An increased demand for urbanization and generous schemes for housing have led to an acceleration of constructions all over India [1,2]. The flourishing of tier 2 cities has clenched India to the third largest construction market worldwide in recent years [3]. This has posed an increased need for sand dredging. But, the prohibition of sand dredging due to environmental disasters has constrained the use of automatized dredging resulting in shortage of sand supply [2,4]. Increased demand but less supply has amplified the problem by making sand a lucrative commodity thereby increasing the market need for manual dredgers [5].
Riverbed sand dredging provides 30%-35% of total sand required for construction [2,5]. Karnataka with its large estuaries and rivers like Cauvery, Nethravati, Swarna, Lakshmanatirtha, Harangi, Hemavathi; is one of the largest sand mining states in India. Moreover, river sand being ideal for construction is in high demand in Southwest coast of India [6-8].
Manual sand dredging involves mining of sand manually from the riverbed and transporting it to the trucks for delivery at construction sites. The job involves workers utilizing country boats and hand tools for rowing, underwater diving, dredging and manual material handling thereby increasing the risk for work-related disorders [9]. The working environment being river water and sand, there might be risk of exposure to hazardous materials [10]. Furthermore, unavailability of Personal Protective Devices (PPD) and social security measures may increase exposure to occupational hazards [11,12]. Thus, an onsite assessment of manual sand dredgers requires multisystem screening for identification of health risks.
A high demand for production, legal constraints on the use of machinery and poor working environment may pose a heightened risk for work related disorders among the manual sand dredgers. Since, it is a cluster industry in this region of Southern Karnataka and has high employee turn-over, it is necessary to identify the inherent risks involved during the task. This study is an attempt to conduct workplace screening programs for detection of health risks and occupational hazards among manual sand dredgers.
Materials and Methods
Approval to conduct the cross-sectional study was sought from Institutional Research Committee, SOAHS and ethical clearance was sought from Institutional Ethical Committee, Kasturba Hospital (IEC 616/2015). Permission was taken from dock owners to conduct the study. Written informed consent with thumb impression was obtained from all the participants in the presence of a witness. The data collection was conducted during November 2015 to January 2016.
The study was conducted in two phases. Phase-I was carried out to develop an onsite assessment schedule for the study. Phase-II included recruitment of manual sand dredgers and onsite evaluation.
Phase: I- Development of Health and Occupational Risk Profile (HORP) assessment schedule:
A literature review was undertaken to identify occupational hazards involved in divers, construction workers and manual material handlers [10,13-17]. A pilot study was conducted on 10 individuals involved in manual sand dredging in order to develop a semi-structured assessment schedule. The site for pilot study was conveniently selected from Parampalli region, Karnataka, India. The assessment schedule was compiled and then content validated by five experts. The professionals had expertise in the field of orthopaedic, neurology, cardiorespiratory and occupational health under physiotherapy discipline.
The validated HORP assessment schedule included onsite screening of the work, workplace, the worker and occupational hazards involved in manual sand dredging. It also included availability of occupational health and safety measures and awareness among the workers.
The components of HORP included screening of sensory, dermatological, ophthalmic, respiratory and musculoskeletal system. The schedule included Standardized Nordic Musculoskeletal Questionnaire (SNMQ) [18,19], Rodgers Muscle Fatigue Analysis (RMFA) [20] and Rapid Entire Body Assessment (REBA) [21] for assessing musculoskeletal disorders. To assess on-site ventilator capacity, breathe holding time and peak expiratory flow rate using Wright’s peak flow meter were utilized. Protective sensation was evaluated using 10g Semmes Weinstein monofilament. Dermatological and ophthalmic symptoms were observed by investigators. Self-reported symptoms related to ear, bladder and bowel were also recorded [Appendix].
Phase: II- Assessment of occupational hazards and health risks involved in manual sand dredging:
A time bound cross-sectional study was undertaken among manual sand dredgers. Since the river water level rises and temperature decreases during monsoon, sand dredging at Swarna river is undertaken only during pre and post monsoon seasons. Hence, a time bound study was carried out during November 2015 to January 2016, which is the post monsoon period in this region of Karnataka.
The docks owners are usually issued temporary licenses from authorities for sand mining. During the study period, eight docks were functioning near to the study area along the course of Swarna river. Three docks were randomly selected using a lottery method. The selected docks were located at Parampalli, Hoodeh and Thonse along the Swarna riverbed.
