Induction with Varied Histological Patterns in Adenomatoid Odontogenic Tumour
Nawal Khan1, Radhika M Bavle2, K Paremala3, Soumya Makarla4, Reshma Venugopal5
1 Postgraduate Student, Department of Oral and Maxillofacial Pathology, Krishnadevaraya College of Dental Sciences, Bangalore, Karnataka, India.
2 Professor and Head, Department of Oral and Maxillofacial Pathology, Krishnadevaraya College of Dental Sciences, Bangalore, Karnataka, India.
3 Reader, Department of Oral and Maxillofacial Pathology, Krishnadevaraya College of Dental Sciences, Bangalore, Karnataka, India.
4 Reader, Department of Oral and Maxillofacial Pathology, Krishnadevaraya College of Dental Sciences, Bangalore, Karnataka, India.
5 Senior lecturer, Department of Oral and Maxillofacial Pathology, Krishnadevaraya College of Dental Sciences, Bangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Nawal Khan, Postgraduate Student, Department of Oral and Maxillofacial Pathology, Sir MVIT Campus, Off International Airport Road, Hunusamaranahalli, Via Yelahanka, Krishnadevaraya College of Dental Sciences, Bangalore-562157, Karnataka, India.
E-mail: parisaig@yahoo.com
Dentin induction, Follicular variant, Impacted premolar, Mandibular
A 38-year-old Indian female patient reported to the clinic with the complaint of missing tooth in the left lower back tooth region. She also gave history of mild swelling in the same area associated with tingling sensation of left lower lip. Extraorally, there was no evidence of any swelling in that area. However, on intraoral examination, a non tender bony hard swelling on the left lingual side of the mandible was seen extending from teeth #33 to 36 region and was approximately 3.0 cm in diameter. Buccal vestibular obliteration and missing mandibular first premolar tooth #34 was also noticed in the same region [Table/Fig-1]. An orthopantomogram revealed a well defined, unilocular radiolucency, measuring approximately 2.0x2.0 cm, with smooth corticated border associated with impacted tooth #34 in non-tooth bearing area of the mandible, close to the lower border [Table/Fig-2]. The lower cortical border of mandible was intact. No resorption of the root apices of the involved tooth as well as the adjacent teeth was seen. A provisional diagnosis of dentigerous cyst was made. The differential diagnoses of Adenomatoid Odontogenic Tumour (AOT), odontogenic keratocyst and unicystic ameloblastoma were considered. A conservative surgical excision of the lesion was carried out along with extraction of impacted first premolar (#34) under local anaesthesia. The postoperative course was uneventful and since six months, there were no signs of recurrence on a regular follow up.
Preoperative intraoral photograph showing missing tooth #34 and mild lingual swelling (arrow) and buccal vestibular obliteration.

Orthopantomogram showing well defined radiolucent lesion (arrow) associated with an impacted left mandibular premolar tooth #34.

On macroscopic examination, the excised specimen was roughly spherical in shape, soft to firm in consistency, well encapsulated and measuring approximately 2 cm in diameter along with the extracted premolar. On gross examination, the cut surface of the specimen had a thick fibrous light brown capsule surrounding the brownish black solid areas [Table/Fig-3]. The central areas showed small specks of white to off-white mineralized areas.
Macroscopic image of the spherical, soft tissue specimen with the cut surface showing central solid area (arrow) surrounded by light coloured thick capsule.

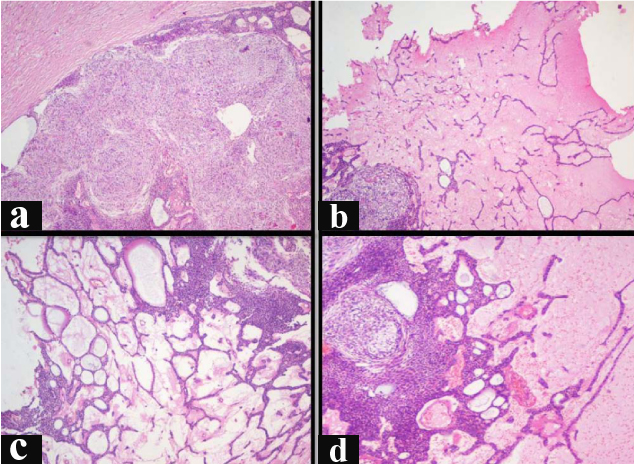
Microscopically, the H&E stained tissue sections revealed a well encapsulated lesional mass [Table/Fig-4a]. The lesional tissue consisted of equal amount of epithelial and connective tissue components [Table/Fig-4b]. The odontogenic epithelium is seen arranged in form of nests, strands, sheets, cribriform pattern, ducts, rosettes, whorls and reticular pattern. The nests were made up of 5-7 polygonal cells; and strands were made up of 15-30 polygonal cells and were seen mostly at the periphery of the lesion [Table/Fig-4b]. Areas of basaloid cells arranged in sheet configuration, with some areas showing cribriform pattern, were also seen [Table/Fig-4c,d]. The ducts, lined by tall columnar cells with long hyperchromatic nuclei, were either empty or contained eosinophilic coagulum or degenerated material [Table/Fig-5]. Whorls of odontogenic epithelial cells of spindle morphology arranged radially were seen [Table/Fig-4a]. Rosette pattern with central eosinophilic coagulum was also seen [Table/Fig-6]. Eosinophilic droplets of varying sizes were seen throughout the lesional tissue [Table/Fig-6]. Reticular arrangement, predominantly seen along the periphery of the lesion, consisted of polygonal cells arranged in net like pattern [Table/Fig-4c].
