Longitudinal Stent Deformation at Aneurysm Site: Flexibility at the Expense of Longitudinal Integrity
Bhupesh R Shah1
1 Associate Professor, Department of Cardiology, NHL Municipal Medical College, Ahmedabad, Gujarat, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Bhupesh R Shah, Associate Professor, Department of Cardiology, NHL Municipal Medical College, Ahmedabad-380006, Gujarat, India.
E-mail: shahbhupesh@hotmail.com
Longitudinal stent deformation is a recently described complication of percutaneous coronary intervention. Novel stents with thin struts and reduced number of fixed links between cells improve flexibility and deliverability but in certain cases it may reduce longitudinal strength and thereby increase the risk of longitudinal deformation. Although longitudinal deformation of coronary stents is an infrequent finding, it requires clinical attention as it may lead to catastrophic clinical outcomes. We report a case of longitudinal deformation of coronary stent observed at our institution while treating ostial lesion and aneurysm of left anterior descending artery. Longitudinal deformation was identified during the procedure and treated with the deployment of another stent. Three-month follow-up of the patient was found satisfactory without any incidence of stent thrombosis.
Complication, Drug eluting stent, Percutaneous coronary intervention
Case Report
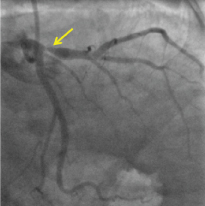
A 43-year-old male patient presented with acute onset of chest pain. His cardiovascular risk factors included current smoking and Type-2 diabetes mellitus. He was successfully thrombolysed with streptokinase as electrocardiogram showed Anterior Wall Myocardial Infarction (AWMI). Diagnostic angiography revealed single vessel disease [Table/Fig-1] with 90% discrete concentric Type B lesion at ostial Left Anterior Descending (LAD) artery followed by small ectatic segment in proximal LAD.
Coronary angiography revealed single vessel disease with 90% discrete concentric lesion (arrow) at ostial left anterior descending artery (LAD) followed by small ectatic segment in proximal LAD.
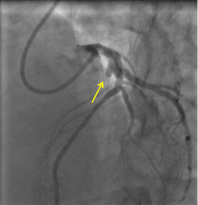
Percutaneous transluminal coronary angioplasty with deployment of stent was decided. Right radial approach was selected and was engaged with LAUNCHER 6F (EBU 3.5) guiding catheter (Medtronic Inc., MA, USA). The lesion was crossed using 0.014” Cougar XT guidewire (Medtronic Inc., MA, USA) followed by 3.5 x 33 mm stent, Pronova XR (Vascular Concept, India) deployment at 16 atmosphere pressure across the aneurysm. Post dilatation was performed using 3.5 X 12 mm NC balloon for 30 seconds at 20 atm. pressure. Post-dilation angiography revealed compression of the proximal edge of the deployed stent because of which the aneurysm remained uncovered [Table/Fig-2]. Longitudinal deformation was confirmed by the nested appearance of the struts of the proximal edge of the stent and shortening of the stent [Table/Fig-3]. To avoid occurrence of stent thrombosis or restenosis in the deformed stent as well as to cover uncovered aneurysm, we deployed another 3.5 x 13 mm Pronova XR stent (Vascular Concept, India), overlapping with the previous stent [Table/Fig-4]. There was no difficulty while overlapping another stent. Post dilatation was carried out with 3.5 X 20 mm NC balloon. Post procedural angiography demonstrated TIMI-III flow.
Post dilation angiography revealed compression (arrow) of the proximal edge of the deployed stent.
