At this juncture, evaluation of biologic agents for reconstruction of the lost periodontium becomes pertinent. Choukroun’s PRF, a second generation platelet concentrate, is a purely autologous product consisting of a flexible fibrin network that enmeshes growth factors, proinflammatory and antiinflammatory cytokines and glycoproteins [10]. Fibrin matrix supports angiogenesis, epithelial coverage of injured tissue and serves as a net to circulating mesenchymal stem cells where initial differentiation can occur to different cell lineages. Slow release of incorporated cytokines combined with properties of the fibrin matrix makes PRF a potential agent for enhancing soft and hard tissue healing and possibly regeneration.
Since, use of bone grafts alone has shown only modest clinical benefits in the management of furcation defects [5], this study was conducted to test the research hypothesis that combining PRF with bone graft would enhance the efficacy of the graft material with respect to clinical and radiographic parameters.
Materials and Methods
In this interventional study of parallel design conducted from May 2011 to June 2012, 16 systemically healthy patients (12 males and 4 females), aged 25-65 years (mean age: 43.05 ± 10.73 years) with 20 Class II furcation defects (13 buccal and 7 lingual) in mandibular first or second molars, were enrolled from the patients of Department of Periodontics, Manipal College of Dental Sciences, Mangaluru, Karnataka, India. Sample size was calculated at 95% confidence interval and 80% power based on a previous study using clinical attachment loss as the variable [6]. Of the 16 patients, 2 patients had bilateral mandibular Class II furcation defects while remaining patients had unilateral Class II furcation involvement. The research protocol was approved by the Institutional Ethical Committee (MCODS/5265/2009). All procedures were performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments. Informed consent was obtained from all subjects included in the study.
Inclusion criteria for the study were presence of furcation involvement in mandibular first or second molar with minimum of 3 mm horizontal probing depth after phase I therapy, presence of gingival margin coronal to or at the level of the roof of furcation and presence of radiographically detectable furcation involvement. Exclusion criteria included medically compromised individuals, individuals allergic to medications, pregnant and lactating mothers, tobacco consumption in any form, history of periodontal surgery at the same site, third molars with furcation involvement, untreated non vital teeth and individuals with poor oral hygiene (plaque index >1.9).
Clinical Data Collection
All patients following an initial examination and diagnosis were subjected to phase I therapy including oral hygiene instructions, supragingival scaling, subgingival scaling and root debridement. Occlusal adjustment was done whenever necessary. Four weeks after phase I therapy, a periodontal evaluation was performed to confirm the suitability of the sites for the study. The selected sites were randomly assigned to test (Group I) and control groups (Group II). Of the two patients with bilateral mandibular Class II furcation defects, both defects of one patient were assigned to test group while each of the bilateral defects of the second patient was allocated to test and control groups respectively.
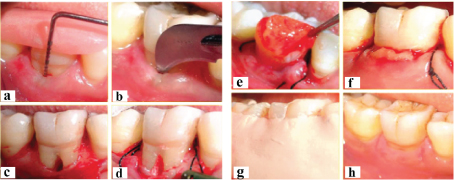
Customized acrylic stents were fabricated and trimmed to the height of contour of the teeth, to serve as fixed reference points to take measurements [Table/Fig-1a]. Vertical groove in the stent ensured reproducibility of alignment of periodontal probe. All soft tissue and hard tissue parameters were measured at base-line and six months postoperatively, using UNC-15 probe (UNC-15, Hu-Friedy, Chicago, IL, USA) for vertical measurements and 1 mm incrementally graduated Naber’s probe for horizontal measurements. Hard tissue measurements were made through bone sounding. Measurements were recorded to the nearest millimeter.
a) Preoperative probing depth measurement using acrylic stent; b) Placement of sulcular incision; c) After debridement; d) After placement of bone graft mixed with PRF; e) Placement of PRF membrane; f) After suturing; g) After placement of periodontal pack; h) After suture removal.
Soft Tissue Parameters Recorded
Distance from the Reference Point (RP) at the edge of the stent to the Cementoenamel Junction (CEJ) at the furcation defect;
Distance from RP to the Gingival Margin (GM) at the furcation defect;
Distance from RP to the Base of the Pocket (BOP) at the furcation defect;
Horizontal Probing depth (P-H).
