Environmental contaminants including toxic metals are of crucial importance due to their bioaccumulation properties in human body [1]. In Iran, contamination of rice consumed by households with toxic metals including lead, cadmium [2,3] and arsenic [4] has been proven. Among the complications of long-term usage of Rice Contaminated With Toxic Metals (RCWTM) are cancer, damage to lungs, liver, and nervous system [5,6]. On the other hand, due to high consumption of rice (45 kg per person per year) [7,8], modification of food habits is effective in reducing the mortality caused by unhealthy diet among people [9]. Therefore, using environmental interventions to enhance people’s knowledge of selecting healthy foods [10] and reducing the consumption of rice contaminated with toxic metals seems to be essential [11]. Educating people to follow a healthy lifestyle is a fundamental need in formation of preventive behaviours against diseases [12].
In ECO, the relationship between individuals, social, and environmental factors and a healthy diet has been proven [19]. ECO considers behavioural change at various levels including intrapersonal, interpersonal, and organizational levels. At interpersonal level, this model takes the effect of social support and social networks on behavioural change into consideration [20]. Lack of social support is the most important barrier for changing food habits, weight reduction, healthy diet, and healthy lifestyle [21,22]. Further, there are experimental evidence supporting the predictive role of social support in enhancing consumption of fruits and vegetables [23], and behaviours of reducing fat consumption [24]. However, few studies have been conducted to investigate whether ECO model have been more successful or HBM model in encouraging people to follow a healthy diet.
On the other hand, considering the role of women in families and their impact on application of educational- health patterns [25], it was assumed that development of social network and paying attention to the role of family members, friends, and colleagues may have a more effective role in encouraging the consumption of Rice Free From toxic Metals (RFFTM) as compared with individual-based model (HBM). Testing this hypothesis will follow identification of solutions for enhancing the efficiency of nutrition interventions.
We filled the gap of previous studies through testing the efficiency of these two six-month interventionist models to see which one underlies better improvement of diet among Iranian women in comparison with control group.
Materials and Methods
This study was an environmental instructional interventionist program based on HBM and ECO models with the purpose of improving the Performance Of Rice Consumption (PORC) among Iranian women aged 18-50 years responsible for cooking in the city of Ilam, Iran. Participants of HBM and control groups consisted of people supported by clinics and employed women were selected for the ECO group.
Before the administration of the questionnaires, the study procedure was explained for the participants succinctly. In order to obtain the probable level of women’s knowledge about the consumption of RCWTM, 30 people who had the characteristics of the target population were investigated through the questionnaire; accordingly, the level of knowledge was obtained to be 30%. Considering α=0.05 and β=20% and the minimum expected development of the knowledge following the intervention as 20%, the number of participants for each group (HBM, ECO, and Control) was obtained to be 80 in each group.
Considering the sampling method for the HBM and control groups, eight clinics were chosen through random sampling out of 13 healthcare centers in city of Ilam. In every center, two ten-household clusters (one cluster as the HBM group and another cluster as the control group) were chosen randomly. Next, using the file number of the households in healthcare centers, the cluster heads were selected. For the ECO group, six organizations were chosen randomly out of 12 organizations in the city of Ilam. After determining cluster heads in HBM and control groups along with the organizations in the ECO group, the people were invited to participate in educational sessions. The questionnaires were administered among participants whose consent was obtained as an initial evaluation. The protocol of the interventionist program was approved at the research center of water and foods in Kurdistan University of Medical Sciences.
Data Collection
Data collection was performed in two stages: before the intervention (December 2014) and after a period of six-month intervention (June 2015) rice consumption performance included changes in the frequency of consumption of Local Rice (LR), harvested in farms of Ilam city, Foreign Rice (FR), imported to Iran, Mixed Rice (MR), a mixture of LR and FR, (no consumption, 1-3 times per week, and 4-7 times per week respectively), and changes in the manner of cooking from Kateh (steaming rice) to Pilaw (draining rice).
Instrument
The instruments in the HBM model was a researcher-made questionnaire consisted of four sections (demographic information, knowledge, the constructs of HBM model and PORC). The instrument utilized in ECO model was also a researcher-made questionnaire consisted of four sections (demographic information, knowledge, the social support construct, and PORC).
