Diabetes Mellitus (DM) is one of the most prevalent endocrine disorder characterized by production of little or no insulin and/or concomitant resistance to the metabolic action of insulin on target tissues. Hyperglycaemia is the immediate metabolic consequence of diabetes mellitus resulting in widespread multiorgan damage ranging from micro to macro vascular complications [1].
India is likely to face epidemic of DM in elderly population. The global prevalence of diabetes is 8.3% in adult population. Worldwide the number of people with diabetes is expected to escalate upto 551.9 million by 2030, corresponding to 9.9% of adult population [2]. Type 2 DM is the fifth most common condition and sixth leading cause of mortality amongst the elderly. Asian Indians are at a greater risk of developing diabetes. India is world’s second most populous country with significant number of patients with Type 2 DM than any other nation [2]. According to WHO, developing countries comprise of 70% of diabetic population, among which 50.8 million people suffering from diabetes are residing in India. In India, approximately 57.2 million and 101.2 million people are expected to be noticed by the year 2025 and 2030 respectively [2,3]. Thus, India could be considered as the diabetic capital of the world.
Diabetes, over long period, is associated with poor oral health which is characterised by periodontal, gingival and other oral problems. These problems are mostly related to poorly controlled metabolic glucose level [4]. Changed oral environment may lead to cariogenic and gingival lesions. Many other problems are associated with increased glucose level, they are, tooth loss, altered taste, periapical abcess, proneness to bacterial, viral and fungal infections, salivary gland disorder etc., [5,6].
Moreover, it has been found that with increase in blood glucose level in diabetes, there is concomitant increase in salivary glucose level [2,7-13]. As saliva is an organic fluid, it represents the hormonal, immunological, neurological, nutritional and metabolic state of an individual.
Glucose being a small molecule passes through porous blood vessels wall and then through blood plasma and gingival fluid, reaches the saliva [7]. Elevated glucose level in saliva could induce an increase in the number of saccharolytic bacteria associated with dental disease in the saliva due to high concentration of organic acids produced by the bacteria as a result of their metabolism of glucose [14]. Also, saliva of diabetic has shown significantly altered salivary pH (acidic) leading to poor oral health. Decrease in salivary pH favours increase growth of pathogenic microbial flora, a common finding in diabetics [4]. These microbes thrive on increased salivary glucose and leads to destruction of hard and soft tissues of oral cavity.
Toothbrush and toothpaste are most widely and universally accepted oral hygiene aids to maintain proper oral health [15]. Moreover, toothpaste has its effects on salivary components including salivary pH [16,17]. Thus, the present study was conducted with an aim to assess and compare the effect of sugar free toothpaste (Vicco SF) and regular toothpaste (Colgate) on salivary glucose and salivary pH among type 2 diabetes and non-diabetes patients. The research hypothesis was that there was no difference in the effect of sugar free toothpaste (Vicco SF) and regular toothpaste (Colgate) on salivary glucose and salivary pH among Type 2 diabetic and non-diabetic patients.
Materials and Methods
The present study was conducted in Department of Public Health dentistry, ACPM Dental College, Dhule and a Private Pathology laboratory, Maharashtra, India.
The present study was a randomized controlled crossover trial and was carried out in two phases. Before the start of the study, written informed consent was obtained from study subjects. The study proposal was submitted for approval and clearance to the ethical committee held at ACPM Dental College, Dhule, and the clearance was obtained.
A pilot study was conducted before the start of the study and the sample size for present study was estimated to be minimum of 20 subjects in each group using N=2T2 x S2/D2 formula, where N= Number of samples, T= Theoretical value of ‘t’ distribution which is 95% confidence i.e., 2.13, D= Minimum expected difference between diabetic and non-diabetic i.e., 1.5 mg%, S= Pooled standard deviation=2.2, N= 19.5~20 (minimum). A ratio of 1:1.5 of sample size was selected for the present study [18].