Vertical Probing Pocket Depth (PPD), Clinical Attachment Loss (CAL) and Gingival Recession (REC) were calculated from the above measurements as C-B, C-A and B-A respectively. P-H was measured using Naber’s probe at the level of the entrance of the furcation defect. The distance through which the probe tip travels from the entrance of the furcation to the depth of the defect translates into the distance it travels at the RP which was recorded as the P-H. At the end of six months, gain in clinical attachment level and probing depth reduction (PPD and P-H) were calculated.
Hard Tissue Parameters Measured by Bone Sounding
Distance from RP to the Fornix of the Furcation (FF);
Distance from RP to the Base of the Furcation defect (BF);
Horizontal depth of furcation defect (BP-H);
Vertical Depth of Furcation Defect (VDF) was calculated from above as b-a. BP-H defect was measured similar to P-H but by bone sounding at the level of the crest of the alveolar bone at the furcation defect. The following changes were recorded six months postsurgery using the aforementioned measurements: vertical defect fill, horizontal defect fill and percentage defect fill.
Patient’s oral hygiene status was evaluated using plaque index by Silness and Loe and gingival status using gingival index by Loe and Silness at baseline and six months post surgery [7].
Radiographic Evaluation
A standardized intraoral periapical radiograph was taken for each selected site using long cone paralleling technique. Standardization was carried out using customized bite registrations using RamitecTM (3M ESPE, Minnesota, USA) bite registration material mounted on film holder while taking the radiograph. All radiographs were scanned using a scanner (HP Scanjet, Hewlett Packard, Palo Alto, CA, USA). Radiographic alveolar bone density at the furcation defect was measured in terms of mean gray value using IMAGE J software (National Institute Of Health, USA) [8-10].
Surgical Protocol
Sites assigned to control group were treated with Open Flap Debridement (OFD) and BCCG, while test group sites were treated with OFD, BCCG and PRF. Intraoral antisepsis was performed with 0.2% chlorhexidine gluconate rinse and povidone iodine solution was used to carry out extraoral antisepsis. Area subjected to surgery was anesthetized, sulcular incision placed and full thickness flap was elevated preserving as much of interproximal soft tissue as possible [Table/Fig-1b]. Thorough debridement of the osseous defect and root surface was carried out but root biomodification or osseous recontouring was not performed [Table/Fig-1c].
In the control group, bone graft material (Grabio GlasceraTM, Dorthom Medidents Pvt. Ltd, India) mixed with saline was incrementally placed in the furcation defect to the plane connecting the eminences of the adjacent root surfaces. Graft material was BCCG composed of 50% bioactive glass and 50% hydroxyapatite. Mucoperiosteal flap was repositioned, secured with simple interrupted or sling sutures and covered with periodontal dressing (Coe-PakTM GC America Inc. Illinois, USA).
PRF was prepared, following the protocol developed by Choukroun J et al., [4], ten minutes prior to its placement. Intravenous blood collected from each patient in 10 mL glass-coated plastic tubes (Becton Dickinson Vacutainer, Franklin Lakes, NJ, USA) by venipuncture of antecubital vein and immediately centrifuged at 3,000 revolutions (400 g) per minute for 10 minutes. Centrifugation immediately after collection allows the formation of a structured fibrin clot in the middle of the tube, with the RBCs at the bottom and Platelet Poor Plasma (PPP) at the top. PPP was syringed out using a sterile syringe and PRF was separated from RBC base (preserving a small red blood cell layer) using sterile scissors. It was then transferred onto a sterile gauze compress and gently squeezed in the gauze compress to obtain a stable PRF membrane.
In the test group, the furcation defect was incrementally filled and condensed with bone graft material mixed with PRF clot, using a plastic instrument [Table/Fig-1d]. PRF membrane was then placed over the furcation, with the RBC interface coronally [Table/Fig-1e]. The membrane was positioned slightly over the edge of the gingival collar. The mucoperiosteal flap was repositioned and secured with simple interrupted or sling sutures using 4-0 non-absorbable black silk surgical suture material (Ethicon, Johnson & Johnson, Somerville, NJ, USA) [Table/Fig-1f]. The surgical area was protected and covered with periodontal dressing [Table/Fig-1g].