Knowledge: This section had seven questions for measuring knowledge about toxic metals, foods contaminated with toxic metals, the ways toxic metals can enter the body, and the diseases caused by consumption of foods contaminated with toxic metals. Correct answers scored one, while wrong answers received no score. The total score was obtained through mean calculation. The validity of this section was measured through test-retest method, K=0.84. In [Table/Fig-1], the constructs items of HBM and ECO groups are showed.
Construct items by individual intervention groups.
| Group | Construct | Construct Items |
|---|
| HBM | Perceived susceptibility | Probability of affliction of person with diseases caused by consumption of RCWTM |
| HBM | Perceived seriousness | -The thought of being afflicted with diseases and the complications caused by consumption of RCWTM (especially some types of cancer) frightens me-Anytime I think about these diseases and complications, I have a bad feeling-If someone becomes afflicted with these diseases and complications especially cancers, they will have to deal with the problems brought about by the disease for a long time-If someone becomes afflicted with these diseases and complications especially cancers, their life will transform completely-A patient suffering from these cancers cannot survive long |
| HBM | Perceived benefits | - When I don’t use these RCWTM, I have a feeling of satisfaction-By not consuming RCWTM, I am no longer worried about suffering from the complications caused by their consumptions-By not consuming RCWTM, the probability of mortality and complications caused by their consumption diminishes-By not consuming RCWTM, the probability of needing "chemotherapy" or "surgeries or other treatments" due to incidence of cancers and other diseases caused by complications of their consumption declines-The best way to prevent these complications is not to use RCWTM |
| HBM | Perceived barriers | -The price of LR is more expensive-I have no knowledge about the complications caused by consumption of FR-LR are not usually good and well cooked-FR become less affected by pests-I cannot distinguish between RCWTM and RFFTM that I’m able to choose the healthy one-All of their family members prefer to consume FR (as it is more well-cooked) |
| HBM | Self-efficacy | -I am able not to use FR-In spite of the will of family members for consumption of FR, I don’t use this kind of rice-I can purchase LR by saving other costs-I can effectively prevent striking of pest to my consumed rice |
| ECO | Social support | -They talk to me about the advantages of consumption of LR-They talk to me about the harms (dangers) of consumption of FR-To purchase or prepare LR, they accompany me to the market-They encourage me to consume LR-For cooking LR they appreciate me-They encourage me to decrease consumption of FR through mixing it with cereals and beans-They suggest need to substitute foods without rice in the food basket of household-They encourage me to cook Pilaw rather than Kateh |
HBM: Health Belief Model, ECO: Ecological- social model, RCWTM: Rice contaminated with toxic metals, RFFTM: Rice free from toxic metals, LR: Local rice, FR: Foreign rice.
The Cronbach alpha obtained for perceived susceptibility, perceived seriousness, perceived benefits, perceived barriers, and self-efficacy were 0.72, 0.75, 0.8, 0.81 and 0.79, respectively.
All constructs of HBM were measured through a five-point Likert scale (completely correct=5 to completely wrong=1). The score of these constructs were evaluated through mean calculation.
The “PORC” was evaluated across two fields of frequency of the women consuming rice during the week and the manner of cooking rice. The women consuming rice were classified into three types including "consumption of LR, FR, and MR across three options (not consuming during the previous week, consuming 1-3 times per week, and consuming 4-7 times per week). Manner of cooking was evaluated based on two types of cooking Kateh and Pilaw. The validity of this section was obtained to be K=0.85 through test-retest method.
“Social support” in ECO included 12 questions related to the social network support of people for individual mother, father, sister, brother, spouse, children, friends, colleagues, neighbours, and relatives [Table/Fig-1]. The responses were evaluated at three points (often=2 to never=0). The score of this construct was applied as the social support score through calculating the mean. The Cronbach alpha coefficient obtained in the social support section was 0.88.
Designing Environmental Intervention
Different components of the intervention, the intervention time, targeted theoretical constructs, and objectives of the training sessions in the intervention program of consumed RFFTM have been presented in [Table/Fig-2] for each intervention group separately. In summary, every participant in the training sessions received the required instruction in sessions of 45-60 minutes within six months. The educational materials of the sessions included lecture, slide, role-playing, reminder cards, pamphlets, and educational CDs. In HBM group, the individuals were only given consultation by researchers. In ECO group, the people were involved in a multifaceted approach consisting of researchers along with social network including family members, friends, and colleagues. For the control group, there were no training sessions or telephone consultation. However, control group received the educational pamphlets and CDs following the completion of the educational intervention.
