Gastrointestinal endoscopy has been practiced for over 200 years. However, the use of endoscopy has increased due to the innovative endoscopy tools and medical methods [1]. Esophagogastroduodenoscopy (EGD) is a method for examining the upper gastrointestinal tract that is often referred to as upper endoscopy. This method is conducted with gastroscopy whereby oesophagus, stomach and duodenum (up to the third part and the fourth section) can be observed [2].
Endoscopy of outpatients is associated with an increase in patient’s anxiety. However, investigations have shown no connection between anxiety and age, gender and type of procedure [3]. Although some studies have indicated a remarkable average increase in the overt anxiety before endoscopy [4]. An endoscopist usually pays little attention to the patients’ pain and anxiety [5].
Anxiety is a serious problem in patients who are being referred to gastrointestinal clinics and diagnostic wards for endoscopy [9]. High levels of anxiety can lead to incomplete, painful, and difficult conduction of the diagnostic procedure. It may also cause an increase in consumption of sedative agents and their complications [6]. Research has indicated that pre-endoscopy anxiety is relatively high among patients, and therefore, it is recommended that serious measures be adopted in order to reduce the patients fears and concerns [9].
There are different medicinal and non-medicinal methods to modify and control anxiety. Benzodiazepines, serotonin reuptake inhibitors, and tricyclic antidepressants are sedatives that are used to reduce anxiety [10]. However, it should be stated that sedative agents are not free from harmful effects, therefore, more personnel are needed for delivering care, relieving the pain, and monitoring the patients [11].
Psychological preparation techniques can cause a reduction in hospital duration, a drop in consumption of sedative agents, improvement in temper, decrease in recovery time and recovery after surgery, and a remarkable drop in fear and anxiety before and after surgery [12,13].
The study was carried out by Pehlivan S et al., indicated that patients who had received spoken information about the process (compared to the control group and the ones who received written information) experienced less pain, felt less concern during the procedure, showed more acceptance, and finally gained remarkably lower scores of anxiety compared to the other two groups [14].
Kutluturkan S et al., investigated the effect of written materials before endoscopy on the level of anxiety. The results of that study indicated that there was a significant difference between the control and experimental groups in terms of the mean score of anxiety. The results also showed that the anxiety level in the experimental group who had received written information was significantly lower than the control group [15].
Materials and Methods
The present study was a clinical trial conducted on 98 patients who were referred to gastroenterology clinic of Ahvaz Golestan Hospital between May 2015 to September 2015. The study commenced after the confirmation of the ethical committee of Ahvaz Jundishapur University of Medical Sciences was taken. Once the inclusion and exclusion criteria were taken into account, the patients were randomly divided (using the table of random numbers) into experimental and control group, each of which included 49 patients.
Inclusion criteria: Aged between 18-80 years, Persian speaker, reading and writing literacy, verbal communication ability, no history of EGD, and consent to enter the study.
Exclusion criteria: Dementia, mental retardation, obvious physical problems, history of major psychological disorder, patient’s failure to cooperate, and excessive anxiety that prevents the patient to cooperate.
To collect the required data, the following two instruments were employed:
1) Spielberg State-Trait Anxiety Inventory which is also known as STAI [16]: It is composed of separate scales of self-assessment to measure state and trait anxiety [14].
State anxiety (state) is referred to anxiety that becomes evident in face of threat or danger. In other words, it occurs in stressful situations and disappears after the danger is gone. However, trait anxiety refers to individual differences in responding to stressful situations with different trait anxiety. STAI is composed of different self-assessment scales for measuring state and trait anxieties. State anxiety scale (Form y1, STAI) includes 20 statements which evaluate the individual’s feelings at the “moment of responding”. Trait anxiety scale (Form y-2, STAI) also includes 20 statements that measure the individual’s general and typical feelings. This inventory has no time limitation [17]. The validity and reliability of this inventory was reported 89% and 90%, respectively [18].
2) Clinical Demographic Questionnaire: This included the patients’ age, education, marital status, occupation, gender, smoking history, development of simultaneous diseases like hypertension, hyperlipidemia, diabetes, chronic renal failure, and lung disease. This questionnaire was given to the patients to be filled out upon their entrance.
Spielberg inventory was filled out by the patients twice; once when they arrived at the gastroenterology clinic for endoscopy and later, an hour before conduction of EGD (after the intervention was carried out) which revealed the level of anxiety before EGD.
After the questionnaire was completed in the first phase, the experimental group went through psychological preparation 2-3 hours prior the endoscopy. After their anxiety, information, and beliefs about endoscopy procedure were assessed in the first phase, the intervention was carried out in three areas: 1) Information control: In this stage the patients’ information was corrected, and additional information about the method of carrying out EDG, conduction time, its duration, and the general conditions of the process were explained to them; 2) Cognitive control: According to the cognitive distortions present in the patients, cognitive control was carried out for them (for example, patient’s attention to the advantages of the procedure and positive points instead of highlighting its negative and adverse aspects); 3) Behavioural control: The patients were trained by psychiatric residents for behavioural control methods including special breathing exercises, swallowing training, distraction technique, etc., so that they could use them in case of anxiety while conducting EGD. In control group, we gave them neutral pamphlets (about fruits and vegetables) without any psychological preparation.
