Atypical Presentation of Isolated Cerebral Aspergillosis in a Renal Allograft Recipient
Minaxi H Patel1, Aruna V Vanikar2, Himanshu V Patel3, Rashmi D Patel4
1 Assistant Professor, Department of Pathology, Laboratory Medicine, Transfusion Services and Immunohematology, G.R. Doshi and K.M. Mehta Institute of Kidney Diseases and Research Centre (IKDRC) - Dr. H.L. Trivedi, Ahmedabad, Gujarat, India.
2 Professor and Head, Department of Pathology, Laboratory Medicine, Transfusion Services and Immunohematology, G.R. Doshi and K.M. Mehta Institute of Kidney Diseases and Research Centre (IKDRC) - Dr. H.L. Trivedi, Ahmedabad, Gujarat, India.
3 Professor, Department of Nephrology and Transplantation Medicine, G.R. Doshi and K.M. Mehta Institute of Kidney Diseases and Research Centre (IKDRC) - Dr. H.L. Trivedi, Ahmedabad, Gujarat, India.
4 Professor, Department of Pathology, Laboratory Medicine, Transfusion Services and Immunohematology, G.R. Doshi and K.M. Mehta Institute of Kidney Diseases & Research Centre (IKDRC) - Dr. H.L. Trivedi, Ahmedabad, Gujarat, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Aruna V Vanikar, Professor and Head, Department of Pathology, Laboratory Medicine, Transfusion Services and Immunohematology and Department of Cell Therapy and Regenerative Medicine, G.R. Doshi and K.M. Mehta Institute of Kidney Diseases, Ahmedabad, Gujarat, India.
E-mail: vanikararuna@yahoo.com
The immunosuppressive state in organ transplantation leads to infectious complications responsible for high mortality rate. Fungal infections account for 5% of all infections in Renal Transplantation (RT) recipients. Aspergillus species are filamentous fungi frequently causing fungal infections in RT recipients. Lungs and paranasal sinuses are the usual portal of entry from where it disseminates to other organs. Here, we are reporting a case of 14-year-old boy with RT from mother’s kidney, who had atypical presentation of isolated cerebral aspergillosis at 19 months post-transplant without identified portal of entry. Early diagnosis and prompt treatment saved the patient and the graft.
Aspergillus, Immunosuppression, Kidney transplantation
Case Report
A 14-year-old boy presented with complains of frontal headache, vomiting, fever and ptosis of left eye since four days. He had undergone RT for End Stage Renal Disease (ESRD) of unknown aetiology with haplo-identical kidney from his mother 19 months back. He had been discharged on 8th postoperative day with Serum Creatinine (SCr) around 0.85 mg/dL on standard triple immunosuppression of tacrolimus, 0.05 mg/kg/day, mycophenolate sodium 360 mg four times a day and prednisolone, 15 mg/day. Subsequent course was uneventful. His graft function was stable with SCr around 0.9 mg/dL on tapered immunosuppression of tacrolimus, 0.03 mg/kg/day (with trough level of 4-6 ng/ml), mycophenolate sodium 360 mg three times a day and prednisolone, 5 mg/day. At seven months post-transplant, BK viremia with viral load of 10000 copies/ml was documented without any complains. Hence, he was switched from tacrolimus to cyclosporine, 3 mg/ kg BW/day. His viremia disappeared after 30 days. Graft function was fairly well maintained all along with SCr around 0.9 mg/dl.