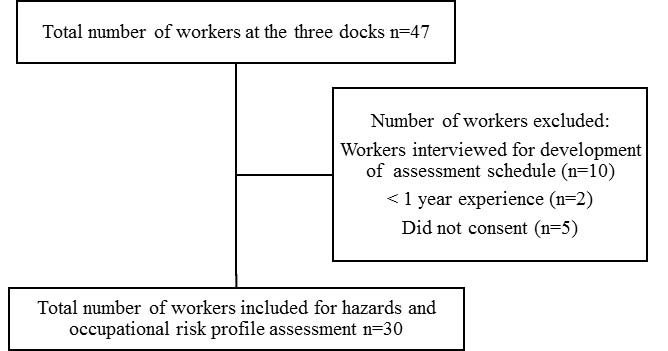
Workers with a minimum of one year experience were selected for the screening. [Table/Fig-1] shows the flow of participants for the study. The duration of administering HORP was 45 to 60 minutes per worker. Workers were not permitted to leave during work hence assessment was conducted during daybreak i.e., prior to the initiation of the work.
Flowchart showing the recruitment of participants for the study.
Statistical Analysis
The data collected on HORP was analysed using SPSS version15.0 and descriptive statistics was used to summarize the data.
Results
Thirty manual sand dredgers were purposively selected for HORP screening. The results from screening has been summarized under general demographic profile of workers; work and workplace evaluation; worker health profile; and workplace safety and security. The workplace safety and security include reports on occupational hazards and workers’ welfare provisions.
Demographics of the workers: It was observed that only male workers are involved in sand dredging. The workers were seasonal migrants from Northern states of India. All the participants were right hand dominant. [Table/Fig-2] shows the demographics and socioeconomic characteristics of participants [22,23].
Demographic and socioeconomic characteristics of the participants (n=30).
| Variables | Mean±SD |
|---|
| Age (years) | 26.8±5.7 |
| Height (feet) | 5.3±0.20 |
| Weight (kg) | 56.4±3.7 |
| Body Mass Index (kg/m2)* | 22.0±3.3 |
| Work experience (years) | 6.06±2.63 |
| Hours of work (per day) | 9.0±1.36 |
| Socioeconomic status† | 6.96±0.76 |
| Monthly income (INR) | 6976.66±465.85 |
*Belong to underweight category under WHO classification of Body Mass Index [22];
†Belong to upper-lower (IV) socioeconomic class under Kuppuswamy’s Socioeconomic Scale [23].
Work and workplace evaluation: The work was carried out by the participants only during post-monsoon season. Tasks involved in manual sand dredging include two phases. The first phase of collecting and loading the sand includes, rowing the boat to the middle of the river, diving, dredging and loading the boat with sand. The second phase includes rowing the boat to the shore and unloading the sand from the boat to the trucks. All the components of both phases of work profile was combined and categorized to rowing, diving and unloading for data analysis and presentation. Rowing included maneuvering the boat to the sand bar and back to shore. Diving included diving to river bottom, dredging the sand and loading it on to the boat. Final task was unloading, that included shifting the sand from boat to truck. All the workers were involved in continuous worker with only one macro-break provided. [Table/Fig-3] shows components of job profile for manual sand dredging.
Components of the work and workplace evaluation (n=30).
| Components | Number of participants (%) |
|---|
| Occupational regionParampalli dockHoodeh dockThonse dock | 9 (30.0)7 (23.3)14 (46.7) |
| Tasks involvedRowing Diving Unloading | 30 (100)30 (100)30 (100) |
| Working hours8-10 hours10-12 hours | 25 (83.3)5 (16.7) |
| Work schedule: Continuous | 30 (100) |
Due to high demand, limited time period and no work segregation, the participants have a continuous work schedule. Each participant had to complete all the tasks including rowing, diving and unloading. Hence, they had limited rest periods which merely included brief stops. The extraction of sand varied every day with an average of 15 to 20 trucks with approximately 10-15 tons per day. The amount was reported by the dock owners and participants.
Equipment utilized for all tasks were customized stool, customized bucket, shovel and oars. Metal stools of 330-350 cm height were used as ladders. The stool was the equipment used for diving. It was entrenched on the riverbed and the workers climbed down the stool and dug sand, using the bucket. Bucket has a metal handle and perforated bottom to help in digging and separating the sand from water. Shovels used had either wooden or metal handle and were used to transfer sand from boat to trucks.
The number of boats available at each riverbed varied. The boats owned by dock owners were 4, 8 and 5 at Parampalli, Hoodeh and Thonse respectively. However, all the boats were not used for dredging due to lack of workers. Each boat had at least three crew members for completion of first two tasks of a cycle. But as the boat reached shore for unloading, more number of workers would get involved to shift sand from boat to truck.
Worker profile: [Table/Fig-4] shows the self-reported and onsite evaluated general health profile. Respiratory and sensory systems were evaluated onsite using Mini Wright’s Peak Flow Meter and 10 g Semmes Weinstein monofilament respectively. A 3-point sensory evaluation was carried out at palmar and dorsal aspects of hands; and the sole of feet. Among all the system evaluations, sensory, dermatological and ophthalmic symptoms were most prevalent.