Photomicrograph showing a) Thick fibrous capsule along with lesional tissue showing presence of whorls, rosettes and few cribriform areas (H&E stain, 10X); b) Odontogenic epithelial cells in the form of nests, cords and strands and degenerated connective tissue (H&E stain, 4X); c) Odontogenic epithelial cells arranged in reticular pattern in degenerative connective tissue. Nests, strands and few solid areas are also seen (H&E stain, 10X); d) Odontogenic epithelial cells arranged in solid patterns showing cribriform areas. Adjacent degenerated stroma containing nests, cords and strands are also seen (H&E stain, 10X).
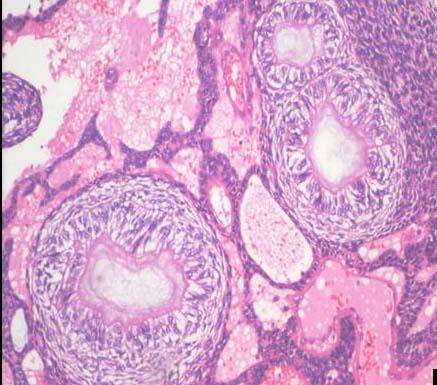
Photomicrograph showing ductal structures, lined by tall columnar cells with elongated nuclei, containing eosinophilic coagulum. The ducts are seen in solid and degenerative background (H&E stain, 20X).
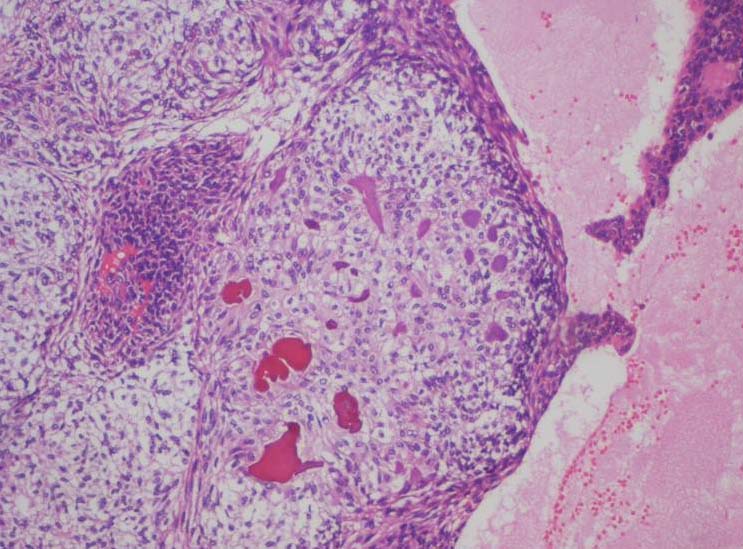
Photomicrograph showing several eosinophilic tumour droplets in tumour nodules composed of spindle shaped epithelial cells and also at the centre of rosette like structures (H&E stain, 10X).
The intervening connective tissue is predominantly degenerating and in some areas is hyalinised. Various stages of degeneration were seen with some areas being pale eosinophilic while others showed areas of clearing [Table/Fig-7a]. Few of the degenerated areas were seen adjacent to haemorrhagic areas [Table/Fig-7b]. Dilated and engorged endothelial lined blood vessels, some of which exhibited perivascular hyalinization, were seen [Table/Fig-8]. Areas of induction of dentinoid and osteodentin were seen in the lesional tissue [Table/Fig-9a-d]. Few areas showed hyalinization, dystrophic calcification and residual bone. Based on these findings, a final histological diagnosis of AOT with inductive changes was made.
a) Areas of degeneration in different stages. Some areas are homogenously eosinophilic while some areas show clearing (arrow) (H&E stain, 100X); b) Photomicrograph showing area of haemorrhage along with degeneration. The area is lined by odontogenic epithelial cells (H&E stain, 4X).
