Diabetes is considered as one of the most important public health problems and the fifth leading cause of death worldwide [1]. Diabetic footcare is the most common cause of hospitalisation in patients with diabetes [2]. In the United States, the cost of treating diabetic foot ulcers is 7-10 thousand dollars, and this amount will increase to 10 thousand dollars when it is complicated, and there is a need for amputation which represents heavy costs on the public health system [3]. According to the national reports, the prevalence rate of diabetic ulcers in Iran is 20% [4]. While it is thought that more than 50% of these cases are preventable, provided that the foot care procedures are trained to patient and patient does these cares on a daily basis. Proper care of feet prevents diabetic neuropathy and ulcers and infection and finally prevents amputation [5]. Studies conducted showed that training played a major role in raising awareness in diabetic patients, dealing with the disease and changing attitudes and behaviour compared to earlier [6,7]. Studies have shown that nurses have a unique position in training of diabetic patients to improve metabolic status and as a result, reduce the complications of diabetes [8,9]. Since the implementation of training programme is not enough without the involvement and active participation of patients, the obtained results will be better if this participation is more conscious [10].
Self-efficacy is a valuable tool for nurses in health-care centres, and evaluating the self-efficacy of patients by nurses and promotion of it can increase the motivation of patients for taking care of themselves; as well as, the promotion of efficacy increases the life expectancy and moderates the health behaviours [11,12]. As most studies conducted suggest that patients with diabetes have less ability to take self-care, they are inflicted with more complications such as blindness, depression, and diabetic foot ulcers [13,14]. This study was conducted for evaluation of the impact of three-month training programme on foot care and self-efficacy of patients with diabetic foot ulcers in a poor setting.
Materials and Methods
This quasi-experimental study was conducted on 60 patients with diabetic foot ulcers in Jiroft Imam Khomeini hospital from January 2016 to May 2016. The sample size was determined by Cochran’s formula with confidence interval 95%. After applying the inclusion and exclusion criteria, all the patients of the time duration were included. Initially, patients were matched in terms of age and gender. The inclusion criteria were diabetic type 2 patients with a diagnosis of diabetic foot ulcers and ready to participate in study and patients having the speech and hearing problems, having critical conditions, and history of drug abuse were excluded from the study. These patients were randomly divided into intervention and control groups (30 patients in each group).
The tools used in this study were: Demographic questionnaire, Diabetes Management Self-efficacy Scale (DMSES) and Diabetes Foot Self-care Behaviour Scale (DFSBS).
DMSES used for assessing self-efficacy among diabetic patients [15]. In research of Mohamadinejad F et al., the content and face validity of the questionnaire was confirmed by a panel of experts and its reliability was estimated 0.84 using Cronbach’s alpha [16]. This questionnaire had 20 questions, and its scoring system is based on the Likert scale and has four sections for feeding (nine questions), measuring the blood sugar (four questions), physical activity and weight control (four questions) and medical care (three questions). Each participant’s response range is between 0 and Zero represents “I do not know” and 10 represents “I am quite capable of doing,” the total score is 200 (higher the number indicates greater self-efficacy) [15].
The rate of patients’ care for foot was assessed by DFSBS which was designed by Chin YF [17]. The content and purpose of the questionnaire were to evaluate, to what extent a patient has done the foot care. The questionnaire contains seven items which were scored based on five-point Likert scale (one - never to five - always). Higher scores showed the patient’s better foot care [17]. To determine the validity, the face and content validity were used and the necessary reforms were carried out based on scientific opinions of ten faculty members of Jiroft Medical Sciences University. The reliability of the questionnaire was calculated as 0.86 through Cronbach’s alpha coefficient. Furthermore, intraclass correlation coefficient of the self-efficacy assessment tool was calculated as 0.90.
For data collection, questionnaires (DMSES and DFSBS) were distributed at one stage among the case and control groups before the start of training programme by two research assistances. Then, training programme in relation to all aspects of diabetes was begun for the case group in this way: A two-hour training session was conducted each week (for three months) by Master of Nutrition for this group. In this training session, how to care the diabetic foot and preventing the development and the formation of new ulcers were taught to patients by focusing on seven important items of DFSBS (checking the extremities and checking between the fingers, washing between the fingers, drying between the fingers after washing, the use of lotions and checking inside shoes). Also, trainings in relation to diet and intake of food groups, sport activities and weight control, the way and time of measuring blood sugar, the proper way of insulin injections and emergency procedures in the disease were presented. Transfer method of training materials was via the lecture, using slides, videos as well as viewing practical skills of trainer and individual’s experience during the participation in training process. After practical training to patients, they were also given a training pamphlet on how to perform the care. Moreover, they were asked to do the health-care daily. Then, questionnaires were distributed three months later between case and control groups for the second stage. The confirmation about foot care was done by family members. Questionnaires were filled by the interviewer for the elderly and people who lack the ability to read and write.