Statistical Analysis
After the data were collected through Spielberg inventory in the two groups, descriptive statistics was employed to examine the effect of the intervention on the level of anxiety in the patients through Mann-Whitney, Kruskal-Wallis, and Chi-square tests using SPSS 17.0.
Results
The study consisted of 98 patients; 52 men and 46 women, who were equally divided into control group and experimental group (p>0.05).
There was no significant difference between the two groups in terms of clinical and demographic factors (p>0.05) [Table/Fig-1].
Showing the frequency and homogenicity of demographic and clinical factors in the two groups.
| Variables | Experimental N. (%) | Control N. (%) | p-value |
|---|
| Gender | Female | 22(44.9%) | 24(49%) | > 0.05 |
| Male | 27(55.1%) | 25(51%) |
| Smoking | Smoking | 15(30.6%) | 10(20.4%) | >0.05 |
| Non-smoking | 34(69.4%) | 39(79.6%) |
| Marital Status | Married | 7(14.3%) | 12(24.5%) | >0.05 |
| Single | 41(83.7%) | 37(75.5%) |
| Divorced | 1(2%) | 0(0%) |
| Education | Under diploma | 14(28.6%) | 13(26.5%) | >0.05 |
| Diploma | 22(44.9%) | 28(57.1%) |
| Associate’s degree | 4(8.2%) | 1(2%) |
| Bachelor’s degree | 6(12.2%) | 6(12.2%) |
| Above bachelor’s | 3(6.1%) | 1(2%) |
| Occupation | Unemployed | 27(55.1%) | 28(57.1%) | >0.05 |
| Employed | 22(44.9%) | 21(42.9%) |
| Medical history | Hypertension | 4(8.2%) | 0(0%) | >0.05 |
| Hyperlipidemia | 5(10.2%) | 4(8.2%) |
| Lung disease | 3(6.1%) | 1(2%) |
| Renal disease | 0(0%) | 4(8.2%) |
| No history | 32(65.3%) | 36(73.5%) |
| Hypertension and Hyperlipidimia | 2(4.1%) | 1(2%) |
| Hypertension and Renal disease | 1(2%) | 1(2%) |
| Hyperlipidimia and Renal disease | 1(2%) | 0(0%) |
| Hypertension, Hyperlipidimia and Renal disease | 1(2%) | 2(4.1%) |
There was no significant difference between the two groups in terms of the level of their state and trait anxiety before the study (p>0.05) [Table/Fig-2].
Comparing the state and trait anxieties in the two groups before the study.
| Dependent Variable | Independent Variable | Group | N. | Mean | SD | p-value |
|---|
| State anxiety | Intervention | Experimental | 49 | 2.90 | 1.046 | 0.794 |
| Control | 49 | 2.92 | 0.932 |
| Trait anxiety | Intervention | Experimental | 49 | 2.69 | 0.940 | 0.343 |
| Control | 49 | 2.84 | 0.825 |
The mean score of state and trait anxieties in the experimental group was significantly lower than that of the control group, which indicates the effect of the interventions [Table/Fig-3].
Comparing the state and trait anxieties in the two groups after the study.
| Dependent Variable | Independent Variable | Group | N. | Mean | SD | p-value |
|---|
| State anxiety | Intervention | Experimental | 49 | 2.10 | 0.984 | <0.001 |
| Control | 49 | 2.80 | 0.935 |
| Trait anxiety | Intervention | Experimental | 49 | 2.39 | 0.931 | 0.004 |
| Control | 49 | 2.90 | 0.872 |
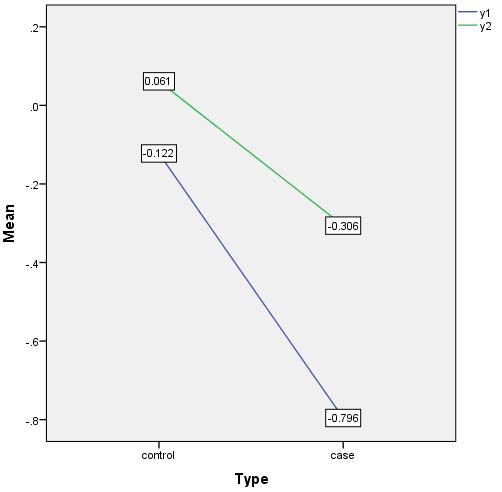
The p-value for state and trait anxieties was <0.001 and 0.004, respectively. This shows that even though the two variables have plummeted, there was a greater reduction in state anxiety.
In other words, the effect of intervention was more noticeable on the state anxiety (which is indicated in [Table/Fig-4]). For instance, the number 0.061 in the trait anxiety (y2) control values have been calculated by subtracting the values of the trait anxiety control values, before and after the intervention. (2.898-2.837=0.061). This means the average of the anxiety before intervention minus the after intervention have been considered for the trait anxiety control values.
The effect of the intervention was more on state then trait anxiety (y1: anxiety state, y2: anxiety trait).
