Proximal humeral fractures are the second most common fractures of the upper extremity accounting for 4% to 5% of all fractures [1]. Majority of undisplaced proximal humeral fractures can be treated with a sling immobilization and physical therapy [2]. However, approximately 20% of displaced proximal humeral fractures require surgery [3].
Conservative treatment is usually associated with nonunion, malunion and avascular necrosis resulting in a painful dysfunction [4,5].
The surgical modalities used are transosseous suture fixation, closed reduction and percutaneous fixation, open reduction and internal fixation with conventional plates, locking plate fixation and hemiarthroplasty which have shown to have mixed results [3,6]. Pre-countoured locking compression plates are fixed angled devices which prevent subsidence in the metaphyseal areas [7-9]. These plates alleviate the risk of malreduction and preserve the blood supply to the bone.
The aim of this study was to assess the functional outcome in proximal humeral fractures treated with locking plates using Neer’s shoulder score.
Materials and Methods
A prospective study was conducted on 53 patients with closed proximal humerus fractures treated with PHILOS. All the patients presenting to the emergency/outpatient department between August 2013 and August 2014 were enrolled in the study.
The inclusion criteria were skeletally matured patients with closed fracture proximal humerus with a displacement of > 1 cm and a varus angulation of >450. Severely comminuted, open fractures and valgus impacted fractures were excluded from the study.
All the necessary preoperative work-up for the patients was done in the form of haematological and radiological examinations. Well written informed consent was taken from all the patients. Prior Ethical Committee approval was obtained before commencing the study.
Surgical Technique
General anaesthesia combined with a regional block was used and a beach chair position was given to all the patients. Three doses of third generation cephalosporin were given perioperatively. A deltopectoral approach was utilized and the necessary surgical steps were followed. An 8 cm to 10 cm incision starting from corocoid process was taken along the line of deltopectoral groove. The internervous plane between deltoid and the pectoralis major muscle was identified and separated. The cephalic vein was retracted laterally or medially depending upon the exposure. The subscapularis muscle was made taut with external rotation and incised in line of its fibres. The fracture fragments were identified and the haematoma was cleared off completely. Tag sutures were taken through the rotator cuff muscles for later repair.
Preliminary reduction was done with the help of K wires and checked in both the orthogonal views. PHILOS plate (Depuysynthes® Switzerland) was applied about 5-8 mm distal to the greater tuberosity and around 2-4 mm posterior to the bicepital groove. The plate was first fixed to the distal fragment and then screws were inserted in the head as per the woodpecker technique. Final reduction was checked in both the orthogonal views. The previously tagged sutures of the rotator cuff were passed through the holes in the plate and sutured. Meticulous closure was done in all the cases. All the patients were kept in arm pouch postoperatively. Mobilization was started from postoperative day one. Similar pain management protocols were followed in all the cases.
All the patients were assessed by same orthopaedic surgeon at a regular interval of three, six and 12 months interval. Clinical assessment was done in the form of pain, function and range of movements. Antero-posterior and axial X-rays were performed for all the patients at each follow up to assess the fracture union. One patient missed the six monthly follow up but was still included in the study as he was present at 12 months follow-up.
Statistical Analysis
The qualitative variables were expressed in proportion and quantitative variables were summarized by mean and standard deviation. All the data was analysed using Epi-Info software (Version 3.5.4) and Microsoft Excel 2013 (Microsoft Office v15.0).
Results
The average age of the patient was 54.3±5.8 years. A total of 24 (45.29%) cases were males and 29 (54.71%) were females in the present study. All 31 (58.49%) cases had right sided involvement while left sided involvement was seen in 22 (41.51%) cases. Eighteen (33.96%) had road traffic accident while 35 (66.04%) cases had a fall following which they sustained the fracture. All the fractures were classified as per the Neer’s classification system which showed that there were 6 (11.32%) cases of 1-part, 19 (35.85%) cases of 2-part, 17 (32.085) and 11 (20.75%) cases of 3-part and 4-part respectively.
The average surgical duration was 94±10.2 minutes. Radiological union was seen at 12±4.6 weeks. There were 2 (3.77%) cases of varus collapse with unsatisfactory results. Union was however observed in both these patients. Both patients had limited range of movements at the terminal follow up. Three (5.66%) cases had screw back out which was later revised with hemiarthroplasty with favourable outcome. The reason for the backout could be severe comminution and osteoporosis in elderly patients. No patient had shoulder impingement.