The control group was not given any training during this period. This study was approved by Ethical Committee of Jiroft University of Medical Science with written consent obtained from patients before data collection.
Statistical Analysis
At the end of the study, primary and secondary ranking of self-efficacy and care of the feet and their rate of change was statistically analysed using t-test. We used Kolmogorov–Smirnov test and Mann–Whitney U-test. SPSS Version 18.0 for Windows (SPSS Inc., Chicago, IL, USA) used for data analysis. The significance level was considered 0.05.
Results
In total, there were 60 patients the number of males and females were 13 (43%), 17 (57%) in control group and 17 (57%), 13 (43%) in case group, respectively. The mean age was 50 ± 3.4 and 46 ± 8.1 in case and control groups, respectively. Most of the patients in both groups were married, employed, and with lower than high school diploma education. Demographic characteristics of participants are shown in [Table/Fig-1]. Groups were similar in terms of age, marital status, occupation, education, smoking, exercise and family history and their differences were statistically significant [Table/Fig-1].
Distribution of subjects surveyed in terms of characteristics and separation of the studied groups.
| Characteristics | Control (n=30) | Case (n=30) | p value |
|---|
| Age | 50±3.4 | 46±8.1 | 0.81* |
| Gender | | | |
| Male | 13 (43) | 17 (57) | 0.3* |
| Female | 17 (57) | 13 (43) | |
| Family history of diabetes mellitus | | | |
| Yes | 13 (43) | 11 (37) | 0.21* |
| No | 17 (57) | 19 (63) | |
| Exercise | | | |
| Yes | 8 (27) | 10 (33) | 0.51* |
| No | 22 (73) | 20 (67) | |
| Smoking | | | |
| Yes | 10 (33) | 12 (40) | 0.41* |
| No | 20 (67) | 18 (60) | |
| Education | | | |
| Lower than high school diploma | 17 (57) | 19 (63) | 0.28* |
| Higher than high school diploma | 13 (43) | 11 (37) | |
| Occupation | | | |
| Employed | 20 (67) | 18 (60) | 0.21* |
| Unemployed | 10 (33) | 12 (40) | |
| Marital status | | | |
| Unmarried | 7 (23) | 5 (17) | 0.13* |
| Married | 23 (77) | 25 (83) | |
Kolmogorov–Smirnov test (K–S test or KS test) used for assessment matching and normality of data in two groups.
The comparison of the self-efficacy in patients with diabetic foot ulcers in case and control groups before training was homogeneous and Mann–Whitney U-test showed that this difference was not statistically significant (p>0.05). However, after intervention, t-test showed that this difference was statistically significant (p=0.001).
In general, according to the results shown in [Table/Fig-2], score of patients after the training was 93.56±2.1 and 182.25±1.4, for control group and case group respectively and the score of self-efficacy in case group was better than the control group (p=0.001).
Comparison of the self-efficacy in patients with diabetic foot ulcers in case and control groups before and after three months.
| Scores | Pre-test | Post-test |
|---|
| Control (n=30) | 87.95±2.1 | 93.56±2.1 |
| Case (n=30) | 81.65±3.1 | 182.25±1.4 |
| p value | *p>0.05 | *p=0.001 |
t-test used
The comparison of the foot care in case and control groups before and after the implementation of training programme showed a significant difference (p=0.001). Diabetic foot care score has been described in [Table/Fig-3] in the same way.
Comparison of the foot care in case and control groups before and after the intervention of training.
