Implication of Posture Analysing Software to Evaluate the Postural Changes after Corrective Exercise Strategy on Subjects with Upper Body Dysfunction-A Randomized Controlled Trial
Purushothaman Senthil1, S Sudhakar2, S Porcelvan3, T.G. Tilak Francis4, D Rathnamala5, R Radhakrishnan6
1 Research Scholar, School of Physiotherapy, Vel’s University, Chennai, Tamil Nadu, India.
2 Assistant Professor, Department of Arthroscopy and Sports Medicine, Sri Ramachandra University, Chennai, Tamil Nadu, India.
3 Professor, Department of Research committee, Saveetha University, Chennai, Tamil Nadu, India.
4 Professor, Department of Physiotherapy, Vel’s University, Chennai, Tamil Nadu, India.
5 Associate Professor, Department of Physiotherapy, Mohamed Sathak A J College of Physiotherapy, Chennai, Tamil Nadu, India.
6 Professor, Department of Physiotherapy, Mohamed Sathak A J College of Physiotherapy, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Purushothaman Senthil, 5/738, G2, JR Nilayam, Vignarajapuram 3rd Extension, Santhosapuram, Chennai – 600073, Tamil Nadu, India.
E-mail: senthilp101010@gmail.com
Introduction
The postural adaptation is very common now a days in school going children, office desk oriented job, computer users and frequent mobile users, and in all major industrial workers. Several studies have documented a high incidence of postural abnormalities in a given population; however, methods of postural measurement were poorly defined. The implication of postural pro software to analyse the postural imbalance of upper body dysfunction is very rare and literature studies says that the kinematic changes in particular segment will produce pain/discomfort and thereby lesser productivity of subjects.
Aim
To evaluate the postural changes in subjects with upper body dysfunction after a corrective exercise strategy using postural analysis software and pectoralis minor muscle length testing.
Materials and Methods
After explaining the procedure and benefits, informed consent was taken from the participating subjects (age 25-55 years). Subjects with upper body dysfunction were randomly allocated into two groups (each group 30 subjects). The Group–A received the corrective exercise strategy and Group-B received the conventional exercise for eight weeks of study duration (15 reps each exercise, total duration of 40 min; four days/week. Pre and Post posture analysis were analysed using posture pro software along with flexibility of pectoralis minor was assessed using ruler scale method.
Results
After interpretation of data, both the group showed the postural alteration and pectoralis minor muscle length changes, p-value (p<0.01) of both group showed highly significant changes. But comparing the both groups, the subjects who received the corrective exercise strategy shown more percentage of improvement in posture alteration (56.25%), pectoralis minor muscle length changes (68.69%) than the conventional exercise received subjects in posture alteration (24.86%) and pectoralis minor muscle length changes (21.9%).
Conclusion
Altered postural changes and pectoralis minor muscle flexibility before and after the corrective exercise strategy evaluated by postural analysis software method shown to be a significant tool in clinical practice, which is easier and reproducible method.
Intervention, Posture deviation, Pectoralis minor flexibility
Introduction
People will have habitual posture, such as slouching and crossing the legs, and they maintain a bad posture regardless of their recognition of incorrect posture and unable to maintain correct posture. These habitual postures may adapt and consider them comfortable, and this can cause strain on the spine, pelvis, muscles, tendons, joints, bones, and discs, which can lead to fatigue and deformation [1]. Thus, incorrect habits, such as excessive uses of computers, desks and chairs without proper height, lack of exercise, carrying heavy school bags, and inappropriate postures when studying or watching television, affect the musculoskeletal system and cause abnormal development, which prohibit the maintenance of correct posture [2]. Moreover, such a posture indicates an imbalance among the body parts owing to stress on the supporting structures of the body and prevents proper functioning of the structures of the body. This can cause problems in appearance as well as pain and physical disability [3]. Brown LT and few other researcher documented a high incidence of postural abnormalities in a young adult’s population; however, methods of postural measurement were poorly defined [4,5]. The upper body dysfunction is the component of discomfort over the neck, shoulder or scapular region which leads to poor performance of upper extremity function [6]. The postural abnormalities in upper body dysfunction is mainly due to underactive and overactive muscle adaptation in the neck, shoulder or upper back region for a long period which leads to several postural alterations like forward headed posture, rounded shoulder, kyphotic posture etc. Kyphotic deviation can even have deleterious effect on physical performance, the ability to perform activities of daily living, and overall quality of life [7]. The implication of postural pro 8 software to analysis the postural imbalance of upper body dysfunction is very rare and Martin AR et al., states that women with excessive kyphosis report more physical difficulty, more adaptations to their lives, and greater generalized fears [8] and community-dwelling men and women aged 65 years and older with excessive kyphosis report poorer satisfaction with subjective health, family relationships, economic conditions, and their lives in general [9].