Postoperative care
Antibiotic (Amoxicillin 500 mg, TID for five days) and analgesic (Ibuprofen 400 mg + Paracetamol 325 mg, TID for three days) were prescribed. Patients were instructed to rinse with chlorhexidine gluconate (0.2%) twice daily for four weeks and to refrain from brushing over the periodontal dressing. Periodontal pack and sutures were removed 10 days postoperatively [Table/Fig-1h]. Surgical wounds were gently cleansed with povidone iodine solution and patients were instructed to brush gently using Charter’s technique with a soft toothbrush. Patients were advised not to use any interdental cleansing aids in the treated area for four weeks after surgery. Recall appointments were made at 15 days, 30 days, 3 and 6 months for follow up and plaque control.
Statistical Analysis
The statistical analysis was done using SPSS 13.0 (SPSS Inc, Chicago, USA). Intragroup comparison of parameters within the respective groups was done using Wilcoxon signed rank test and intergroup comparison between Group I and Group II using Mann-Whitney U test. Level of significance of 0.05 was considered for all statistical comparisons.
Results
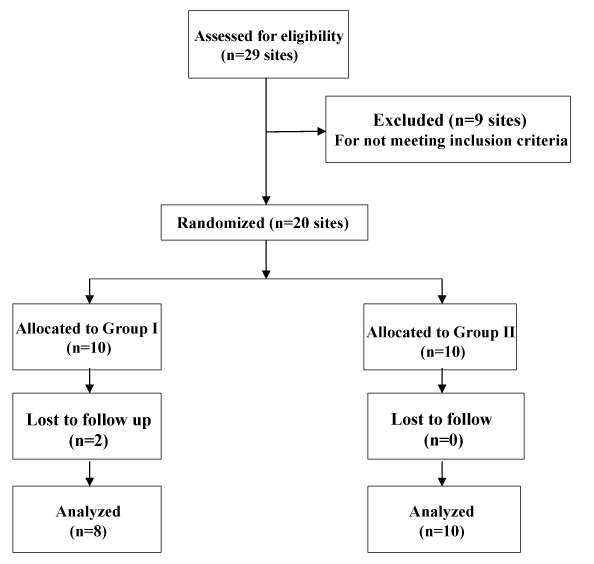
A total of 20 Class II furcation defects in 16 systemically healthy patients were included at the initiation of the study. Two patients from Group I dropped out before the termination of the study and a total of 14 patients with a mean age of 42.28±10.72 years having 18 defects completed the six months follow up [Table/Fig-2]. No significant difference in age, gender, location of defects (buccal/lingual) or type of tooth (first/second molar) existed between the two groups. Plaque index and gingival index showed statistically significant decrease over six months in both the groups but there was no significant difference between the groups at baseline or at six months [Table/Fig-3]. Statistically significant reduction in PPD, CAL, P-H, VDF and BP-H was observed in test group when compared to control group at six months [Table/Fig-4]. Percentage vertical defect fill was 40.68% and 20% in test and control groups respectively. Percentage horizontal defect fill was 47.06% and 24.44% in test and control groups respectively. Besides, an intergroup comparison revealed significant increase in radiographic bone density at the furcation defect in test group compared to control group at 6 months [Table/Fig-5].
Flow chart showing the inclusion and exclusion of sites.
Plaque index and gingival index at baseline and six months in test and control groups.
| Parameters | Time interval | Baseline | At six months postoperative | Difference | p-value |
|---|
| Plaque Index [PI] | Group I | 0.59 ± 0.090 | 0.50 ± 0.064 | 0.090 ± 0.036 | 0.012* |
| Group II | 0.61 ± 0.105 | 0.51 ± 0.072 | 0.096 ± 0.064 | 0.017* |
| p-value | 0.674^ | | 0.753^ | |
| Gingival Index [GI] | Group I | 0.99 ± 0.088 | 0.84 ± 0.172 | 0.147 ± 0.101 | 0.012* |
| Group II | 1.03 ± 0.122 | 0.83 ± 0.100 | 0.203 ± 0.114 | 0.012* |
| p-value | 0.674^ | | 0.294^ | |
Wilcoxon signed rank test and Mann-Whitney U test
Significant [p < 0.051];
Non-significant [p > 0.051]
Mean changes in clinical parameters between two groups over six months.