| Scores | Pre-test | Post-test |
|---|
| Control (n=30) | 31.25±1.1 | 30.18±0.8 |
| Case (n=30) | 29.49±2.4 | 47.43±1.3 |
| p value | p=0.68* | p=0.001* |
t-test used
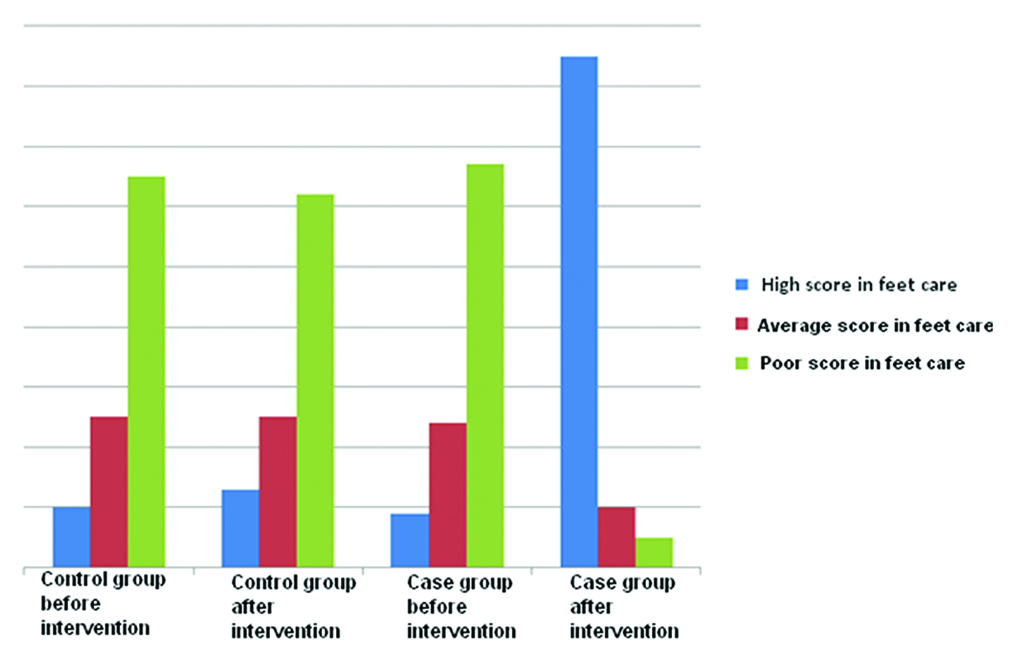
Out of 30 patients, 20 (67%) patients in the case group had poor ulcer care before training and only 5% of them had poor ulcer care after training. There was a significant difference between scores of ulcer care before and after the training (p=0.001).
In control group, 65% of patients had poor foot care score before three months but after that 62% of the patients had poor foot care score. There was difference in the scores, but it was not statistically significant.
After training, there were more patients who had high score in the foot care in case group as compared to patients in control group [Table/Fig-4].
Distribution of foot care in patients before and after the intervention.
Discussion
Most studies conducted have never shown the beneficial effects of training the methods for taking care of themselves in controlling blood sugar and complications of the disease [18,19]. According to studies done, lifestyle modification along with comprehensive training and ongoing programmes as well as strengthening the capacity of patients about their care promote the self-care situation in these patients and will have a significant role in reducing short- and long-term complications and appropriate control of the disease [20,21].
Results of the present study showed a significant difference between average self-efficacy scores in case (182.25) and control (93.56) groups three months after intervention.
Mohamadinejad F et al., also achieved to similar results. Their results showed that the average self-efficacy in diabetic patients after the training had a significant difference than before the training [16]. In a study conducted by Mahmoodi A et al., with the aim to implement the empowerment programme in diabetic patients, it was shown that patients were able to reduce their blood haemoglobin A1c level after three months of participation in these programmes because of increasing their self-efficacy and self-care ability. Mahmoodi A et al., in his study came to the conclusion that patients who participate in the care of themselves are more successful in lower limbs ulcer care [22].
Another study showed that diabetic patients who have participated in empowerment training programmes were more successful in controlling blood sugar and haemoglobin A1c due to increased awareness of the importance of haemoglobin and also increased self-efficacy and self-care, but the control group was not able to reduce haemoglobin levels A1c and this amount has been in a constant status before and after the intervention [23].
In the study conducted by Inoue M et al., on type 2 diabetic patients in 17 primary care clinics in Japan, they showed that there is a positive relationship between critical knowledge level with understanding the care in diabetes and self-efficacy [24]. In a study done by Dunn SM et al., in Australia showed that the implementation of formal training programme on diabetes for two days improved performance and efficiency of patients [25].
In our study, the average score for feet care was 47.43 in the case group and 30.18 in the control group after the intervention which is shown in the results that there was a significant difference between the case and control groups in terms of foot care at three months after the training. Most of the participants in the case group clearly showed a significant improvement in the feet care and reducing new ulcers. Our results showed that the increase of disease complications was associated with fewer scores of foot care. Chin YF et al., in their study showed that diabetic feet care training increases self-efficacy of patients and significantly improves the disease complications [26].
As mentioned, the results of previous studies are quite consistent with our results that represent the prominent role of training in increasing the self-efficacy and foot ulcers care and prevention of new ulcers in patients. By controlling their blood glucose, the patients can also have control on their disease [27].
Limitation
The limitation of this study was hard access to patients after intervention for completion of the questionnaire and small sample size. The studies with larger sample size can be conducted in future for more conclusive results.
Conclusion
The result of this study showed the implementation of training programme significantly improves the self-efficacy and feet care in diabetic patients that indicates the importance of training in patient’s empowerment and their self-care.
*Kolmogorov–Smirnov test (K–S test or KS test) used for assessment matching and normality of data in two groups.
*t-test used
*t-test used