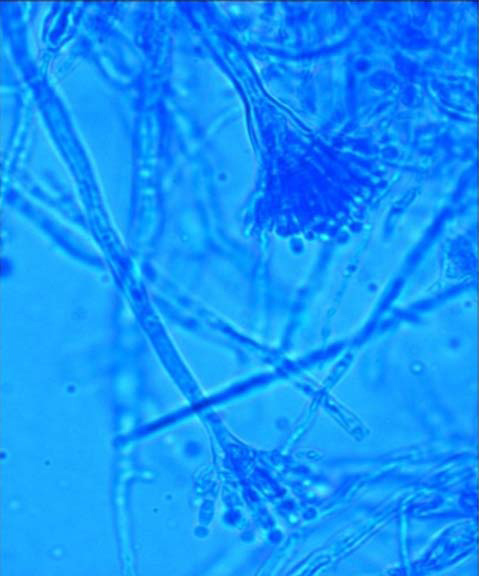
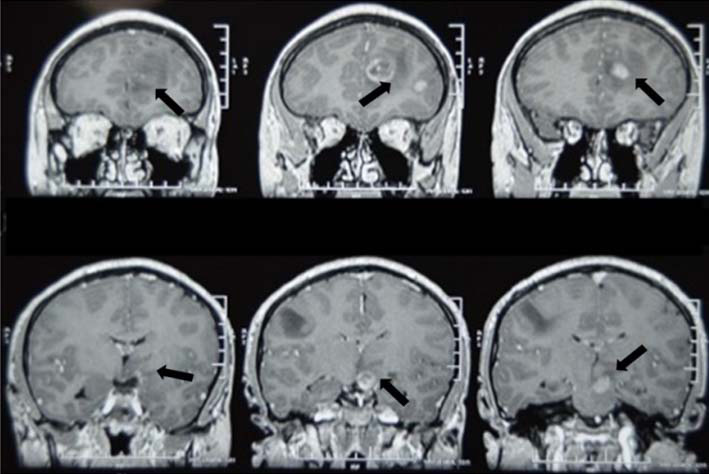
On admission, he was fully conscious and oriented with vital examination in normal range. However he was febrile with temperature of 102°F. He had mild pallor. His respiratory, cardiac and gastrointestinal examinations were unremarkable. Central Nervous System (CNS) examination revealed 3rd cranial nerve palsy affecting left eye. His chest x-ray and ultrasonography of renal allograft were unremarkable. Lab investigations revealed acute renal allograft dysfunction with SCr of 2 mg/dL, haemoglobin, 9.8 gm/dL and Total Leucocyte Count (TLC) of 12×103/μL. Urine examination showed albumin, 25 mg/dL and microscopy revealed 25-30 fresh RBCs, 3-5 pus cells and occasional granular casts per High Power Field (HPF). CSF examination revealed proteins of 53.6 mg/dL, sugar of 62 mg/dL and microscopy revealed 100 cells/HPF (mainly lymphocytes). Culture testing for aerobic and anaerobic bacteria by Bactec 9050 was sterile. Fungal culture on Sabouraud’s Dextrose Agar yielded black fluffy moulds on 4th day. This was subjected to lactophenol cotton blue preparation. Microscopy showed distinctive conidial heads with flask-shaped phialides arranged in whorls on vesicles [Table/Fig-1] very sensitive to voriconazole and amphotericin-B. Thus, the diagnosis of cerebral Aspergillosis (caused by Aspergillus niger) was established and confirmed by galactomannan antigen test with positive index of 0.69 (reference negative index: <0.5). Cryptococcal antigen test and molecular test for DNA of Mycobacterium tuberculosis (by Genexpert) were negative. MRI brain showed multiple rounded peripherally enhancing lesions in brain parenchyma involving left parafalcine frontal region, left frontal convexity, left posterior temporal region, left hypothalamic region, left half of midbrain and left cerebral hemisphere [Table/Fig-2].
Photomicrograph of lactophenol cotton blue preparation from fungal culture showing distinctive conidial heads of Aspergillus niger with flask-shaped phialides arranged in whorls, 400 x view.
MRI of brain showing multiple rounded peripherally enhancing lesions in brain parenchyma involving left parafalcine frontal region, left frontal convexity, left posterior temporal region, left hypothalamic region, left half of midbrain and left cerebral hemisphere.
Patient was treated with liposomal amphotericin-B (3 mg/kg BW/day) for three weeks and switched over to oral voriconazole, 400 mg/day for four weeks. Simultaneously mycophenolate was discontinued; cyclosporine trough level was maintained at 100 ng/mL. He became afebrile after one week, SCr decreased to 1.6 mg/dL, haemoglobin improved to 11.9 gm/dL, TLC, 9.8×103/μL and urine routine examination was unremarkable. His ptosis recovered at the end of six weeks. After six weeks MRI showed significant improvement with resolution of many granulomas.