| Group I | Group II | Comparison between Group I and Group II |
|---|
| Parameter | Baseline mean±SD [mm] | Six months postoperative mean± SD [mm] | Mean difference over six months mean±SD [mm] | Baseline mean±SD [mm] | Six months postoperative mean±SD [mm] | Mean difference over six months mean±SD [mm] | Mean±SE [mm] | p-value |
|---|
| Probing Pocket Depth [PPD] | 5.63±1.41 | 2.25±0.46 | 3.375±1.061 (p=0.007†) | 4.90±0.57 | 2.50 ± 0.53 | 2.40±0.516 (p=0.004†) | 0.975±0.380 | 0.007† |
| Clinical Attachment Loss [CAL] | 7.00±0.93 | 4.00±0.54 | 3.00±0.926 (p=0.010*) | 5.90±0.88 | 4.00 ± 0.82 | 1.90±0.568 (p=0.004†) | 1.100±0.354 | 0.006† |
| Gingival Recession [REC] | 1.38±0.74 | 1.75±0.71 | -0.375±0.518 (p=0.083^) | 1.10±0.99 | 1.50 ± 0.97 | -0.40±0.516 (p=0.046*) | 0.025±0.245 | 0.916^ |
| Horizontal Probing Depth [P-H] | 3.75±0.71 | 1.25±0.46 | 2.50±0.535 (p=0.010*) | 3.80±0.63 | 2.40 ± 1.08 | 1.40±0.843 (p=0.006†) | 1.100±0.344 | 0.009† |
| Vertical Depth of the Furcation Defect [VDF] | 3.38±1.408 | 2.00±0.926 | 1.375±0.518 (p=0.023*) | 3.00±1.25 | 2.40 ± 1.08 | 0.60±0.699 (p=0.034*) | 0.775±0.297 | 0.023* |
| Horizontal depth of the Furcation Defect [BP-H] | 4.25±0.463 | 2.25±0.707 | 2.00±0.756 (p=0.030*) | 4.50±0.71 | 3.40 ± 0.97 | 1.10±0.876 (p=0.008†) | 0.900±0.392 | 0.030* |
Wilcoxon signed rank test and Mann-Whitney U test
Significant [p< 0.05];
Non-significant [p>0.05];
Highly significant [p<0.01]
Radiographic bone density at baseline and six months in test and control groups [in mean gray levels].
| Parameter | Time interval | Baseline | At six months postoperative | Difference | p- value |
|---|
| Mean gray value at the defect | Group I | 89.52± 14.97 | 109.60 ± 19.86 | 20.08 ± 19.53 | 0.023* |
| Group II | 96.71 ±19.78 | 101.97 ± 20.10 | 5.26 ± 5.94 | 0.021* |
| p-value | 0.408^ | | 0.036* | |
Wilcoxon signed rank test and Mann-Whitney U test
Significant [p < 0.05];
Non-significant [p > 0.05]
Discussion
This clinical study was designed to evaluate and then compare the regenerative potential of BCCG and its combination with biologic agent PRF in mandibular Class II furcation defects in terms of six parameters: reduction in PPD, gain in CAL, vertical, horizontal and percentage bone fill and change in radiographic bone density. Such a comparison would help in inferring whether addition of PRF to bone graft has an enhanced therapeutic benefit in the management of furcation defects.
In the test group (Group I), the mean PPD reduction of 3.38±1.06 mm was statistically highly significant and mean clinical attachment gain of 3.00± 0.93 mm was statistically significant. Comparing with an arm of the study conducted by Pradeep AR et al., in which a combination of PRF and porous hydroxyapatite were used with OFD in mandibular Class II furcation defects [11], the mean reduction in PPD was 3.68±1.07 mm and mean relative vertical clinical attachment gain was 3.31±0.52 mm both being in accordance with the results of this study. In a study by Lekovic V et al., wherein the investigators combined bovine porous bone mineral and PRF and by Pradeep AR et al., wherein porous hydroxyapatite was combined with PRF in the management of intrabony defect a significant reduction in PPD and gain in clinical attachment level was observed from baseline [12,13]. This is in accordance with the results of this study though a direct comparison is debatable since defect morphology can influence the outcome of regenerative procedures.