There was one (1.89%) case of superficial infection which responded well to oral antibiotics. There were no cases of avascular necrosis seen in the present study. As per the Neer’s scoring system [Table/Fig-1], 7 (13.21%) cases had excellent results, 37 (69.81%) had satisfactory, 6 (11.32%) had unsatisfactory while 3 (05.66%) cases had poor outcome [Table/Fig-2,3,4 and 5].
| Functional |
| Pain | Scores |
| No Pain | 35 |
| Slight, occasional, no compromise in activity | 30 |
| Mild, no effect on ordinary activity | 25 |
| Moderate, tolerable, makes concessions | 15 |
| Marked, serious limitations | 5 |
| Totally disabled | 0 |
| Function |
| Strength- normal | 10 |
| Good | 8 |
| Fair | 6 |
| Poor | 4 |
| Trace | 2 |
| Zero | 0 |
| Reaching- Top of Head | 2 |
| Mouth | 2 |
| Belt buckle | 2 |
| Opposite axilla | 2 |
| Brassiere hook | 2 |
| Stability- lifting | 2 |
| Throwing | 2 |
| Pounding | 2 |
| Pushing | 2 |
| Hold overhead | 2 |
| Range of Motion |
| Flexion- 1800 | 6 |
| 1700 | 5 |
| 1300 | 4 |
| 1000 | 3 |
| 800 | 2 |
| <800 | 1 |
| Abduction 1800 | 6 |
| 1700 | 5 |
| 1400 | 4 |
| 1000 | 3 |
| 800 | 2 |
| <800 | 1 |
| Extension 450 | 3 |
| 300 | 2 |
| 150 | 1 |
| <150 | 0 |
| External Rotation 600 | 5 |
| 300 | 3 |
| 100 | 1 |
| <100 | 0 |
| Internal Rotation 900 | 5 |
| 700 | 4 |
| 500 | 3 |
| 300 | 2 |
| <300 | 0 |
| Anatomy (Rotation, Angulation) |
| None | 10 |
| Mild | 8 |
| Moderate | 4 |
| Marked | 0-2 |
| Results |
| 90-100 Points | Excellent |
| 80-89 Points | Satisfactory |
| 70-79 Points | Unsatisfactory |
| <70 Points | Failure |

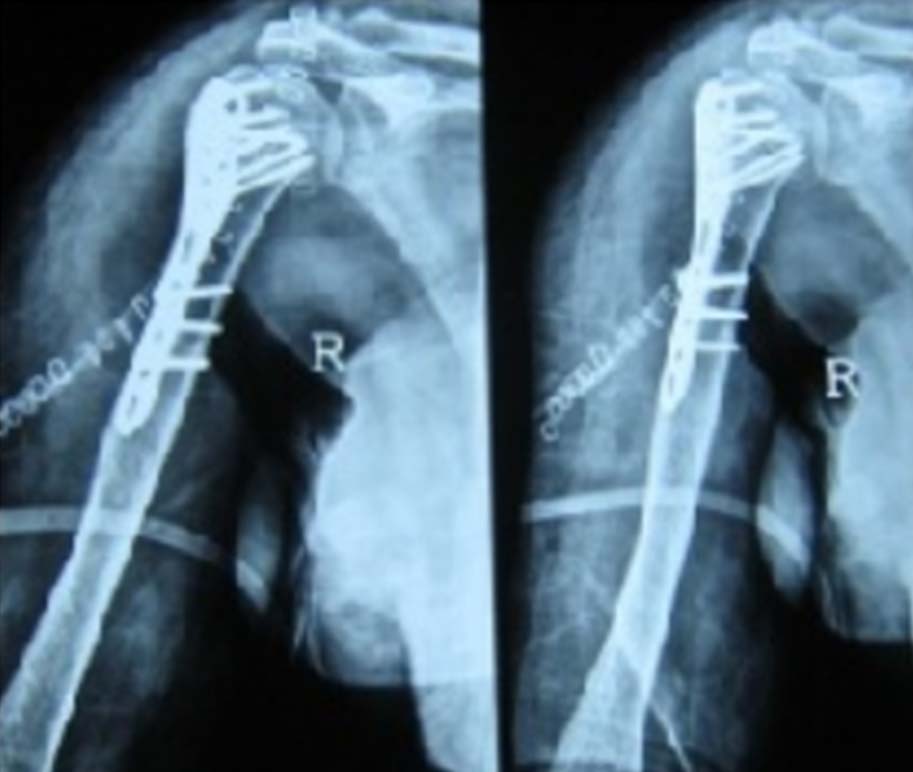
Immediate post-operative.