Different components of intervention, intervention time, intervention methods, targeted theoretical constructs applied in the program of intervention of consumption of healthy rice by individual intervention groups.
| Time and groups | Targeted theoretical constructs | Methods used |
|---|
| Week 1-3: HBM,ECO | Knowledge | The objectives of the training sessions:– Stating some facts about toxic metals– Introducing toxic metals that contaminate the rice consumed by households– Introducing the ways toxic metals can enter the body– Introducing the diseases caused by consumption of rice contaminated with toxic metals– Presenting solutions for reducing toxic metals in the bodythe participants received reminder card and pamphlet |
| Week 4-6:HBM | Perceived sensitivity | The objectives of the training sessions:– Enhancing the perceived sensitivity of the person about the diseases caused by consumption of rice contaminated with toxic metals |
| Perceived seriousness | The objectives of the training sessions:– Enhancing the perceived seriousness of the person regarding being afflicted with diseases caused by consumption of rice contaminated with toxic metalsthe participants received reminder card and pamphlet |
| Week 7-10:HBM | Perceived benefits | The objectives of the training sessions:– Increasing the advantages resulting from consumption of rice free from toxic metals– Enhancing the benefits of decreasing rice consumption in the household’s food basket |
| Perceived barriers | The objectives of the training sessions:– Training problem-solving and problem-solving strategies for overcoming individual and environmental barriers for consuming rice free from toxic metals– Transference of information about how to overcome the barriers means consumption of rice free from toxic metals (pest striking of rice free from toxic metals, the procedure of cooking rice free from toxic metals, and the high price of rice free from toxic metals)the participants received reminder card and pamphlet |
| Week 11-13:ECO | Social support | The objectives of the training sessions:– Formation of a social network consisting of employees by individual organization to receive group support and discussion and opinion exchange about consumption of local rice, solutions for decreasing rice consumption, and the manner of healthy cooking of rice– Group cooking of local rice in the worksitethe participants received reminder card and pamphlet |
| Week 14-16:HBM | Self-efficacy | The objectives of the training sessions:– Increasing the ability of women regarding the manner of cooking rice free from toxic metals– Increasing the ability of in preserving rice free from toxic metals so that they do not become afflicted with pests– Increasing the ability of women in selecting rice free from toxic metals in the food plan despite the desire of family members– Increasing the ability of women in economic saving in the household costs to purchase rice free from toxic metalsthe participants received reminder card and pamphlet |
| Week 17-19:ECO | Social support | The objectives of the training sessions:– Formation of social network consisting of mother, sister, friends, and relatives in virtual environments including Viber, WhatsApp, and Telegram and presentation of educational program for the people in the groups and question and answer in the virtual space to develop women social support in cooking rice free from toxic metals |
| Week 20-21:ECO | Social support | The objectives of the training sessions:– Question and answer in organizations regarding the type of consumed rice and the manner of cooking rice– Encouraging employees to continue discussion on the type of consumed rice in the worksite and the relevant social networkthe participants received reminder card and pamphlet |
| Week 22-24: HBM, ECO | Self-efficacy only for the HBM groupand social support only for the ECO group | The objectives of the training sessions:– Individual telephone consultation with women in HBM and ECO (emphasizing support of family members) groups in consuming local rice, decreasing consumption of foreign rice, and substituting it with foreign rice in the food plan and the manner of cooking rice contaminated with toxic metals as pilaw |
Considering the fact that there is no industrial factories around the rice farms in the city of Ilam and according to the conducted experiments implying the health of LR in Ilam and, more importantly, due to the contamination of the majority of rice produced in the North of country with toxic metals [2-4], Ilam LR was introduced as the RFFTM to the participants.