Bone sounding has been considered to be as reliable as surgical re-entry for assessing hard tissue changes, hence was used for indirect bone measurement in this study [14,15]. The control group showed a mean reduction in VDF of 0.60±0.70 mm and BP-H of 1.10±0.88 mm, while in the test group mean reduction in VDF was 1.38±0.52 mm and in BP-H was 2.00±0.76 mm. In a study arm of the systematic review by Reynolds MA et al., comparing bone graft alone to bone graft with ePTFE barrier for the treatment of mandibular furcation defects [5], following observations were made: mean horizontal furcation defect fill ranged from 1.1 mm to 3.3 mm for combination therapy and from 1.0 mm to 1.8 mm for grafting alone. Improvements in mean vertical defect fill for combined therapy was 0.1 mm to 2.9 mm which closely paralleled those observed following grafting alone (0.4 mm to 2.8 mm). The vertical and horizontal defect depth reduction in the test and control groups observed in the present study were within the range observed in this systematic review and the test group showed significant increase when compared to the control group.
Mean percent horizontal defect fill in the test group was 47.06% while in control group was 24.44%. In the test group, mean percent vertical defect fill was 40.68% while in the control group was 20%. Clinical improvement from Class II to Class I furcation defect was observed in all test sites and 60% of the control sites. However, complete furcation closure was not observed at any of the treated sites. Machtei EE et al., [16] observed that postoperative changes were most significant in the horizontal dimension of the furcation defects, with less dramatic but nonetheless statistically significant changes in the vertical axis of the furcation. Similar findings have been reported by Yukna RA [17] and Caffesse RG et al., [18]. The findings in the present study are in agreement with this observation.
Radiographic analysis revealed that in the test group, mean increase in radiographic bone density after six months follow up was 20.08±19.53 gray levels and in the control group 5.26±5.94 gray levels. There was a significant increase in density in the test group compared to control group indicating that PRF may enhance the regenerative capacity of BCCG.
Studies have shown modest clinical benefit in combining bone grafts with barrier membrane in the treatment of furcation defects [5,19]. Complications observed with GTR include membrane exposure with subsequent bacterial contamination, erythema, swelling, suppuration and postoperative pain [20]. High cost and need for second stage surgery in case of non-resorbable membranes are other deterrents. In this regard, PRF as an autologous resorbable dense fibrin scaffold with slow release of growth factors appears to be a plausible alternative. PRF can act as an interpositional biomaterial, if not a strong barrier, and avoid early invagination of gingival epithelium due to the release of TGF-β which acts as a growth inhibitor of epithelial cells [21,22].
In the present study none of the complications associated with GTR were observed at the test sites. Besides, in this study as well as in studies by Jankovic S et al., and Simonpieri A et al., a marked diminution in postoperative pain and discomfort has been noted [23,24]. Postoperative inflammation appeared to be less in the test group when compared to the control group. This could be due to PRF acting as an immune regulatory node with inflammation retrocontrol abilities. The presence of inflammatory retrocontrol cytokines (particularly IL-4), chemotactic properties of cytokines like IL-1β, IL-6 and TNF-α as well as their capacity to facilitate access to the injured site (neovascularization) could explain the reduction of postoperative infections and reduced inflammation noted at surgical sites when PRF is used as a surgical additive [25]. Inspite of these advantages of PRF over commercially available barrier membranes, early resorption substantially shorter than four to six weeks necessary for GTR and less than ideal space maintenance still stand in the way of using PRF as a GTR membrane.
Limitation
A larger sample size and long term follow up would have been more conclusive in deriving inferences from the end results. Besides, digital subtraction radiography, CBCT or computer assisted densitometric image analysis would have thrown more light on hard tissue changes observed in this study.
Conclusion
At this point in time when bone graft, GTR or a combination of the two have not been able to achieve predictable closure of furcation defects, research on adjunctive and alternative treatment modalities to accomplish this end gains increased importance. With significant improvement at test compared to control sites, the present study favors the adjunctive use of PRF with BCCG over BCCG alone in the management of mandibular Class II furcation defects. Currently, there is sparse evidence to support the use of PRF with bone graft in the management of periodontal osseous defects in general and furcation defects in particular. Further studies are required to assess the added benefit of combining PRF with bone graft material in periodontal regeneration.
Wilcoxon signed rank test and Mann-Whitney U test
*Significant [p < 0.051];
^Non-significant [p > 0.051]
Wilcoxon signed rank test and Mann-Whitney U test
*Significant [p< 0.05];
^Non-significant [p>0.05];
†Highly significant [p<0.01]
Wilcoxon signed rank test and Mann-Whitney U test
*Significant [p < 0.05];
^Non-significant [p > 0.05]