The methods of evaluation of subject with upper body dysfunction using the posture analysis software are inadequate in the clinical practice.
However, not enough corrective exercise strategy for posture correction is available to the public with poor postural adaptation. Therefore, the present study aimed to evaluate the postural changes in subjects with upper body dysfunction after a corrective exercise strategy using postural analysis software and pectoralis minor muscle length testing.
Materials and Methods
The study was the randomized control trial with trial registered number CTRI/2016/08/007140 (www.ctri.nic.in). After the ethical concern was received from the Institutional based Ethical Committee from doctoral Committee, the study was conducted from August 2016 to January 2017 in Orthopaedic outpatient, Physiotherapy Department of Mohamed Sathak AJ College of Physiotherapy, Tamil Nadu, India. The sample size was calculated from the pilot study done among the subjects with upper body dysfunction interpreted results. Sixty subjects with upper body dysfunction of both genders between 25-55 years were included in this study. The effects of poor posture might be cumulative and therefore might increase in severity after the age of 35 years (Russek AS) [10].
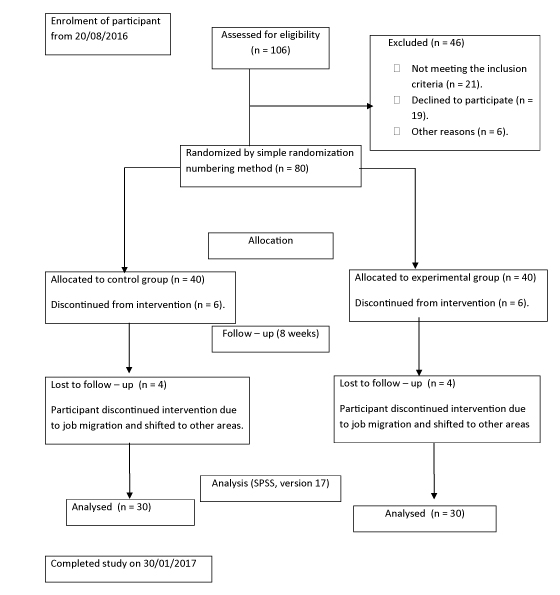
The subjects with any neurological problems like disc prolapse and stroke, any recent surgery and recent fracture or tumour around shoulder, neck and upper back region are excluded from the study. After explaining the procedure and benefits; informed consent was taken from the participating subject [Table/Fig-1].
Consort algorithm for subject allocation and data analysis of randomized, controlled trial.
Allocation of subjects into two groups was done by simple random numbering method. In subjects with upper body dysfunction, the kinematic alteration of shoulder, neck and upper back region will leads to postural adaptation. Later the muscle imbalance occurs because of these adaptations as stated by Janda’s approach of upper cross syndrome. Thus, we have framed the corrective exercise strategy with scapular stabilisation, deep cervical flexors endurance [Table/Fig-2] versus conventional exercise in control group [Table/Fig-3]. Thirty subjects in Group-A receives the corrective exercise strategy in two phases (In Phase-I starts with two weeks of warm-up exercise, passive stretching to upper trapezius, levator scapulae, sternocleido mastoid, pectoralis major and minor, lattismus dorsi, posterior capsule stretch, thoracic mobilization (using foam roller), isolated activation to middle and lower trapezius, rhomboids, serratus anterior, deep cervical flexors endurance training for four days/week with 15 reps/set of three sets, 40 min/day.
