multiple congenital anomalies; baby died after 10 minutes. These anomalies were grouped under OEIS complex.
Extrophy of cloaca, Gestation, Placenta
Case Report
A 22-year-old primigravida with 28 weeks of gestation visited in the second stage of labour. There was no significant antenatal history of exposure to teratogenic drugs, infection, diabetes, hypertension and exposure to radiation. Her married life was nine years and it was not consanguineous. There was no history of treatment for infertility. Her antenatal scan during 17 weeks revealed a single live foetus without congenital abnormalities. She delivered a live baby weighing 1.16 kg at 28 weeks of gestation with multiple congenital abnormalities. The baby died after 10 minutes. There was no history of similar malformations and death of a foetus with such similar malformations in the family. The dead foetus was sent for detailed autopsy examination.
External examination showed the following: Foetus weighed 1.3 kg with attached placenta weighed 240 gm, crown-rump length – 19 cm, crown-heel length – 36 cm, head circumference – 29 cm, chest circumference – 19 cm. Placenta and umbilical artery showed normal histological features.
Congenital malformations:
A large defect in the anterior abdominal wall (omphalocele) with widened umbilical ring with a circumference of 24 cm [Table/Fig-1]
Umbilical cord was inserted at the inferior border of the sac and splitting of the cord noted
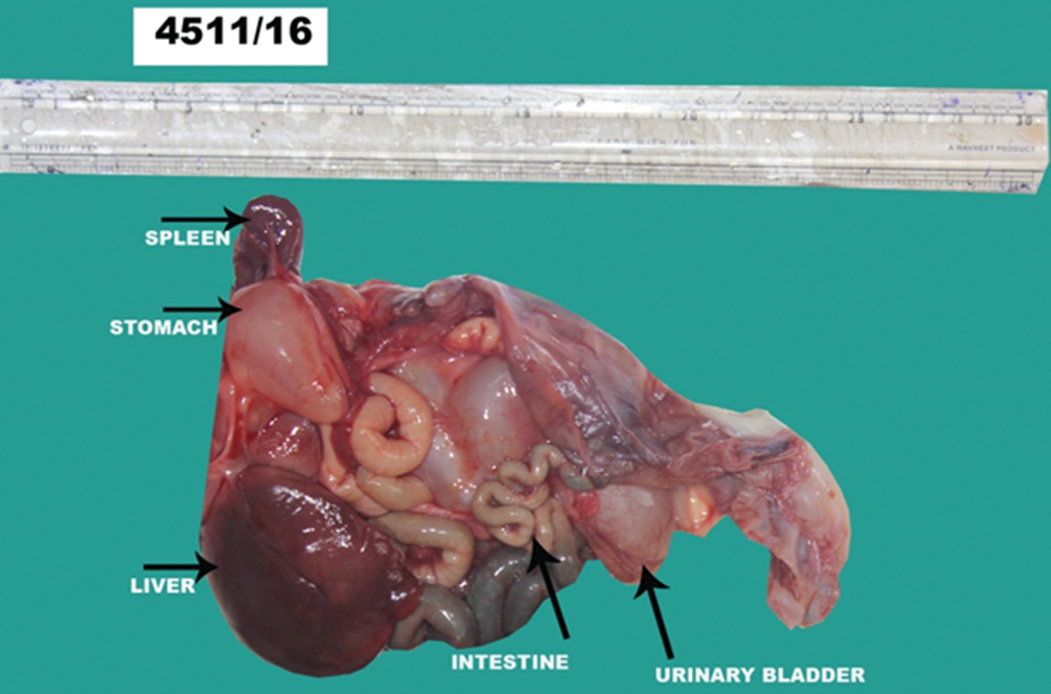
The contents of the sac were liver, stomach, spleen, right kidney with attached bladder, left kidney, pancreas, loops of intestine with dilated distal loops filled with meconium, bilateral testis [Table/Fig-2]
External genitalia was not identified except two small ridges [Table/Fig-3]
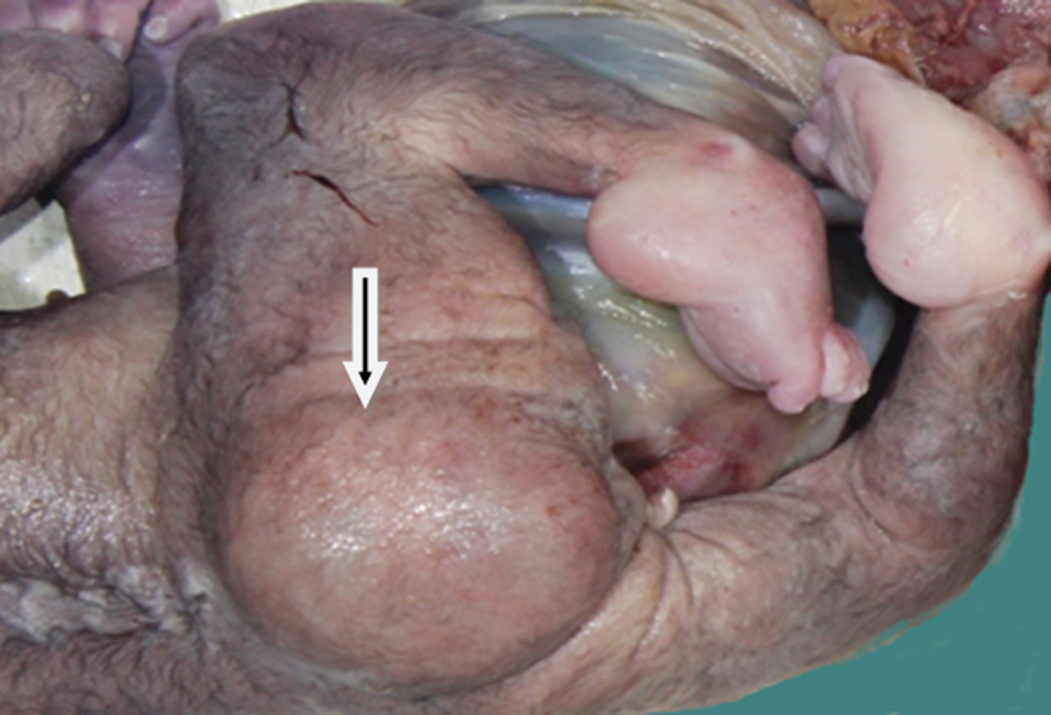
Lumbosacral meningocele measuring 7 cm in diameter [Table/Fig-3]
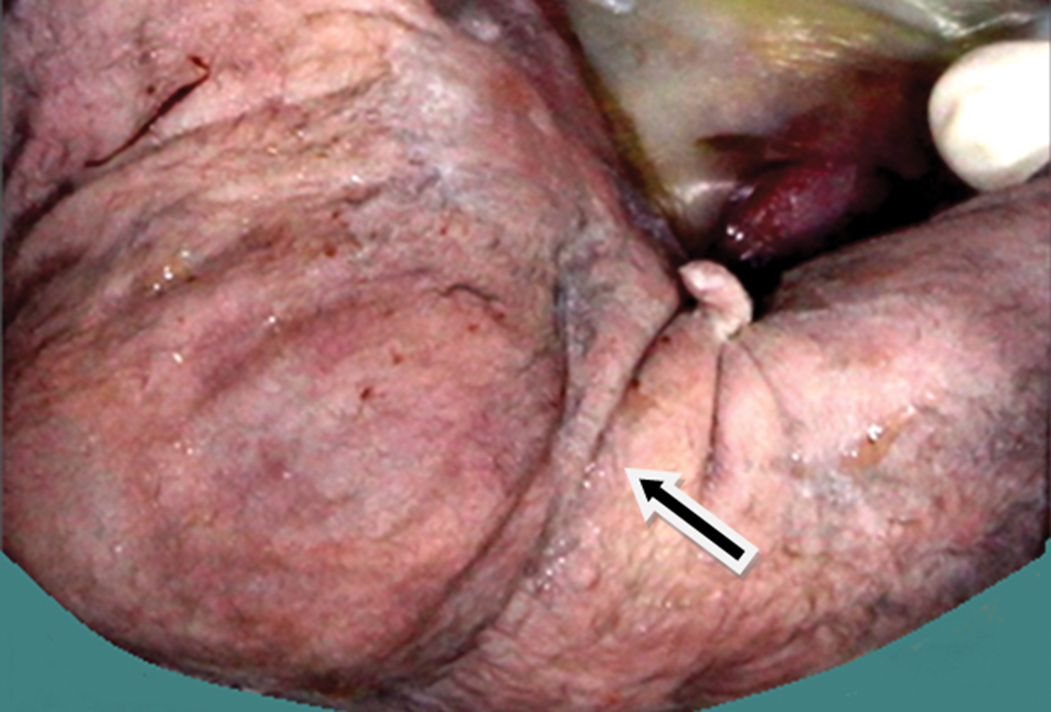
Imperforate anus with absence of genitelia – there was no anal opening in the perineal region [Table/Fig-4].
Exstrophy of bladder - anterior wall of bladder was defective.
Omphalocele: Large anterior abdominal wall defect with herniation of viscera, covered by thin amniotic membrane.

Contents of omphalocele sac.
Sacral defect. (Arrow denotes Lumbosacral meningocele)
Imperforate anus with absence of genitelia (Arrow).
Based on the presence of four cardinal anomalies diagnosis of OEIS complex was rendered.
