Itolizumab in the Management of Psoriasis with Metabolic Syndrome
Shrichand G. Parasramani1
1 Senior Consultant, Department of Dermatology, Lilavati Hospital and Research Center, Bandra Reclamation, Bandra (W), Mumbai, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shrichand G. Parasramani, Senior Consultant, Department of Dermatology, Lilavati Hospital and Research Center, Bandra Reclamation, A-791, Bandra (W)-400050, Mumbai, Maharashtra, India.
E-mail: drshrichandparasramani@gmail.com
Psoriasis is a chronic, relapsing, inflammatory disease that has been associated with Metabolic Syndrome (MS), a cluster of cardiovascular risk factors mainly hypertension, obesity, diabetes mellitus and hyperlipidemia. A 49-year-old male patient presented with extensive plaque psoriasis from past 13 years. Past medications included methotrexate, PUVA therapy, topical immunosuppressants and corticosteroids. His baseline Psoriasis Area and Severity Index (PASI) score was 39.8. The patient was screened and diagnosed with MS as per Alberti’s Criteria (his waist circumference was 100 cm, blood pressure was 160/100 mmHg and High Density Lipoprotein (HDL) was 30 mg/dl). Considering severity of the disease, in this case we used anti-CD6 humanized monoclonal antibody Itolizumab (1.6 mg/kg body weight) to treat psoriasis and concurrent MS. The patient achieved PASI 50 response in six months after treatment of 10 infusions of Itolizumab (First seven doses were given every fortnightly and the last three doses every month). Further, Itolizumab treatment was continued once every three months and PASI 75 response was achieved at the end of 15 months. His PASI score increased to 30.7 after 18 months. Contemplating link between psoriasis and MS due to possibility of overlapping inflammatory pathways, we instructed patient to reduce his weight and prescribed oral tablet metformin 500 mg twice a day. After losing 6 kg weight, his PASI score came down to 22.2 at the end of 21st month. This suggests that MS was a driving factor in worsening of his psoriasis. Psoriatic patients should be checked simultaneously for co-morbid disease conditions. The report indicates direct association of psoriasis and MS.
Anti-CD6, Biological therapy, High Density Lipoprotein, Obesity
Case Report
A 49-year-old male, presented with a history of extensive plaque psoriasis since 2003. His paternal uncle also had psoriasis. The patient was non alcoholic with no tobacco addiction and a routine light exerciser. The patient had taken methotrexate, tried PUVA therapy and used several local creams and ointments in the past. He was hypertensive and on antihypertensive treatment amlodipine 5 mg daily since last eight years.
Physical examination of the patient revealed his body weight to be 79 kg, height 167 cm, BMI- 28.1 kg/m2, waist circumference 100 cm and blood pressure 160/100 mmHg. His baseline Psoriasis Area and Severity Index (PASI) score was 39.8. The laboratory parameters of the patient were analysed: Fasting Blood Sugar (FBS) level was 70 mg/dl and Postprandial Blood Sugar (PPBS) level was 95 mg/dl. Haemogram was found to be normal. Serum creatinine, blood urea, liver function tests and thyroid function tests were normal. Tests for HIV, hepatitis B and C were negative. HDL cholesterol was 30 mg/dl while the rest of the lipid profile was normal. X-ray chest and ECG were normal. Mantoux test and anti-nuclear antibody test were negative. The presence of MS was assessed in line with the 2009 consensus criteria of Alberti KGMM et al., mentioned in [Table/Fig-1] [1]. MS is considered to be present when subject presents three or more of the mentioned criteria.
Criteria for metabolic syndome and patient’s assessment results.