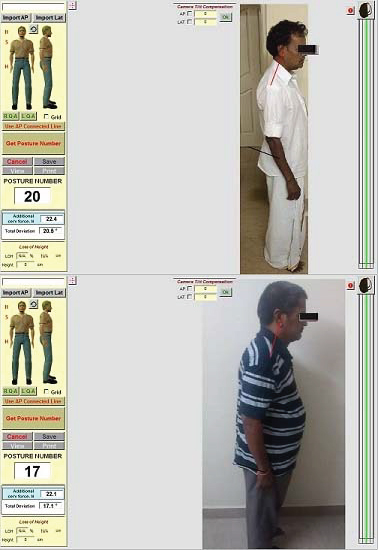
In phase-II, the gradual strengthening exercises for underactive muscles and reactive integration training for six weeks of total duration, four days/week with 15 reps/set of three sets, 40 min/day). 30 subjects in Group-B received the conventional exercise Free exercise to shoulder joint, pendular exercise for shoulder, active stretching of pectoralis minor and major muscles, isometrics exercise to neck and scapula, shoulder blade squeezing exercise, shoulder shrugging exercise, shoulder wall sliding exercise, relaxed breathing exercise for eight weeks of duration with 40 min/day, (15 reps/set) three sets and four days/week [11]. The high-intensity strength training with several different neck/shoulder exercises targeting the deltoids, upper trapezius, neck extensors etc. reported pain reductions corresponding to approximately 1–3 on a 10-point scale [11]. In scapular stabilisation exercise, the subject was prone lying and arm is moved upward in 90° and 120° of shoulder abducted position. Postural deviation of upper body dysfunction (forward headed posture, flat neck, shoulder protracted or retracted, kyphosis) can be assessed using posture software which will give the cumulative values of changes as posture number either in minus or plus value. Pre and post posture analysis were analysed using posture pro 8 software, where the subjects were requested to stand in a erect standing posture and the sagittal plane images were taken with the camera at 1.5 m distance from subjects and these photogrammetric images were incorporated in posture pro 8 software using window 10. In this software, the subjects image were uploaded and the posture number value is achieved by clicking on the subjects ear lobe, shoulder tip and greater trochanter of hip joint [Table/Fig-4] along with flexibility of pectoralis minor were assessed using ruler scale method, where the subjects are positioned in supine lying and the measurement of linear distance from the treatment table to posterior aspect of acromion process with average of three measurements were taken. This method of measuring the pectoralis minor muscle length testing have been proved by intra-reliability study in subjects with and without signs of shoulder symptoms by Lewis JS and Valentine RE 2007 [12].
Corrective exercise strategy (Group – A).
| Exercise protocol | Exercise regimen | Duration | Sets | Sessions |
|---|
| Phase – I(two weeks) | Warm-up exercise, passive stretching to upper trapezius, levator scapulae, sternocleido mastoid, pectoralis major and minor, lattismus dorsi, posterior capsule stretch.Thoracic mobilization (using foam roller). Isolated activation to middle and lower trapezius, rhomboids, serratus anterior, deep cervical flexors. | 40 minutes | Three sets(15 reps) | Four days/ week |
| Phase – II(six weeks) | Strengthening exercise and reactive integration. | 40 minutes | Three Sets(15 reps) | four days/ week |
Conventional exercise Protocol (Group B).
| Exercise protocol | Exercise regimen | Duration | Sets | Sessions |
|---|
| Phase – I(eight weeks) | Pendular exercise for shoulder.Free exercise to shoulder joint.Active stretching to underactive muscles.Isometrics exercise to neck.Shoulder blade squeezing exercise.Shoulder shrugging exercise.Shoulder wall sliding exercise.Breathing exercise. | 40 minutes | Three Sets(15 reps) | Four days/ week |
Postural evaluation of subjects using postural analysis software.