On last follow-up at 18 months after this infection and approximately three years post-transplant, he is maintaining stable graft function with SCr of 0.86 mg/dl on triple immunosuppression of cyclosporine, 50 mg twice a day, prednisolone, 10 mg/day and mycophenolate 360 mg three times a day.
Discussion
The incidence of fungal infections is 2-5% in RT patients, and is associated with high mortality [1]. Candida, Aspergillus and Cryptococcus species are frequently isolated fungi, presenting with pneumonia, sinusitis and gastrointestinal manifestations resulting from haematogenous spread or by direct extension from paranasal sinuses [1,2].
Aspergillus species cause approximately 20% of fungal infections. An untreated invasive aspergillosis is reported to have 100% mortality [3]. Administration of steroids, anti-lymphocyte globulin, history of systemic infections like sepsis, caused by cytomegalo virus/herpes virus, renal insufficiency, anti-rejection therapy and antibiotic over-use post- transplant are the well-known risk factors for invasive aspergillosis.
Aspergillosis primarily affects the respiratory tract and nasal sinuses, and CNS involvement is usually secondary. It may spread via venous catheters, lumbar puncture, epidural anesthesia, donor-to-host transmissions via allografts, and hospital acquired infections. CNS aspergillosis starts with fungal invasion of the cerebral blood vessels progressing to ischemic and haemorrhagic infarcts, multiple abscesses in cerebrum/cerebellum/spinal cord, convulsions, mycotic aneurysms, subarachnoid haemorrhage, and/or empyema formation and progressive altered mental status [4].
Diagnostic tools include histopathological evaluation, chest x-ray, CT-scan, MRI, CSF examination, direct microscopy from clinical samples and serological detection of antigens or nucleic material of Aspergillus, or detection of antibodies in serum. Serum galactomannan assay has diagnostic value and prognostic implications. In a review of 27 patients with hematologic malignancies and aspergillosis, patients with persistently positive galactomannan results were at significantly higher risk of death and had autopsy-proven aspergillosis than those with a normalized value [5,6].
Anti-fungal treatment of invasive aspergillosis is immediately started with definite diagnosis. Liposomal amphotericin-B appears to have less adverse effects compared to conventional amphotericin. Combination of antifungal medication and surgical debridement also may be required for invasive aspergillosis [1]. The indexed patient tolerated therapy well without losing graft function.
Conclusion
We conclude that invasive CNS aspergillosis is a rare serious fungal infection in RT recipient which can be treated promptly with high index of suspicion thereby saving the graft as well as life of the patient.
Abbreviations
CSF- Cerebrospinal Fluid
CNS- Central Nervous System
ESRD- End Stage Renal Disease
HPF- High Power Field
MRI- Magnetic Resonance Imaging
RT- Renal Transplantation
SCr- Serum Creatinine
TLC- Total Leucocyte Count
[1]. Denning DW, Stevens DA, Antifungal and surgical treatment of invasive aspergillosis: review of 2121 published casesRev Infect Dis 1990 12:1147-201. [Google Scholar]
[2]. Torre-Cisneros J, Lopez OL, Kusne S, Martinez AJ, Starzl TE, Simmons RL, CNS aspergillosis in organ transplantation: a clinicopathological studyJ Neurol Neurosurg Psychiatry 1993 56:188-93. [Google Scholar]
[3]. Munoz P, Guinea J, Bouza E, Update on invasive aspergillosis: clinical and diagnostic aspectsClin Microbiol Infect 2006 12(s7):24-39. [Google Scholar]
[4]. McCarthy M, Rosengart A, Schuetz AN, Kontoyiannis DP, Walsh TJ, Mold infections of the central nervous systemN Engl J Med 2014 371:150-60. [Google Scholar]
[5]. Miceli MH, Grazziutti ML, Woods G, Zhao W, Kocoglu MH, Barlogie B, Strong correlation between serum aspergillus galactomannan index and outcome of aspergillosis in patients with hematological cancer: clinical and research implicationsClin Infect Dis 2008 46:1412-22. [Google Scholar]
[6]. Koo S, Bryar JM, Baden LR, Marty FM, Prognostic features of galactomannan antigenemia in galactomannan-positive invasive aspergillosisJ Clin Microbiol 2010 48:1255-60. [Google Scholar]