Based on the results of pilot study, Group A (study group) comprised of 30 subjects, aged between 38-66 years (mean age 53 years) with an established diagnosis of Type 2 DM. The subjects were randomly recruited from Archana Diabetologic Hospital, through lottery method which was carried out by the hospital administrative officer. The Group B (control group) comprised of 45 non-diabetes subjects, aged between 34-64 years (mean age 51 years).
Subjects Selection Criteria
Subject with (either controlled/uncontrolled) Type 2 DM and first, second or third order relatives of study subjects with Diabetes were included. All the subjects having minimum of 20 functional teeth in oral cavity were included. Subjects with any other systemic illness or a modification other than for diabetes and subjects with adverse habits (betel chewing, tobacco chewing) were excluded.
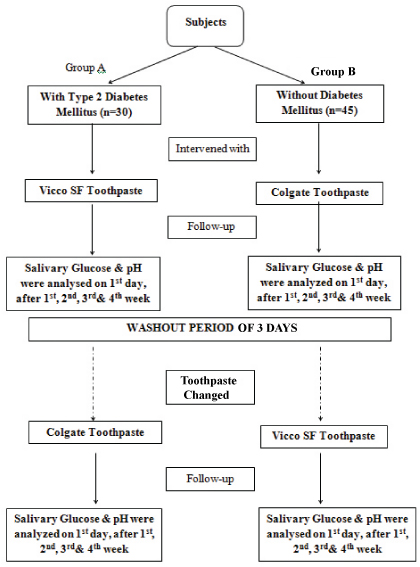
In phase 1, subjects in Group A and Group B were intervened with sugar free (Vicco SF) and regular tooth paste (Colgate) respectively for four weeks. Subjects were advised to brush twice daily. After the end of phase 1, toothpaste were switched over between the groups after washout period of 21/2 (approx 3 days) days to rule out any possible carryover effect [19,20]. During washout period, subjects were advised to brush with water alone. No changes in their brushing habits were made. In phase 2, subjects in Group A and Group B were intervened with regular toothpaste (Colgate) and sugarfree toothpaste (Vicco SF) respectively for another four weeks. In both phases, unstimulated saliva samples were obtained for each subject only once on day 1, at the end of first, second, third and fourth week in a sterile container and were assessed for salivary glucose levels and salivary pH before and after brushing. In both the phases, all the subjects and the laboratory assistant analysing the parameters were blinded. All the toothpaste were wrapped by brown color sellotape and sterile containers were numbered bb1, bb2, bb3 etc for saliva collected before brushing (bb) and ab1, ab2, ab3 etc for saliva collected after brushing (ab).
Salivary Sample Collection
Saliva collection was done in early morning hours. One hour prior to the collection of saliva, the subjects were asked to refrain from eating, drinking or other oral hygiene procedures. Subjects were asked to hold the saliva and collect/spit in the sterile container, containing sodium fluoride, till 1.5 ml of saliva was collected [2,9,21,22]. After collection, samples were stored at 4°C and were carried to laboratory as soon as possible for analysis of the study parameters [23].
Salivary pH Estimation
Salivary pH was estimated by digital pH meter, Hanna Instrument (Hanna pH Tester Checker) [24].
Salivary Glucose Estimation
The collected saliva samples were centrifuged in the semi-automatic analyser (Remi Centrifuge, Mumbai). On centrifugation of unstimulated saliva (1 ml for 3000 rpm for 20 minutes), clear supernatant was processed for estimation of salivary glucose. Glucose estimation was done by GOD-POD (ERBA, Germany) kit [4,21,25]. Initially, 1000 µl of glucose reagent solution was taken in a test tube, and then 10 µl of test salivary sample was added and stirred properly. After 15 minutes, the test sample was aspirated and the readings were noted (ERBA CHEM-5 Plus).
Statistical Analysis
The collected data was dichomotous in nature and was subjected to paired t-test for intragroup comparison (from baseline, before brushing on day 1 to after brushing at the end of fouth week) and unpaired t-test for intergroup comparison using SPSS version XVI software. Intergroup comparison was done between:
Phase 1 Group A and Phase 2 Group A;
Phase 1 Group B and Phase 2 Group B;
Phase 1 Group A and Phase 2 Group B;
Phase 1 Group B and Phase 2 Group A.