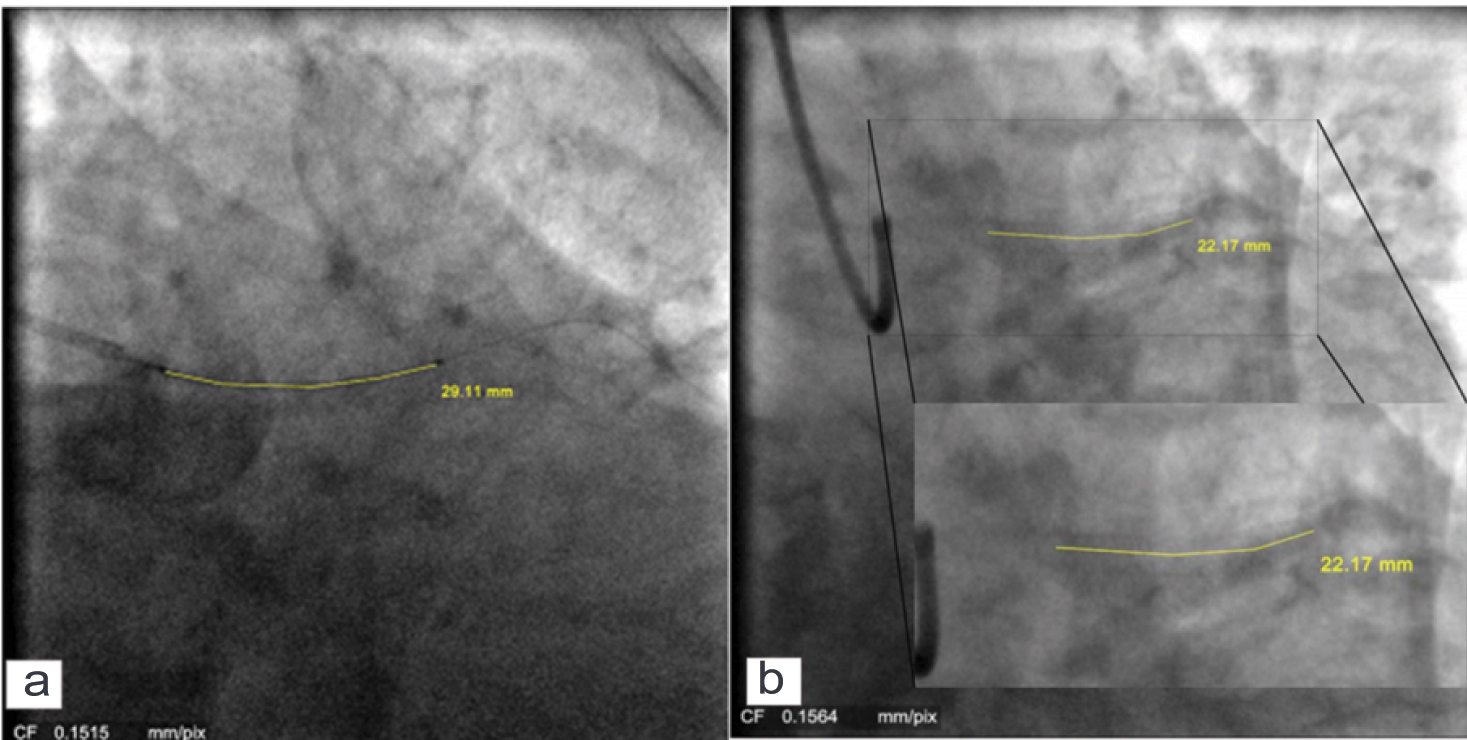
(a) Stent length before the deployment of the stent (b) Shortening of the proximal edge of the stent.
Coronary angiogram showed deployment of another stent, overlapping with the previous stent (arrow) to cover uncovered aneurysm.

The stay of the patient in the hospital was uneventful. He was discharged from the hospital after three days with double dose dual antiplatelet therapy {Clopidogrel (75 mg BD) and aspirin (150 mg OD)}. We observed satisfactory clinical outcomes (ejection fraction of 35 – 49%) with no incidence of stent thrombosis at three-month clinical follow up.
Discussion
Percutaneous Coronary Intervention (PCI) revolutionized with the advent of drug eluting stent. With innovative stent designs (thin strut and lesser number of connector) and use of novel alloys, interventional cardiologists are now able to treat more challenging lesions. The performance of the stent depends upon several other attributes i.e., recoil, longitudinal and radial strength, radio-opacity, scaffolding and trackability. There is a possibility that enhancement of one attribute may adversely affect other attributes of stent performance. The stents with thin strut and less number of connectors within cells have higher flexibility and deliverability however those are at the expense of longitudinal strength. Such stents have resistance to longitudinal stress and tend to undergo Longitudinal Stent Deformation (LSD). LSD, nesting and crushing of the stent struts into and over each other, is the result of compression applied to the struts along longitudinal axis by other device, such as guide catheters, post dilatation balloons or imaging tools [1]. The reported incidence of this rare complication of PCI is 0.2% [2]. LSD needs to be corrected as it may lead to catastrophic outcomes including intra procedural stent thrombosis [3].
LSD has recently become appreciated. However, Mamas et al., identified 57 reported cases of LSD using systemic search of the FDA Manufacturer and User Facility Device Experience Database and revealed that such complication is not new and had been previously reported as far back as 2004 [3].