The training sessions of HBM group were different from those of ECO group. This was performed for role modelling of colleagues in the worksite for social support and encouraging other colleagues to consume LR. For example, first, small groups and organizations were formed to develop group support and enhance receiving social support to consume RFFTM. Next, to develop the support of family members and social network of the participants, educational groups consisted of the mother, sister, friends, colleagues, and relatives were formed in virtual spaces such as Viber, What’s App, and Telegram to realize the predetermined objectives of consuming LR. In both HBM and ECO intervention groups, the solutions for reducing consumption of FR or substituting them with LR were as follows: decreasing consumption of rice whether healthy or unhealthy in the diet, mixing LR and FR with greater portion of LR than the FR, cooking rice with a mixture of cereals and beans with a greater portion of cereals and beans, cooking foods which can be served with bread. In both of the intervention groups, rice cooking method as pilaw was emphasized as the healthy cooking method [25]. To encourage people to consume LR and continuously participate in the training sessions, a 3 kg LR package was given as a gift to every participant.
Statistical Analysis
After entering data in SPSS software (version 20.0), analyses were performed. Kolmogorov-Smirnov test was used to evaluate the normality of knowledge data and the constructs of HBM and ECO model. For descriptive analysis of the variables, the descriptive statistics of frequency and mean with a confidence interval of 95% were used. To evaluate the changes in the knowledge, groups’ constructs, and PORC in the three groups before and after intervention, due to non-normality of data, the nonparametric test of Wilcoxon was used. Repeated measures’ analysis of variance was employed for comparing the consumption of LR and FR in the three groups of HBM, ECO and control before and after intervention.
Results
The mean score of participants’ age in the HBM, ECO, and control group was 36.79±8, 33.76±5.24, and 36.4±9, respectively. In terms of academic studies, in the HBM, ECO, and control group, high school diploma (50%), academic studies (95%), and high school diploma (45%) had the highest frequency, respectively. In terms of marital status, there was no significant difference between the three groups [Table/Fig-3].
The demographic characteristics of the three groups HBM, ECO and control.
| Demographic characteristics | HBM | ECO | Control |
|---|
| Mean age | 36.79(8) | 33.76(5.24) | 36.4(9) |
| Education levelUnder diplomaDiplomaHigher than diploma | 40(50)24(30)16(20) | 04(5)76(95) | 36(45)20(25)24(30) |
| Married statusMarriedOther (single, widowed, divorced) | 11(13.8)69(86.2) | 16(20)64(80) | 7(8.8)73(91.3) |
[Table/Fig-4] indicates that the mean score of knowledge, perceived sensitivity, perceived seriousness, perceived benefits, and self-efficacy in the HBM group had a significant increase after the intervention, and regarding perceived barriers there had been a significant decrease.
Knowledge and constructs of the HBM, ECO, and control groups before and after the intervention.
| Constructs | M(SD) | Z | p-value | CONTROLM(SD) | Z | p-value | Scores range |
|---|
| Before intervention | After intervention | Before intervention | After intervention |
|---|
| HBMKnowledgePerceived susceptibilityPerceived seriousnessPerceived benefitsPerceived barriersSelf-efficacy | 1.18(2.45)7.72(1.57)19.93(3.46)20.65(3.43)25.18(3.84)11.19(3.55) | 6.95(0.21)9.07(0.96)22.71(2.17)22.96(2.1)21.25(2.5)14.75(3.74) | -8.22-5.27-5.06-4.54-6.18-5.46 | <0.001<0.001<0.001<0.001<0.001<0.001 | 0.35(1.45)8.21(1.21)20.94(2.91)20.86(2.85)25.03(3.96)11.84(3.8) | 0.98(2.21)8.08(1.64)20.86(3.25)21.06(3.19)26.21(2.77)10.74(3.92) | -1.97-0.63-0.182-0.24-1.61-1.69 | 0.03740.5040.6810.8680.1180.081 | 0-70-100-250-250-300-20 |
| ECOKnowledgeSocial support | 4.73(2.68)64(25.04) | 6.86(0.44)117(28.12) | -5.86-7.77 | <0.001<0.001 | 0.35(1.45)78.01(15.76) | 0.98(2.21)63.99(9.6) | -1.97-5.47 | 0.03740.000 | 0-70-297 |
[Table/Fig-4] shows the development of knowledge and social support after the intervention compared with the pre-intervention period in the ECO group. In the control group, a significant decrease in the social support during the second evaluation as compared with the first evaluation was evident.