Outcome Measures
Postural deviation of subjects with upper body dysfunction using postural pro analysis software.
Flexibility of pectoralis minor muscle using muscle length test method.
Statistical Analysis
The data analysis was performed using SPSS statistical package for Social Science in Microsoft windows. The data were normally distributed and therefore parametric tests were performed. Descriptive statistics were presented as numbers and percentages. The data were expressed as Mean and SD. Independent sample student t-test/Mann-Whitney U test were used to compare continuous variables between two groups. Paired sample test/ Wilcoxon signed rank were used for ordinal data into within groups. A two sided p-value <0.05 was considered statistically significant.
Results
The baseline anthropometric data of subjects are presented in [Table/Fig-5]. After interpretation of data, both the group showed the postural alteration [Table/Fig-6] and pectoralis minor muscle length [Table/Fig-7] changes. A p-value (<0.001) of both group showed highly significant changes. But comparing the both groups the subjects who received the corrective exercise strategy shown more percentage of improvement in posture alteration (56.25%), pectoralis minor muscle length changes (68.69%) than the conventional exercise received subjects in posture alteration (24.86%) and pectoralis minor muscle length changes (21.9%).
Anthropometric data of subjects in each group (Mean ± SD).
| Characteristics of participant | Control group (N = 30) | Experimental group (N =30) |
|---|
| Male / Female | 14/16 | 12/18 |
| Age (years) | 50 ±4 | 52 ±4 |
| Height (cms) | 155±7 | 160±7 |
| Weight (kg) | 67±11 | 69±12 |
Posture number between experimental and control group.
| Posture number | Experimental group | Control group | Significant |
|---|
| Mean | SD | Mean | SD |
|---|
| Pre – Test | 17.60 | 4.19 | 16.73 | 2.87 | 0.355 (NS) |
| Post – Test | 7.70 | 3.82 | 12.57 | 2.55 | <0.001 *** |
NS – Not significant *** - Paired sample test/ Wilcoxon signed rank p < 0.001
Pectoralis minor length in centimeters between experimental and control group.
| Pectoralis Muscle Length (Centimetre) | Experimental Group | Control Group | Significant |
|---|
| Mean | SD | Mean | SD |
|---|
| Pre – Test | 9.55 | 2.33 | 9.17 | 2.21 | 0.517 (NS) |
| Post – Test | 2.98 | 1.09 | 7.15 | 2.16 | <0.001 *** |
NS – Not significant *** - Paired sample test/ Wilcoxon signed rank p < 0.01
Discussion
Postural education and assessments are a part of physical therapy education and clinical practice. The normal upright posture has been described as a state of balance requiring minimal muscular effort to maintain [13]. As kyphosis increases, there are certain alterations in the normal alignment that may cause pain and risk of dysfunction in the shoulder and pelvic girdle, and cervical, thoracic, and lumbar spine. Forward head posture, scapula protraction, reduced lumbar lordosis, and decreased standing height are often associated with hyperkyphosis [14]. The consequence of postural abnormalities can leads to pain and injury, postural education and correction have been used as treatment approaches [15,16]. Many study literature have shown a reasonable correlation between radiographic measurements and the placement of markers for measuring the abnormal posture and these method of the anatomical landmarks measuring postural abnormalities creates a possible use of photography as a form of scientific assessment (do Rosário JC 2013) [17]. Furlanetto TS et al., states that the photogrammetric method of evaluating the spine is a viable, valid and reproducible but still need more study literature [18]. Postural assessment through photography is a simple method that allows the acquisition of quantitative values to define the alignment of body segments [16]. The photographs provide valid and reliable indicators of the position of the underlying spine in sitting and the results of this study by Niekerk SM et al., the photograph Method can be used in practice as a valid measure of sitting posture [19]. In our previous case report study, we used to evaluate the upper body dysfunction of 94-year-old male subjects using posture pro 8 software and the significant percentage of kyphotic deviation changes occurs after the intervention [20].