General health profile of the participants (n=30).
| Variables | Numbers (%) |
|---|
| Co-morbidities• Hypertension• Diabetes• Others* | 2 (6.6)08 (26.7) |
| Substance abuse• Tobacco chewing/ Smoking• Alcohol• Multiple substance abuse | 10 (33.3)20 (66.7)03 (10.0) |
| Sensory symptoms• Self-reported sensory problems• Hands Unilateral presentation Bilateral presentation• Feet Unilateral presentation Bilateral presentation• Multiple (more than two sites involved/ both hands and feet were involved) | 30 (100)03 (10.0)22 (73.4)021 (70.0)20 (66.7) |
| Trench foot (Bilateral) | 20 (66.7) |
| Dermatological symptoms• Callosities• Dermatitis/ Itching | 20 (66.7)30 (100) |
| Ophthalmic symptoms• Redness• Itching | 30 (100)4 (13.4) |
| OthersHistory of bowel and bladder discomfortEar pain/ discharge | 023 (76.7) |
| Variable | Mean ± SD |
| Respiratory system• Breath holding time (sec)• Peak expiratory flow rate (L/min) | 61.26±7.43470.16±55.65 |
*Responses included asthma, arthritis, and back pain
Musculoskeletal evaluation included pain and discomfort [Table/Fig-5], fatigue and posture evaluations [Table/Fig-6]. Prevalence of acute and chronic pain and discomfort was reported according to body segment. About 93.34% of participants complained of pain and discomfort at any of the body segments in the past 12 months. Fatigue and posture evaluation was conducted using photography and videography for tasks consuming more than 10% of daily shift. Moore JS and Garg A, had proposed an evaluation method to assess work-related strain [24]. The method used included 10% of the work cycle as the least duration for exertion. Hence, 10% was set as criteria for the study so as to include most of the tasks performed during a work cycle. The photography and videos were used afterwards to document each task, perform a direct observation and score REBA for identification of risk for musculoskeletal disorders. The three tasks identified were rowing, diving and unloading. Self-reported fatigue was only assessed for diving because videography could not be carried out.
Prevalence of musculoskeletal pain and discomfort using SNMQ (n=30).
| Region | Prevalence of pain and discomfort (%) using SNMQ |
|---|
| 12-months prevalence | 7-days prevalence |
|---|
| Neck | 19 (63.3) | 14 (46.7) |
| Shoulder | 15 (50.0) | 17 (56.7) |
| Elbow | 03 (10.0) | 10 (33.3) |
| Wrist/ Hand | 07 (23.3) | 12 (40.0) |
| Upper back | 18 (60.0) | 16 (53.3) |
| Lower back | 22 (73.3) | 21 (70.0) |
| Hips/ Thighs | 11 (36.7) | 11 (36.7) |
| Knees | 02 (6.7) | 06 (20.0) |
| Ankle/ Feet | 03 (10.0) | 05 (16.7) |
Prevalence of fatigue and postural risks (n=30).
| Tasksinvolved* | Fatigue risk using RMFA | REBA scores |
|---|
| Prevalence (%) | Priority for change | Mean±SD | Corrective measure |
|---|
| Rowing | 19 (63.3) | Very High | 11.93±1.74 | Very high risk, implement change |
| Diving | 07 (23.3) | - | - | - |
| Unloading sand | 22 (73.3) | Very High | 13.83±0.74 | Very high risk, implement change |
*Tasks performed for more than 10% of shift duration
Workplace safety and security: Mechanical, physical/thermal and chemical/biological hazards were reported by participants which have been enumerated in [Table/Fig-7]. Safety from occupational hazards through personal protective devices and availability of security schemes were also identified.
Self-reported exposure to occupational hazards (n=30).
| Variables | Number (%) |
|---|
| Mechanical• Slips/ Trips• Fall | 10 (33.4)04 (13.3) |
| Physical/ Thermal• Cold water exposure• Weather related- heat exposure | 26 (86.7)25 (83.4) |
| Chemical/ Biological• Direct contact with salty water• Accidental water ingestion | 28 (93.3)12 (40.0) |
| Workers’ Welfare provisions*• Social security schemes• Employment security schemes• Health insurances schemes• Availability of Personal Protective Devices | 15 (50.0)018 (60.0)06 (20.0) |
*Awareness about safety and security at workplace
Discussion
This study is a preliminary research on work-related disorders among manual sand dredgers. Manual sand dredging is an economic non-market activity with no fixed workplace and temporary employment [25]. The exclusive hiring of male workers was due to the tasks requiring rigorous manual material handling. The participants were seasonal migrant young adults who migrate to Karnataka when cultivation is poor in their states [26]. The participants belonged to upper-lower (IV) socioeconomic class which has been reported previously for other jobs under unorganized sectors [27,28].