Discussion
OEIS is a rare complex in which clustering of many common malformations occurs. It was first described by Carley et al., in 1978. It is a midline defect comprised OEIS. The incidence is one in 200,000 to 400,000 pregnancies [1,2]. OEIS complex is a severe form in spectrum of congenital defects of exstrophy-epispadias sequence, which includes phallic separation with epispadias, pubic diastasis, exstrophy of bladder, cloacal exstrophy and OEIS complex [3].
OEIS complex is a severe form of exstrophy-epispadias complex which results from improper closure of ventral abdominal wall due to failure of cephalocaudal and lateral folding with associated defects of cloaca and urorectal septum [4]. Cloaca is a phylogenetic embryonic structure and it serves as the only opening for caudal parts of digestive, genital and urinary systems. Normally during development, these separate into lower abdominal wall with bladder, intestine and anus, genital organs, pelvic bones and lumbosacral spine. OEIS complex results from developmental defects affecting the mesenchyma which is required for the development of infraumbilical mesoderm, the urorectal septum and lumbosacral somites [5]. Infraumbilical mesoderm gives rise to lower abdominal wall, genital tubercles and pubic rami. Therefore, any abnormality in mesodermal migration leads to premature rupture of cloacal membrane leading to omphalocele and exstrophy of cloaca. Genital anomalies due to the failure of fusion of genital tubercles and separation of pubic rami. Abnormalities of urorectal septum lead to failure of cloacal septation, rudimentary hindgut, persistent cloaca and imperforate anus [5].
Although OEIS is sporadic in nature with no obvious aetiology, in some cases associated chromosomal aberrations have been reported [6]. OEIS complex has been reported in siblings from different pregnancies [3]. Association of OEIS with deletion of chromosome 1p36 has been reported [5]. It has been suggested that the association of OEIS with homeobox gene such as homeobox HB9 and retinoic acid and its receptors [7].
OEIS has been reported in association with maternal exposure to diazepam, cigarette smoking, maternal obesity and uterine fibroids [5]. Lubala TK et al. reported a case of OEIS with maternal gonococcal infection in early pregnancy and foetal alcohol exposure throughout the pregnancy [8].
In the present case, there is no history of such exposure and did not have any of the risk factors. There is no similar history of malformation in the family.
Beside these cardinal malformations, OEIS complex has been reported to have other associated anomalies of central nervous system, cardiovascular system, vertebrae, upper urinary tract, malrotation, defects in vertebral column, absent appendix, lower limb abnormalities like talipes equinovalgus, single umbilical artery [4].
In the present case, four cardinal anomalies of OEIS were present along with the absence of external genitalia.
Conclusion
OEIS complex is a rare congenital abnormality with unknown exact aetiology, needs further investigation. Due to the recurrence in siblings, diagnosis is of paramount importance in the prenatal evaluation of further pregnancies. Treatment varies from appropriate perinatal management to termination of pregnancy depending on the severity.
[1]. Ben-Neriah Z, Withers S, Thomas M, Toi A, Chong K, Pai A, OEIS complex: Prenatal ultrasound and autopsy findingsUltrasound Obstet Gynecol 2007 29(2):170-77. [Google Scholar]
[2]. Mishra B, Sujani L, OEIS complex: A rare case reportJ Evol Med Dent Sci 2013 2(48):9410-14. [Google Scholar]
[3]. Smith NM, Chambers HM, Furness ME, Haan EA, The OEIS complex (omphalocele-exstrophy-imperforate anus-spinal defects): Recurrence in sibsJ Med Genet 1992 29(10):730-32. [Google Scholar]
[4]. Kar A, Kar T, Dnal I, Biswal P, Jena S, Perinatal autopsy finding in OEIS complex associated with other congenital anomaliesInt J Sci Res 2014 3(6):2039-41. [Google Scholar]
[5]. El-Hattab AW, Skorupski JC, Hsieh MH, Breman AM, Patel A, Cheung SW, OEIS complex associated with chromosome 1p36 deletion: A rare case report and reviewAm J Med Genet A 2010 152A(2):504-11. [Google Scholar]
[6]. Jyothi UA, Ramakrishna BA, Vandana K, Omphalocele, exstrophy of cloaca, imperforate anus and spine abnormalities-OEIS complex: A rare case reportJ Evol Med Dent Sci 2015 4(51):8954-57. [Google Scholar]
[7]. Keppler-Noreuil K, Gorton S, Foo F, Yankowitz J, Keegan C, Prenatal ascertainment of OEIS complex/cloacal exstrophy - 15 new cases and literature reviewAm J Med Genet A 2007 143A(18):2122-28. [Google Scholar]
[8]. Lubala TK, Shongo MY, Mbuyi SM, Mutombo AM, Ngwej T, Kabange FN, OEIS complex (omphalocele-extrophy of bladder-anal imperforation-spina bifida) and prenatal alcohol exposure: A case reportPan Afr Med J 2013 15(142):2256 [Google Scholar]