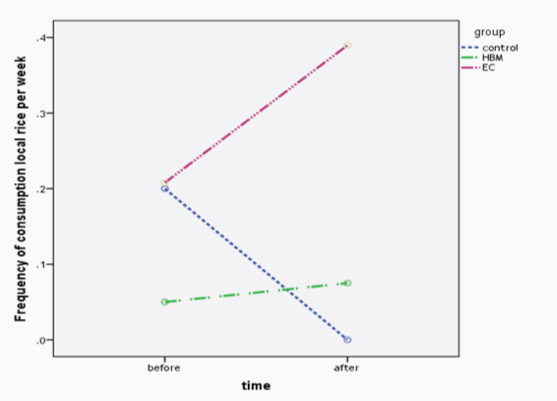
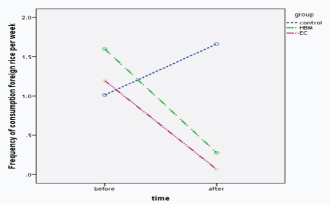
[Table/Fig-5] shows the frequency of the women consuming LR, FR, and MR for intervention and control groups separately. Growth in the consumption of LR and reduction in the consumption of FR was significant in both groups according to Wilcoxon test (p<0.001). Difference in the manner of cooking was significant for both groups. Furthermore, repeated measures’ analysis of variance indicated that the three groups under study had a significant difference in terms of consumption of LR and FR (p<0.05). Following the intervention, consumption of LR in the ECO group was greater than HBM group. Consumption of FR had decreased further in the ECO group than HBM group [Table/Fig-6,7].
Performance of consumption of local rice, foreign rice, and mixed rice as well as the cooking method in the three groups HBM, ECO and control before and after the intervention.
| Performance | HBM | Z | p-value | ECO | Z | p-value | CON | Z | p-value |
|---|
| Before interventionN(%) | After interventionN(%) | Before interventionN(%) | After interventionN(%) | Before interventionN(%) | After interventionN(%) |
|---|
| Frequency consumption of LRDid not consumeConsumes 1-3 times per weekConsumes 4-7 times per week | 78(97.5)0(0)2(2.5) | 75(93.8)4(5)1(1.2) | -7.98 | <0.001 | 70(87.5)4(5)6(7.5) | 54(67.5)21(26.25)5(6.2) | -2.74 | 0.006 | 71(88.8)2(2.5)7(8.7) | 80(100)*0(0)0(0) | -2.81 | 0.005 |
| Frequency consumption of FRDid not consumeConsumes 1-3 times per weekConsumes 4-7 times per week | 3(3.8)26(32.5)51(63.7) | 63(78.8)12(15)5(6.2) | -7.37 | <0.001 | 24(30)14(17.5)42(52.5) | 75(93.8)3(3.8)2(2.5) | -6.65 | <0.001 | 28(35)23(28.8)29(36.3) | 8(10)11(13.8)61(76.3) | -4.8 | <0.001 |
| Frequency consumption of MRDid not consumeConsumes 1-3 times per weekConsumes 4-7 times per week | 79(98.8)0(0)1(1.2) | 22(27.5)43(53.8)15(18.7) | -6.8 | <0.001 | 66(82.5)3(3.8)11(13.7) | 32(40)41(51.3)7(8.8) | -2.73 | 0.006 | 61(76.3)6(7.5)13(16.3) | 72(90)1(1.2)7(8.7) | -1.93 | 0.053 |
| Cooking methodKatehPilaw | 70(87.5)10(12.5) | 18(22.5)62(77.5) | -6.7 | <0.001 | 19(23.8)61(76.2) | 8(10)72(90) | -3.31 | 0.001 | 7(8.8)73(91.3) | 14(17.5)66(82.5) | -1.94 | 0.052 |
*Since at the time of data collection exactly after the intervention the amount of local rice in the market had reduced and its price increased consequently, we observed a lack of consumption in the control group. However, we saw an increase of consumption in both groups HBM and ECO that is an indicator of positive impact of educational intervention.
Changes in consumption of local rice in terms of frequency of consumption per week in the three groups HBM, ECO and control before and after the intervention.