Results
Appropriate follow up of all the subjects was achieved and hence data of all the subjects was statistically analysed.
Intragroup Comparison
[Table/Fig-2] demonstrates mean values of salivary glucose levels and salivary pH of subjects in Group A (diabetes) and Group B (non-diabetes) of both phases. Result shows statistically highly significant reduction of salivary glucose (p<0.001) and increase of salivary pH (p<0.001) in diabetes and non-diabetes group using sugarfree toothpaste. Diabetes group using regular toothpaste showed comparatively less reduction of salivary glucose (p<0.001) than sugar free toothpaste. Also, reduction of salivary glucose was statistically non-significant (p=0.12) in non-diabetes group using regular toothpaste. Salivary pH was significantly increased (p<0.001) in both the groups in both phases.
Comparison of changes in salivary glucose levels and salivary pH- intragroup.
| Variables | Bb Day 1 (baseline) | ab week 4 | Diff | t | p |
|---|
| S. Glu mg/dl | S. pH | S. Glu mg/dl | S. pH | S. Glu mg/dl | S. pH | S. Glu mg/dl | S. pH | S. Glu mg/dl | S. pH |
|---|
| Ph. 1 Gr. A (Dv) | 7.74 + 1.95 | 6.74 + 0.03 | 4.57 + 0.87 | 6.90 + 0.04 | 3.17 + 1.47 | 0.16 + 0.05 | 11.76 | 19.54 | <0.001a | <0.001a |
| Ph. 2 Gr. A (Dc) | 7.47 + 1.05 | 6.67 + 0.03 | 6.37 + 1.00 | 6.74 + 0.04 | 1.10 + 0.77 | 0.07 + 0.04 | 7.81 | 8.71 | <0.001a | <0.001a |
| Ph. 1 Gr. A v/s Ph. 2 Gr. A | -- | -- | -- | -- | t = 6.80 P= <0.001 | t =8.49 P= <0.001 | | -- | -- | -- |
| Ph. 1 Gr. B (NDc) | 5.08 + 1.28 | 6.81 + 0.03 | 4.84 + 1.07 | 6.85 + 0.04 | 0.24 + 1.03 | 0.04 + 0.04 | 1.59 | 5.43 | 0.12, ns | <0.001a |
| Ph. 2 Gr. B (NDv) | 6.20 + 0.88 | 6.70 + 0.04 | 3.51 + 0.40 | 6.87 + 0.03 | 2.69 + 0.87 | 0.17 + 0.05 | 20.77 | 21.75 | <0.001a | <0.001a |
| Ph. 1 Gr. B v/s Ph. 2 Gr. B | -- | -- | -- | -- | t =12.19 p= <0.001 | t =13.03 p= <0.001 | | -- | ---- | |
p<0.001 HS
Intragroup comparisons (horizontal) : paired t-test
Intergroup comparisons (vertical) : unpaired t-test
Ph 1 Gr. A (Dv): Diabetes subject using sugarfree toothpaste (Vicco SF) in phase 1
Ph 1 Gr. B (NDc): Non-diabetes subject using regular toothpaste (Colgate) in phase 1
Ph 2 Gr. A (Dc): Diabetes subject using regular toothpaste (Colgate) in phase 2
Ph 2 Gr. B (NDv): Non-diabetes subject using sugarfree toothpaste (Vicco SF) in phase 2
Bb Day 1: Salivary glucose level before brushing on day 1
ab week 4: Salivary glucose level after brushing at the end of fourth week
Intergroup Comparison
[Table/Fig-2] shows comparison between phase 1 Group A and phase 2 Group A (DV and DC) and phase 1 Group B and phase 2 Group B (NDC and NDV). Results were found to be highly significant (p<0.001) for salivary glucose and salivary pH.