Stents with less number of connectors may be prone to deformation when subjected to longitudinal compressive or elongating forces. Ormiston JA et al., performed bench test study on the longitudinal integrity of several contemporary stents. The results revealed that certain models were more likely to have less longitudinal strength than others, specifically stents with two connectors between hoops [4]. Similarly, Prabhu S et al., concluded that longitudinal integrity is the property of the number and orientation of the connectors [5]. They observed that the stents with three or more connectors have good longitudinal strength whereas stents with two connectors have poor resistance to longitudinal compression. The stent used in this case, i.e., Pronova XR, has pivoted articulation design with mid strut connectors. It has been stated previously by Prabhu S et al., that such mid strut connector geometry provides the column strength to resist longitudinal compression and obstructs the rings from nesting into each other [5]. Clinically, Pronova XR polymer-free sirolimus eluting stent system has appeared safe and effective in treatment of de novo lesions [6].
In our case, percutaneous coronary intervention was planned to treat coronary aneurysm and lesion. As there was a higher chance of restenosis with covered stent and bare-metal stent also the lesion was in left main artery, we decided to deploy drug eluting stent while considering age of patient. We deployed long stent (3.5 x 33 mm) to cover lesion as well as aneurysm. However, coronary angiography after the deployment of stent revealed uncovered aneurysm due to shortening of the stent. So, additional stenting was required to treat a coronary aneurysm in proximal-LAD that remained uncovered. We prescribed double dose dual antiplatelet therapy to avoid the risk of post procedural stent thrombosis. We also measured the stent length (off-line) before and after the procedure [Table/Fig-3] using CAAS, version 5.9.2 (Pie Medical Imaging B.V., the Netherland) and noticed remarkable shortening (6.94 mm) of the stent. Hanratty CG and Walsh SJ reported three interesting cases of this complication occurred in ostial lesions [7]. In two of the reported cases, guide catheter compression of the proximal stent edge lead to LSD whereas in third case both ends of the stent deformed as a result of intravascular ultrasound catheter. However, the complication was resolved by post dilatation of distorted stent region or by deploying an additional stent.
Conclusion
Thus, this rare and often ineludible complication of stent deformation mandates awareness, identification and careful management. Post dilatation or if necessary, implantation of additional stent should be considered for treatment. In present case, three month follow up of the patient was found satisfactory without any incidence of stent thrombosis.
[1]. Rigattieri S, Sciahbasi A, Loschiavo P, The clinical spectrum of longitudinal deformation of coronary stents: From a mere angiographic finding to a severe complicationThe Journal of invasive cardiology 2013 25(5):E101-05. [Google Scholar]
[2]. Williams PD, Mamas MA, Morgan KP, El-Omar M, Clarke B, Bainbridge A, Longitudinal stent deformation: A retrospective analysis of frequency and mechanismsEuroIntervention: journal of EuroPCR in collaboration with the Working Group on Interventional Cardiology of the European Society of Cardiology 2012 8(2):267-74. [Google Scholar]
[3]. Mamas MA, Williams PD, Longitudinal stent deformation: Insights on mechanisms, treatments and outcomes from the food and drug administration manufacturer and user facility device experience databaseEuroIntervention: Journal Of Europcr In Collaboration With The Working Group On Interventional Cardiology Of The European Society Of Cardiology 2012 8(2):196-204. [Google Scholar]
[4]. Ormiston JA, Webber B, Webster MW, Stent longitudinal integrity bench insights into a clinical problemJACC Cardiovascular interventions 2011 4(12):1310-17. [Google Scholar]
[5]. Prabhu S, Schikorr T, Mahmoud T, Jacobs J, Potgieter A, Simonton C, Engineering assessment of the longitudinal compression behaviour of contemporary coronary stentsEuroIntervention: journal of EuroPCR in collaboration with the Working Group on Interventional Cardiology of the European Society of Cardiology 2012 8(2):275-81. [Google Scholar]
[6]. Legutko J, Zasada W, Kałuża GL, Heba G, Rzeszutko L, Jakala J, A clinical evaluation of the ProNOVA XR polymer-free sirolimus eluting coronary stent system in the treatment of patients with de novo coronary artery lesions (EURONOVA XR I study)Indian Heart Journal 2013 65(4):388-94. [Google Scholar]
[7]. Hanratty CG, Walsh SJ, Longitudinal compression: A “new” complication with modern coronary stent platforms—time to think beyond deliverability?EuroIntervention : journal of EuroPCR in collaboration with the Working Group on Interventional Cardiology of the European Society of Cardiology 2011 7(7):872-77. [Google Scholar]