Changes in consumption of foreign rice in terms of frequency of consumption per week in the three groups HBM, ECO and control before and after the intervention.
Discussion
This study was the first randomized controlled trial interventionist program comparing the effect of two interventionist models of HBM and ECO on the consumption of RFFTM and prevention of diseases caused by consumption of RCWTM among Iranian women. In this study, HBM intervention indicated positively significant changes in the constructs of the model, as compared with the women in the control group. However, it should be noted that these positive changes also existed in the social support construct in the ECO group as compared with the control group. These positive changes in the intervention groups were due to the implementation of instructional program.
This study was similar to other experimental studies in Iran and other countries aimed at enhancing knowledge on nutrition [25-27], perceived sensitivity, perceived seriousness about diseases caused by consumption of RCWTM [25,28], perceived benefits [25,29,30], self-efficacy [25,27], decreasing perceived barriers [25], and enhancing social support [31-33] in intervention groups. The findings of the research indicated improved knowledge in the intervention group, when compared with the control group. Better improvement in the HBM group in comparison with ECO group was due to the higher knowledge of ECO group before beginning the training intervention. The greater knowledge of organizational women before implementation of the training program might have been due to the high level of academic studies and access to information references about toxic metals and their impact on human body in this group compared to HBM group. Although the control group received absolutely no training program, they also had a slight increase in knowledge. This might have been due to reservation about the information caused after the completion of the questionnaire and the tendency of people to gain information about toxic metals. However, there was a significant difference regarding the knowledge of people in the intervention group when compared with the control group. The similar results of previous studies also suggested that there has been an increase in the nutrition knowledge of participants in control group [34].
Further, supporting the hypothesis of the study, following the educational program, women in ECO group consumed 26.25% LR more than those in HBM group. ECO group had a healthier food plan than the HBM group. This educational program resulted in greater reduction in the consumption of FR and led to an increase in the consumption of LR in the ECO group than in the HBM group. Furthermore, these results were in line with previous findings about the effect of HBM [27,30,34,35] and ECO [23,36] models in improving healthy diet in intervention groups.
In addition, a larger number of women in ECO group after the intervention consumed rice as pilaw in comparison with HBM women. In a study by Alidosti et al., changes in the methods of cooking foods were observed in the HBM intervention group [24]. In the control group, there was found no significant difference in HBM’s constructs after intervention program in intervention groups compared with the preliminary evaluation. The results of the educational intervention program indicated improved social support in the ECO group as compared with the control group after the intervention. These results were in line with other studies conducted in workplace and emphasize the positive role of social support in encouraging people to follow healthy diet [31-33].
The factor that might have led to greater success of the educational program in improving the nutritional performance of the ECO group rather than the HBM group was the development of social support on the part of mothers, fathers, sisters, brothers, spouses, children, relatives, neighbours; in other words, the development of social network was an influential factor.
Limitation
Evaluation of rice consumption during the week was performed by the three items of frequency of consumption of LR, FR, and MR. A larger number of questions ars required for more precise evaluation of consumption of rice in diet such as the amount of consumed rice in terms of the type of rice (LR or FR). Due to cultural context of the region, forming social networks consisted of neighbours and implementation of the educational program in the houses of participants was impossible. Therefore, in the ECO group working women were chosen. This might have affected the results, as they had higher educational degrees compared to the HBM group members. On the other hand, for the HBM group team cooking was impossible. However, it was possible for the ECO group in the worksite. Long-term evaluation of LR consumption was not performed. Therefore, the results obtained from a long-term research can provide a fundamental basis for future studies and for the objectives of interventional programs to follow a healthy diet.
Conclusion
Both instructional interventionist methods in this study caused positive and significant changes in the diet of people regarding consumption of RFFTM and decreasing consumption of RCWTM. On the other hand, development of social support might have had a more effective role in improving the diet of people.
Funding/Support: This study was financially supported by the Deputy of Research and Technology of Kurdistan University of Medical Sciences, Sanandaj, Iran.
*Since at the time of data collection exactly after the intervention the amount of local rice in the market had reduced and its price increased consequently, we observed a lack of consumption in the control group. However, we saw an increase of consumption in both groups HBM and ECO that is an indicator of positive impact of educational intervention.