[Table/Fig-3] shows comparison between phase 1 Group A and phase 2 Group B (DV and NDV), results were statistically insignificant for both salivary glucose (p=0.12) and salivary pH (p=0.59).
Comparison of changes in salivary glucose levels and salivary pH- intergroup.
| Variables | Bb Day 1 (baseline) | ab week 4 | Diff | t | p |
|---|
| S. Glu mg/dl | S. pH | S. Glu mg/dl | S. pH | S. Glu mg/dl | S. Glu mg/dl | S. pH | S. Glu mg/dl | S. pH | S. Glu mg/dl |
|---|
| Ph. 1 Gr. A (Dv) | 7.74 + 1.95 | 6.74 + 0.03 | 4.57 + 0.87 | 6.90 + 0.04 | 3.17 + 1.47 | 0.16 + 0.05 | 11.76 | 19.54 | <0.001a | <0.001a |
| Ph. 2 Gr. B (NDv) | 6.20 + 0.88 | 6.70 + 0.04 | 3.51 + 0.40 | 6.87 + 0.03 | 2.67 + 0.87 | 0.17 + 0.05 | 20.77 | 21.75 | <0.001a | <0.001a |
| Ph. 1 Gr. A v/s Ph. 2 Gr. B | -- | -- | -- | -- | t = 1.59 P = 0.12, ns | t = 0.54 P = 0.59, ns | -- | -- | -- | -- |
| Ph. 1 Gr. B (NDc) | 5.08 + 1.28 | 6.81 + 0.03 | 4.84 + 1.07 | 6.85 + 0.04 | 0.24 + 1.03 | 0.04 + 0.04 | 1.59 | 5.43 | 0.12, ns | <0.001a |
| Ph. 2 Gr. A (Dc) | 7.47 + 1.05 | 6.67 + 0.03 | 6.37 + 1.00 | 6.74 + 0.04 | 1.10 + 0.77 | 0.07 + 0.04 | 7.81 | 8.71 | <0.001a | <0.001a |
| Ph. 1 Gr. B v/s Ph. 2 Gr. A | -- | -- | -- | -- | t = 4.11 p= <0.001 | t = 3.4 p= <0.05b | -- | -- | -- | -- |
p<0.001 HS
p<0.05 sig
Intragroup comparisons (horizontal): paired t-test Intergroup comparisons (vertical): unpaired t-test
Ph 1 Gr. A (Dv): Diabetes subject using sugarfree toothpaste (Vicco SF) in phase 1
Ph 1 Gr. B (NDc): Non-diabetes subject using regular toothpaste (Colgate) in phase 1
Ph 2 Gr. A (Dc): Diabetes subject using regular toothpaste (Colgate) in Phase 2
Ph 2 Gr. B (NDv): Non-diabetes subject using sugarfree toothpaste (Vicco SF) in phase 2
Bb Day 1: Salivary glucose level before brushing on day 1
ab week 4: Salivary glucose level after brushing at the end of fourth week
The comparison between phase 1 Group B and phase 2 Group A was found to be statistically significant for both salivary glucose (p<0.001) and salivary pH (p<0.05).
Discussion
Hyperglycaemia is the immediate metabolic consequence of DM. The consequences of DM has large burden on the individual as the metabolic derangement bound with Diabetes Mellitus causes secondary pathophysiological changes in multiple organ systems [21]. Increase in blood glucose level concomitantly increases salivary glucose in diabetes.
Studies have been conducted to compare and correlate salivary glucose level and blood glucose level. Hedge A et al., and Vasconcelos AC et al., found that salivary glucose level was higher in diabetes than in non-diabetes controls [4,7]. In addition, results showed that salivary pH is decreased in diabetes when compared with non-diabetes controls [4].
Correlation between salivary glucose level and blood glucose level is also supported by many more studies (2,7-14). Less significant correlation was also found in children with diabetes [21,26].
It is of utmost importance for individuals suffering from diabetes to maintain the glucose level to normal throughout their lifespan as it indeed has an impact on the risk of development of complications [2].