Most of the workers were unaware regarding any health problems like hypertension, diabetes mellitus or any form of medication and health checkups. Co-morbidities like hypertension and lower back pain have been proved to cause work loss due to avoidance of risk exposures at work like lifting loads [29]. Workplace substance abuse among workers hamper productivity, work efficiency, general health and most importantly can cause accidents [25, 30-32]. Kumar YS et al., had conducted a study in the same geographical location on industrial workers showing 23.1% of workers involved in abusive habits with majority indulging in multiple substances [28].
Majority of the participants (73.34%) showed bilateral sensory deficit of hands however, all the workers (100%) reported of some sensory problem. Bilateral presentation of sensations symptoms of hands (73.4%) and feet (70.0%) was more than unilateral presentations. Symmetrical sensory changes in hands were probably because of bimanual repeated use of hand tools leading callosities in the hands [33]. Prolonged exposure to non-freezing cold water would have led to diminished sensation and trench feet [10]. This type of exposure causes Huntington’s response characterized by epidermal vasoconstriction but with continued long duration exposure leads to cold induced vasodilation [34].
Callosities occur as a protective response to repetitive contact stress and friction [35]. Low friction and cylindrical grip on shovel handles might have led to callosities [33]. A study on Swarna river water samples has reported increased levels of chloride reaching two times higher than permissible limits [36]. Higher chloride content may be a factor causing symptoms of dermatitis. Moreover, prolonged immersion of feet in water can alter the skin layers and sweat pattern thereby making them prone to bacterial and fungal infections [10,37,38]. These factors could have caused itching and symptoms of dermatitis [10,37-39].
A high prevalence of redness, itching of eyes and ear pain might be probably due to diving and exposures to chemicals dissolved in water [40-42]. The workers complained of increased lacrimation, itching, gravel like sensation and redness which disappeared within few hours. There was no change in visual acuity which was suggestive of mild conjunctival irritation [40]. Though the workers had no complains of bladder and bowel problems, 50 to 60 ml accidental ingestion of water was reported which may cause bowel irritations [42].
On-site respiratory evaluation on breath holding time and peak expiratory flow rate showed values within normal ranges. However, the participants involved in manual sand dredging may be at risk of diving response. Diving response occurs due to breath holding along with exposure of face to cold water. This response comprises of reduction in heart rate, peripheral vasoconstriction and an increase in sympathetic activity [43]. Consequently a detailed evaluation of the respiratory system of the participants is recommended.
Manual sand dredging involves heavy physical work, awkward postures, forceful movements, continuous work hours and substantial work demands which are established risk factors for musculoskeletal fatigue, pain and discomfort [14,44-46]. These risk factors cause micro-trauma thus resulting in pain and inflammation [20,47,48]. Low back, neck and shoulder were the most prevalent sites of musculoskeletal pain and discomfort. Postural risk analysis using REBA showed rowing and unloading as very high risk tasks requiring static muscle activity, repetitive movement and awkward posture. Static loading and repetitive activity cause lactic acid accumulation leading to micro-trauma and inflammation [49,50]. These tasks require immediate implementation of an ergonomic measure. Similar findings regarding factors influencing musculoskeletal have been reported on workers involved in manual material handling [11,13,14].
Hazards at workplace influence the efficiency and health of workers [49]. Exposures to high chloride content water and early morning drop in water temperatures were substantially reported hazards. Day time heat exposure while unloading task can cause discomfort and heat strokes [11,15]. Accidents reported were slips or trips occurring frequently while getting in or out of the boat. These slips or trips sometimes led to fall. There were no provisions for PPD during manual sand dredging at any of the docks. Lack of awareness regarding health risks and use of PPD can extensively increase the chances of occupational diseases [50,51].
None of the workers were insured nor aware regarding social security schemes. Meager health, employment and social security available to these workers expose them to immense occupational and health risks [11,12,50]. Although the dock owners have an association, the workers had no associations to represent their rights.
Subsequent to the completion of the study, workers from the three docks and the owners were given informal group education on good practices, need for health check-ups and measures for improving safety and security at work.
Limitation
The limitations of the study are a detailed system evaluation like the range of motion and all parameters of ventilation could not be included due to time and space constrains. The self-reported health problems by the participants also require medical examination for confirming any diagnosis.
Conclusion
Workplace exposure to hazards and resultant injuries have a complex multifaceted relation. This study shows a high prevalence of multiple work-related disorders and hazards involved in manual sand dredging, a highly demanding job in coastal Karnataka. Lack of health and safety measures were also identified.
*Belong to underweight category under WHO classification of Body Mass Index [22];
†Belong to upper-lower (IV) socioeconomic class under Kuppuswamy’s Socioeconomic Scale [23].
*Responses included asthma, arthritis, and back pain
*Tasks performed for more than 10% of shift duration
*Awareness about safety and security at workplace