| Criteria for metabolic syndrome | Patient’s assessment results |
|---|
| Waist circumference | ≥80 cm for women | ≥94 cm for men | 100 cm |
| Triglycerides | ≥150 mg/dL(1.7 mmol/L) | On hypo-lipemiant treatment | Normal |
| High Density Lipoprotein (HDL) | <50 mg/dl (1.3 mmol/l) for women | <40 mg/dl (1.0 mmol/l) for men | 30 mg/dL |
| Blood Pressure (BP) | ≥130/85 | On hypertension (HT) treatment | 160/100 |
| Basal Glycaemia | ≥100 mg/dl or glucose intolerance or diagnosed DM | On hypo-glycaemiant treatment | Normal |
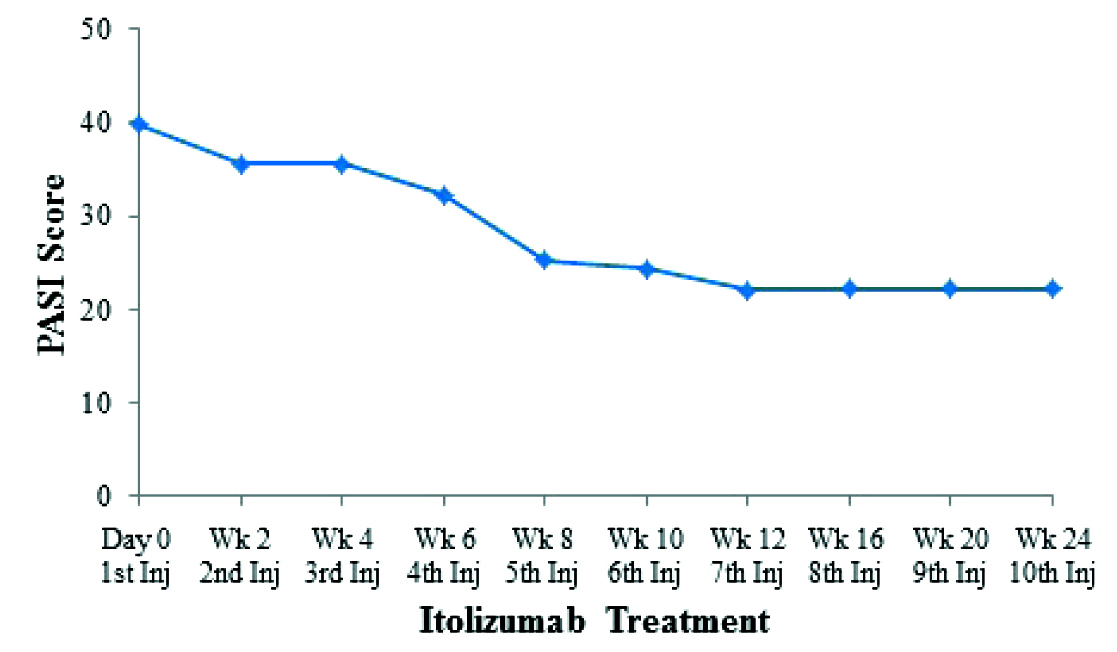
The patient was given intravenous (IV) Itolizumab 1.6 mg/kg body weight (125 mg in 250 ml of normal saline given slow IV over two hours). A total of 10 injections were given as follows: First seven doses were given every fortnightly and the last three doses every month. He was administered IV hydrocortisone 100 mg and IV pheniramine maleate 45.5 mg/2 ml vial half hour prior to Itolizumab infusion to prevent any untoward infusion reaction.
The effect of Itolizumab treatment on PASI score of a patient is given in [Table/Fig-2]. The improvement in PASI score was seen from baseline. After the 10 injections of Itolizumab, the patient attained almost PASI 50 response. Further, the patient was asked to continue the Itolizumab treatment once every three months. This resulted in the reduction of PASI score and at the end of 15 months patient achieved PASI 75 response (PASI score 12.8) [Table/Fig-3].
PASI assessment during the Itolizumab therapy.
Effect of Itolizumab therapy clinically.