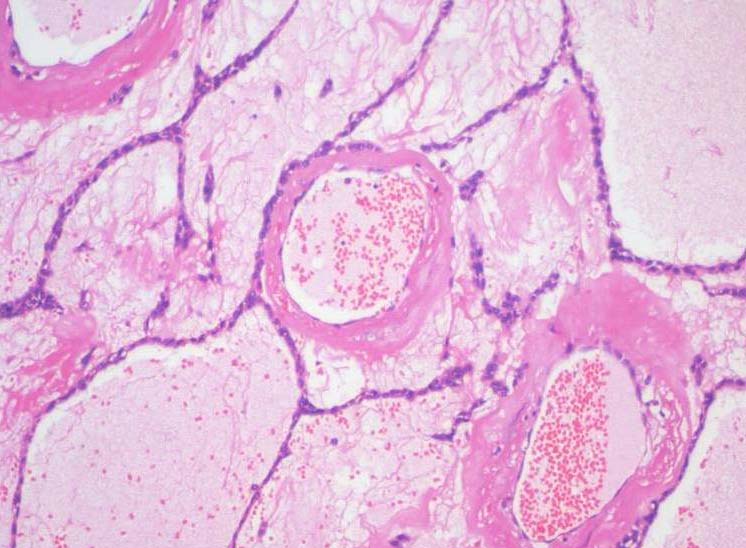
Perivascular hyalinization of dilated and engorged endothelial lined blood vessels in areas of degeneration. The degenerated areas show odontogenic epithelial cells in reticular pattern (H&E stain, 10X).
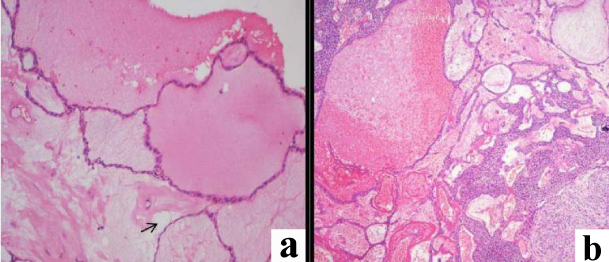
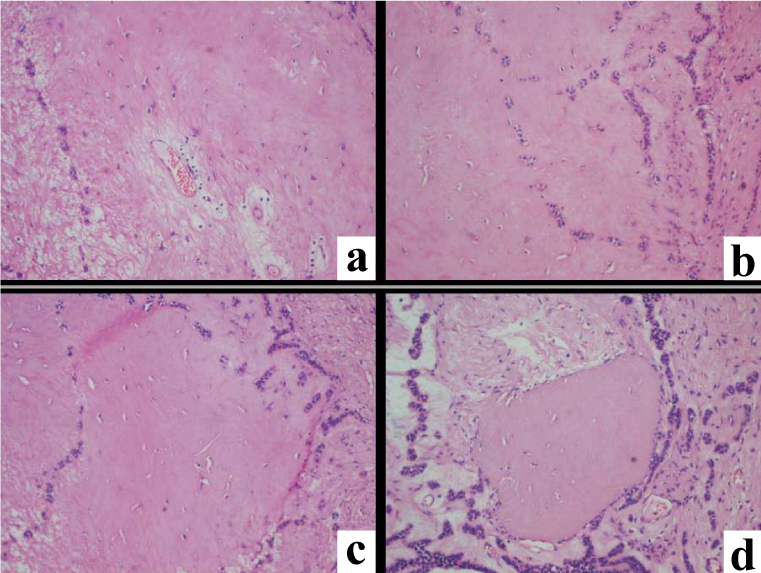
a) Areas of hyalinization along with induction of dentin like areas (H&E stain, 10X); b) Dentinoid seen as a homogenous eosinophilic area with entrapped mesenchymal cells and also odontogenic cells in the lacunae (H&E stain, 10X); c) Multiple clefts and lacunae in osteodentin, lined by odontogenic epithelial cells and ectomesenchyme (H&E stain, 10X); d) Well formed areas of osteodentin amidst odontogenic epithelial cells and ectomesenchyme (H&E stain, 10X).
In our case, the various histological variations were seen along with osteodentin and dentinoid material. These are infrequent findings which have been reported by Taketa Y in his studies [1]. This challenges the inclusion of AOT in first category of benign epithelial tumours in many instances and therefore requires further research.
It is hoped that the present and other reports of adenoid odontogenic tumours with osteodentin and dentinoid material will aid in determining the proper categorization of this tumour and address the inductive changes.
[1]. Takeda Y, Induction of osteodentin and abortive enamel in adenomatoid odontogenic tumourAnn Dent 1995 54(1-2):61-63. [Google Scholar]