Therefore, the present study was an attempt to assess the effect of sugar free and regular toothpastes on salivary glucose and salivary pH in Type 2 diabetes and non-diabetes subjects.
In the present crossover study, in phase 1, 30 Type 2 diabetes subjects (Group A) and 45 non-diabetes (Group B) were intervened with sugar free and regular toothpaste respectively. In phase 2, tooth pastes were switched over between the groups. Salivary glucose and salivary pH was assessed on day 1, at the end of first, second third and fourth week.
Unstimulated whole saliva was taken for estimation, as in stimulated saliva there are alterations in the salivary composition; hence the diagnostic possibility has more with unstimulated saliva than stimulated saliva [2,13].
Saliva was collected in a sterile container by spitting method, to which sodium fluoride was added to prevent alteration in salivary glucose (stabilizing effect) [2,9,21,22].
Conventionally, there are two methods for estimation of salivary pH. First is strip coded method and secondly the digital pH meter. In the present study, Hanna instrument digital pH meter was used [24]. As exact numerical value was required; this is more applicable for comparison.
Salivary glucose estimation was done by glucose oxidase peroxide method, which is also supported by many other studies [4,21,25].
The result showed that salivary glucose level was decreased and salivary pH was increased in both the groups using sugar free toothpastes. However, group using sugar free tooth paste showed highly significant changes when compared with regular toothpaste. The intergroup comparison between phase 1 Group A and phase 2 Group B was found to be non-significant. This is probably because, both the group were using sugarfree (Vicco SF) tooth paste.
The decrease in salivary glucose among subjects using sugarfree toothpaste was probably due to anti-diabetic effect of the principle ingredients of sugarfree toothpaste.
Following are the principle ingredients of Vicco SF toothpaste with their mode of anti-diabetic action: Bakul (Mimusops elengi, 3.2 g), Manjishtha (Rubia Cordifola, 2.6 g) and Jambhul (EugeniaJambolana, 1 g) act by restoration of B cells of Langerhans [27-29]. Patang (Caesalpiniaceae 2.4 g), Babool (Acacia Arabica, 1.8 g and Dalchini (Cinnamomum Zeylanicum,0.16 g) act by increasing insulin secretion [30]. Trifal (1.6 g) acts by the virtue of hypoglycaemic effect due to sorbitol [31]. Also, increase in salivary pH among subjects using sugarfree toothpaste might be because of reduced salivary glucose.
Sorbitol is one of the key ingredients used as humectant and sugar substitute in most of the regular toothpaste. However, exploration of literature reveals that sorbitol had no significant effect on salivary microorganisms and oral glucose clearance [32,33]. Moreover, subjects using regular toothpaste also showed increase in pH, perhaps the act of tooth brushing itself helped in reducing the microbial load, thus indirectly showed its effect on salivary pH and simultaneously salivary glucose [34]. Also, salivary pH is buffered to a small extent by saliva proteins and phosphate. The major influence on saliva pH is of bicarbonate ion which is a by-product of cell metabolism. Bicarbonate ions present in saliva neutralizes acid produced by microorganisms when carbohydrate is fermented. An increase in bicarbonate ion concentration is due to the increased metabolic rate. This, in turn, raises the pH (more alkaline) of saliva [35,36].
Limitation
Separate controlled and uncontrolled diabetic status was not considered in this study. Due to less available literature, results were not compared with other studies. Duration of effect of sugarfree toothpaste was not assessed.
Recommendations
Effect of sugarfree toothpaste should be assessed for its acceptance, efficacy and adverse effect over a long period of time. Changes, if any, in oral health status should be evaluated before and after usage of sugarfree toothpaste over a period of time (effect of sugarfree toothpaste should be assessed on oral hard and soft tissues). Relationship between decrease in salivary glucose and increased salivary pH should be evaluated. Microbial changes should be evaluated after use of sugarfree toothpaste.
Conclusion
Our study findings suggest that sugarfree toothpaste could be recommended for subjects with diabetes mellitus for maintaining their proper salivary glucose and salivary pH level. Thus, helps to improve oral health.