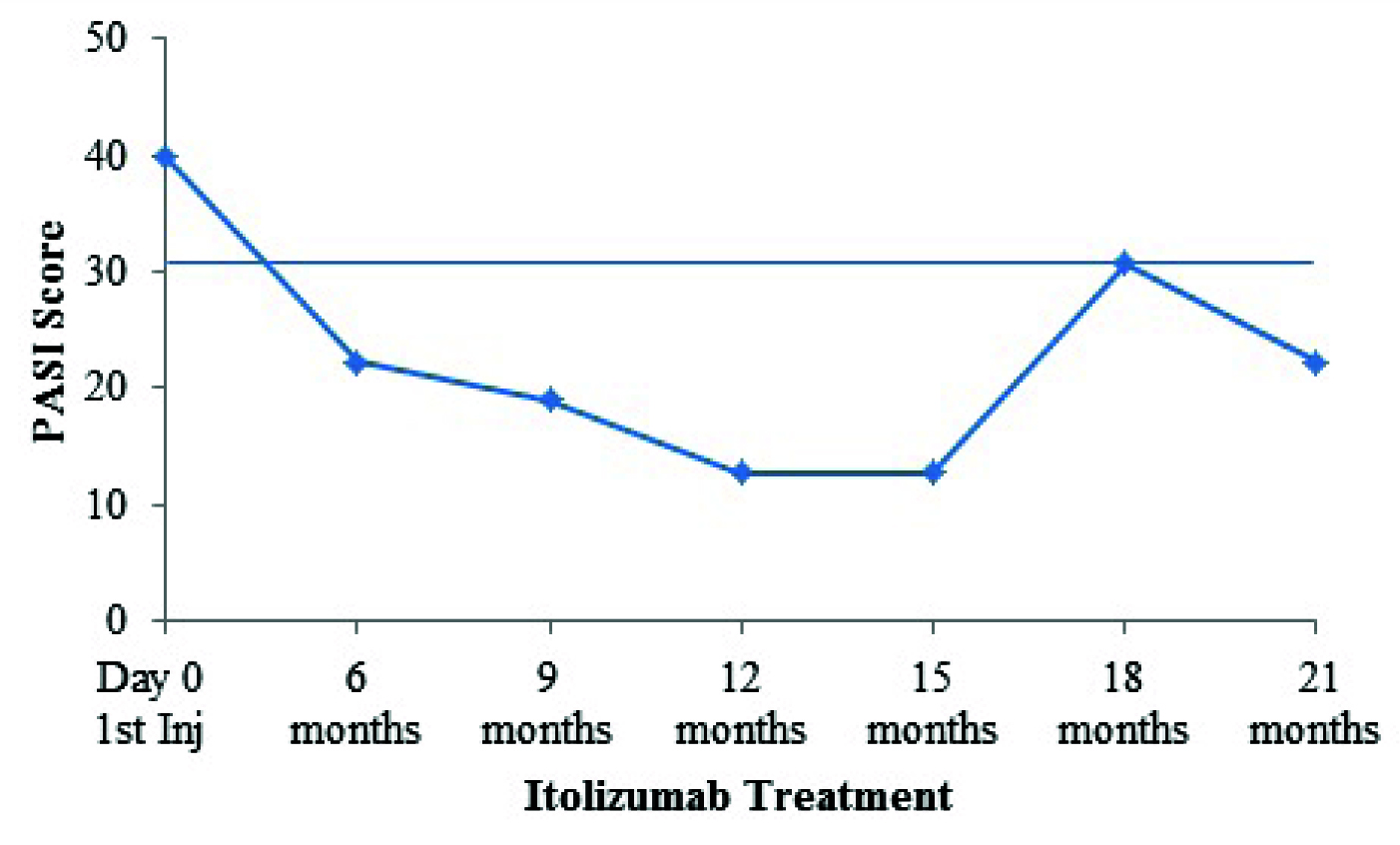
After three months his PASI score increased to 30.7, he was asked to reduce weight and was also prescribed oral metformin 500 mg tablet twice a day after breakfast and dinner respectively. Within one month (19th month) his PASI declined and became 25.5. At the end of 21st months he lost 6 kg and his PASI reduced to 22.2 [Table/Fig-4]. Recent follow up suggested that patient is maintaining PASI 75 response and continuing tablets metformin 500 mg and started calcipotriol lotion for psoriasis.
PASI assessment during the Itolizumab therapy and during the post therapy doses.
Discussion
Itolizumab is a humanized monoclonal anti-CD6 antibody which down regulates T cell activation resulting in decreased synthesis of pro-inflammatory cytokines and it also plays a vital role in decreasing T cell infiltration at sites of inflammation, a crucial step in psoriasis [2].
In the present case, improvement in PASI response was observed in the patient after Itolizumab therapy. After 10 injections of Itolizumab, the patient achieved PASI 50 response in six months. PASI 75 response was attained at the end of 15 months. Krupashankar DS et al., reported that at week 12, significant PASI 75 response was achieved in 27.0% and 36.4% in two regimens of Itolizumab as compared to 2.3% in patients who were on placebo [3]. Budamakuntla L et al., mentioned 97% improvement in PASI response after Itolizumab treatment for eight weeks in patients with chronic plaque psoriasis [4].