The results of the study showed that the intervention had a significant effect on reducing anxiety.
According to the results of the study, only the trait anxiety before intervention had significant difference with age and occupational status (p<0.05) [Table/Fig-5,6]. Hence, in order to examine the effect of these two variables on the level of state anxiety after the intervention, a logistic regression model was utilized, which indicated that only occupational status influenced the level of state anxiety post intervention. In other words, the unemployed individuals had a generally higher level of state anxiety after intervention compared with their employed peers. That being said, although the level of state anxiety in unemployed patients had also significantly decreased like other patients, yet they generally had a higher level of state anxiety in comparison with the other patients.
Anxiety level in term of employment status.
| Dependent variable | Independent variables | Group | N | Mean | SD | p-value |
|---|
| State anxiety | Employment | Unemployed | 55 | 3.18 | 0.964 | 0.002 |
| Employed | 43 | 2.56 | 0.908 |
| Trait anxiety | Employment | Unemployed | 55 | 2.89 | 0.896 | 0.130 |
| Employed | 43 | 2.60 | 0.849 |
Anxiety level in term of gender.
| Dependent variable | Independent variable | Group | N | Mean | SD | p-value |
|---|
| State anxiety | Sex | Male | 52 | 2.69 | 0.897 | 0.018 |
| Female | 46 | 3.15 | 1.032 |
| Trait anxiety | Sex | Male | 52 | 2.63 | 0.864 | 0.088 |
| Female | 46 | 2.91 | 0.890 |
The results of the study also indicated that the decrease level of anxiety (y1 and y2) had no relationship with age, gender, occupational status, education, occupation, and smoking history (p>0.05). There was only a slightly significant relationship between decrease and previous medical problems, in that patients who were simultaneously suffering from three diseases of hyperlipidemia, hypertension, and renal disease experienced a higher reduction in the level of their anxiety (p=0.041).
Discussion
The present study was carried out to examine the effect of psychological preparation on the level of anxiety among patients before endoscopy. The results indicated that psychological preparation caused a reduction in trait and state anxiety in patients. This finding is in line with other studies conducted on psychological preparation on patients before endoscopy [14,15]. Similar findings were also reported in some other studies which investigated the effects of written information about the process [15] and other non-medicinal methods like relaxing music [18] on the level of anxiety in patients subjected to other invasive procedures.
In a study conducted in 2015, psychological preparation was carried out through informational, behavioural and cognitional methods, and it was concluded that such methods reduced the level of anxiety in patients before coronary artery bypass grafting [19].
Contrary to our study, in a study in 2014 on patients in need of Coronary Artery Bypass Grafting (CABG), use of relaxation methods was not effective in lowering anxiety [20]. In that study, relaxation was the only utilized method while in the present study cognitive and behavioural methods along with information control were employed. It is recommended that different intervention methods get separately and simultaneously examined and be compared with control groups in future studies in order to determine the effect of each method.
In the present study, there was a significant decrease in the level of state and trait anxiety in the experimental group. This decrease was greater for state anxiety. This can be attributed to the fact that state anxiety increases in response to stressful situations [17] and it is expected that it drops as a result of psychological preparation before endoscopy. Reduction in trait anxiety can be due to response to cognitive and behavioural interventions. It is recommended that each method and their effects on state and trait anxieties be separately investigated. It seems that trait anxiety could benefit from lengthening cognitive interventions.
The results of the present study proved no significant relationship between demographic factors and the efficacy of psychological interventions. Only a slight increase was observed in the effectiveness of the interventions on patients with the three diseases of hyperlipidemia, hypertension, and renal disease. These patients were already facing psychological, social, and economical problems and required more psychological interventions. Thus, the interventions from the present study caused a more noticeable decrease in their anxiety. It is recommended that this issue be more precisely investigated in later studies. As the study carried out by Cald Well PH et al., revealed women had more stress than men about the surgery [21], the results of the present study also showed that women had a higher level of state anxiety compared to men; however, it was observed that this increase had no effect on the level of post-intervention anxiety. Therefore, it is suggested that this issue be investigated with larger samples.
The results of the present study indicated that there was no relationship between initial level of anxiety and demographic and clinical factors. Only unemployed patients, compared to employed ones, had a higher level of anxiety (independent of the intervention). In other words, unemployed individuals have a higher level of state anxiety, and all other variables remained constant which can be due to spiritual pressures caused by unemployment and financial problems. It is also possible that this is caused by their fear of the result of endoscopy and diagnosis of disease which could need expensive medicine with high costs. It is suggested that this issue be further investigated in future studies.
Limitation
All of the participants were literate, and no illiterate patient was selected for the study. Individuals with major psychological problem were not included in the study. The effect of cognitive, information, and behavioural interventions were not separately examined. The intervention period was short.
Conclusion
The result of this study showed that psychological preparation and intervention before endoscopy can decrease the patients’ anxiety.
Endoscopy is an invasive procedure that may increase anxiety and cause problems for patients undergoing this procedure. Thus, it is recommended to provide the endoscopic department with trained endoscopists and nurses or make sure that a psychologist attends the medical team.