Discussion
Proximal humerus fractures can be one of the most devastating entities to treat. These fractures usually show a bimodal age distribution with high energy velocity injuries in younger population to trivial trauma in older age groups. Although, undisplaced fractures can be treated non-operatively with favourable outcome, fractures with intra-articular extension and severe comminution necessitate surgical fixation [9,10].
These fractures are difficult to manage conservatively owing to their anatomical location which renders bracing, ineffective. Surgical options like percutaneous K wires are associated with less soft tissue damage, less blood loss and neurovascular injury. But these techniques do not ensure stable anatomical reduction and hinders early mobilization and fracture healing. Moreover, complications like pin tract infection and delayed mobilization, further curtails the indications for this procedure [11].
Options like multiloc nailing and plating each have their own advantages and disadvantages and the debate for the superior implant continues. Nailing being load sharing devices have biomechanical superiority over plating systems. Hessmann MH et al., in their study of 160 patients over six months follow up stated that 93.7% cases had good to excellent results as per the surgeon’s view [12].
Internal fixation with non-locking plates has resulted in poor clinical outcomes and high failure rates in the past. Pre-countoured anatomical locking compression plates are more versatile with higher rates of union, especially in osteoporotic bones [13,14]. They provide more stable buttress laterally and the diverging screw options in the cancellous bone, makes them the implant of choice in complex fractures. The forces are transmitted from the bone to the screw head and then to the plate and thus these plates have a better stability than the non-locking plates. Siffri PC et al., in their cadaveric study suggested that locking plates have better torsional stability when compared to non-locking plates [15]. Second generation locking plates advocates the use of anterolateral deltoid split approach to preserve the blood supply of the humeral head, use of rotator cuff sutures, medial column stabilization and use of endosteal supports [13,15]. We had no experience with the second generation plates and deltoid splitting approach. All the surgeries executed in the present study were done using the delto-pectoral approach.
There are few complications like plate breakage, screw cut out, avascular necrosis, varusmal reduction and revision surgery associated with the use of locking plates [16,17]. Owse ley KC and Gorczyca JT in their series of 53 patients had a screw cut out rate of 23% [18]. They also stated that screw cut out is one of the most common reasons for revision surgery. The rate of screw cut out in the present study was 5.66%. This failure can be attributed to majority of the patients in elderly age group with osteoporotic bones.
Fracture geometry also plays an important role in the final outcome. Hertel R et al., in their series of 100 patients with intracapsular humerus fracture assessed the perfusion with the help of Doppler study [19]. They developed a binary description system and concluded that anatomical neck fracture, shorter calcar and disruption of the posteromedial hinge when present together has a positive predictive value for ischaemia of 97%. Avascular necrosis is another but delayed complication which occurs in three and four part fractures with severe comminution. It usually occurs years after the fixation and can cause poor functional outcomes [20,21]. Still, there are few series which shows favourable outcomes inspite of avascular necrosis [22]. There was no case of avascular necrosis encountered in the present study. Short term follow up can be one of the reasons that this complication was not seen.
Reduction of the fracture is of paramount importance in any surgery which holds true even for proximal humerus fractures. Varusreduction is one of the serious intraoperative complications which are unaccepatble as it leads to early failure in most of the cases. In the present study, difficulty in reduction was encountered in 3.77% cases which lead to varus collapse. These cases were revised with hemiarthroplasty due to severe osteoporosis. In our experience, patients with two part fractures did well as compared to three and four part fracture cases. Although, many people state that the results of hemiarthroplasty in three and four part fractures are superior to plating, recent meta-analysis deny the same [22].
Proper placement of the plate is equally important for a superior outcome in these fractures. These plates, unlike non-locking plates, are anatomically pre-countoured and thus even a slight displacement can result in shoulder impingement. The ideal position of the upper most extent of the plate is 5 mm-8 mm distal to the greater tuberosity as per the AO-OTA principles. There have been cases with shoulder impingement varying from 1.8%-8% in the literature [23-27]. In contrast to the aforementioned studies, there were no cases of impingement found in the present study, which was highly statistically significant (p<0.0001).
The average time for radiological union was 12±4.5 weeks which is comparable to the previous studies [7,17]. Final results were compared with the study by Neer [28], using the Neer’s scoring system which was statistically significant (p<0.05).
Limitation
Less sample size and short duration of follow-up remains the limitations of the study.
Conclusion
Fractures of the proximal humerus have always been perplexing. We believe that despite the associated complication rates, these plates work wonderfully in situations with severe osteoporosis and comminution. Varus reduction with a metaphyseal beak longer than 2 mm as described by Hertel have good and favourable functional outcome. Proper patient selection and thorough knowledge of the anatomy and biomechanical principles are the pre-requisites for a successful surgery.