Psoriasis is a chronic inflammatory disease mainly characterized by activation of Th-1 and Th-17 T cells, Antigen Presenting Cells (APC’s) and Th-1 pro-inflammatory cytokines. The chronic Th-1 inflammation also plays a vital role in the pathophysiology of MS, diabetes, atherosclerosis, obesity and myocardial infraction [5]. The increased level of Th-1 cytokines, Vascular Endothelial Growth Factor (VEG-F) and adhesion molecules (e.g., ICAM-1, E-selectin) are detected in psoriasis, obesity and coronary artery disease. These inflammatory mediators have a strong impact in psoriasis and MS [6]. Recent studies showed that there is an increased prevalence of MS in psoriasis patients [7-9].
Understanding the link between psoriasis and MS due to the possible overlapping inflammatory pathways, we instructed patient to reduce his weight and prescribed metformin. As expected, after losing 6 kg, his PASI score came down to 22.2 at the end of 21st month. This suggests that proper treatment with therapies is very important in Psoriatic patients with comorbid disease profile.
Patients with MS show an inadequate response to biologics; this is more seen in fixed dosage regimens. Itolizumab is a weight based regimen hence does not suffer from this phenomenon. Saraceno R et al., mentioned that multidisciplinary approach with endocrinologists and nutritionists resulted in an improvement of MS and also psoriasis in the patient [10]. Hence, in the current case when appropriate reduction in weight occured the response to treatment improved. These results indicate that MS is a driving factor in worsening of psoriasis. Psoriatic patients should be checked simultaneously for MS. There is a possible direct association of psoriasis severity with MS. Rigorous clinical trials are required to be conducted to understand the appropriate relation between MS and psoriasis.
Conclusion
The association of MS amongst psoriasis sufferers is very high and the disease is considered as an independent risk factor for MS. After addressing the comorbid condition, Itolizumab was found to be useful in treating a case of severe psoriasis with MS.
[1]. Alberti KGMM, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of ObesityCirculation 2009 120:1640-45. [Google Scholar]
[2]. Menon R, David BG, Itolizumab – a humanized anti-CD6 monoclonal antibody with a better side effects profile for the treatment of psoriasisClin Cosmet Investig Dermatol 2015 8:217-22. [Google Scholar]
[3]. Krupashankar DS, Dogra S, Kura M, Saraswat A, Budamakuntla L, Sumathy TK, Efficacy and safety of itolizumab, a novel anti-CD6 monoclonal antibody, in patients with moderate to severe chronic plaque psoriasis: results of a double-blind, randomized, placebo-controlled, phase-III studyJ Am Acad Dermatol 2014 71(3):484-92. [Google Scholar]
[4]. Budamakuntla L, Madaiah M, Sarvajnamurthy S, Kapanigowda S, Itolizumab provides sustained remission in plaque psoriasis: a 5-year follow-up experienceClin Exp Dermatol 2015 40(2):152-55. [Google Scholar]
[5]. Griffiths CE, Barker JN, Pathogenesis and clinical features of psoriasisLancet 2007 370(9583):263-71. [Google Scholar]
[6]. Azfar RS, Gelfand JM, Psoriasis and metabolic disease: epidemiology and pathophysiologyCurr Opin Rheumatol 2008 20(4):416-22. [Google Scholar]
[7]. Zindanc I, Albayrak O, Kavala M, Kocaturk E, Can B, Sudogan S, Prevalence of metabolic syndrome in patients with psoriasisThe Scientific World Journal 2012 2012:312463 [Google Scholar]
[8]. Lakshmi S, Nath AK, Udayashankar C, Metabolic syndrome in patients with psoriasis: A comparative studyIndian Dermatol Online J 2014 5:132-37. [Google Scholar]
[9]. Ali NM, Kuruvila M, Unnikrishnan B, Psoriasis and metabolic syndrome: A case control studyIndian J Dermatol Venereol Leprol 2014 80:255-57. [Google Scholar]
[10]. Saraceno R, Ruzzetti M, De Martino MU, Di Renzo L, Cianci R, De Lorenzo A, Does metabolic syndrome influence psoriasis?Eur Rev Med Pharmacol Sci 2008 12:339-41. [Google Scholar]