The upper body dysfunction is defined as a muscular imbalance of upper part of the body which includes the chest, shoulders and neck musculature. The certain muscle group become tight and overactive, in turn the opposing muscles which are the mid and lower trapezius muscles (back musculature), serrates anterior (scapular stabilising muscles) and deep neck flexors become under-active and weak [21]. As this muscular imbalance persist for longer period, the subjects with upper body dysfunction become overloaded from their daily activities and will usually adapt to the activities they do the most, which results in the ‘tonic’ muscles becoming overactive, tight and adaptively shortening while the ‘phasic’ muscles becoming under-active, weak. These adaptive changes creates a poor posture around the neck, shoulder and upper back region which can be assessed by posture pro software analysis method. The protracted shoulder is associated with shorter pectoralis minor muscle [22]. Muscular imbalance can be corrected by strengthening of the posterior scapular stabilizers combined with stretching of the pectoral muscles can correct posture and maintain normal scapula-humeral rhythm [23]. The exercise is progressed in sitting and standing with resistance gradually [11]. The deep cervical endurance can be trained using the biofeedback unit initially in supine lying and progressed in sitting and standing [24].
In this study, the corrective exercise strategy includes the overactive tonic muscles have been passively stretched and the under-active phasic muscle have been strengthened in a progressive grades which is compared with the conventional exercise like isometric exercise and active free exercise. Interpretation of both the groups showed good progression in posture changes but more significant changes in the corrective exercise strategy group.
Conclusion
Scapular stabilisation exercise, deep cervical flexor endurance training, pectoralis minor and major muscle stretching, thoracic mobility exercise, breathing exercise and postural education were performed four times a week for eight weeks showed significant changes in the posture deviation and the pectoralis minor muscle length test. The software used to evaluate the postural changes before and after the interventions showed much differences which is correlated with the changes in the pectoralis minor muscle length flexibility. From this study, we conclude that the posture analysis software can be more viable and reproducible tool of evaluating the subjects with upper body dysfunction.
NS – Not significant *** - Paired sample test/ Wilcoxon signed rank p < 0.001
NS – Not significant *** - Paired sample test/ Wilcoxon signed rank p < 0.01
[1]. Carter JB, Banister EW, Musculoskeletal problems in VDT work: a reviewErgonomics 1994 37:1623-48. [Google Scholar]
[2]. Kim JK, Lee SJ, Effect of stretching exercise as work-related musculoskeletal pain of neck and shoulderJ Kor Alliance Health Phys Edu 2004 43:655-62. [Google Scholar]
[3]. Anderson CA, Harvey RJ, Discriminating between problems in living: an examination of measure of depression, loneliness, shyness, and social anxietyJ Soc Clin Psychol 1988 6:482-91. [Google Scholar]
[4]. Brown LT, A combined medical and postural examination of 746 young adultsAm J Orthop Surg 1917 15:774787 [Google Scholar]
[5]. Singer KP, A new musculoskeletal assessment in a student populationJournal of Orthopaedic and Sports Physical Therapy 1986 8:34-41. [Google Scholar]
[6]. http://alexeatly.com/upper-body-dysfunction/#sthash.oEUsUKO4.dpuf [Google Scholar]
[7]. Katzman WB, Wanek L, Shepherd JA, Sellmeyer DE, Age-related hyperkyphosis: its causes, consequences, and managementThe Journal of Orthopaedic and Sports Physical Therapy 2010 40(6):352-60. [Google Scholar]
[8]. Martin AR, Sornay-Rendu E, Chandler JM, Duboeuf F, Girman CJ, Delmas PD, The impact of osteoporosis on quality-of-life: the OFELY cohortBone 2002 31:32-36. [Google Scholar]
[9]. Takahashi T, Ishida K, Hirose D, Nagano Y, Okumiya K, Nishinaga M, Trunk deformity is associated with a reduction in outdoor activities of daily living and life satisfaction in community-dwelling older peopleOsteoporos Int 2005 16:273-79. [Google Scholar]
[10]. Russek AS, Diagnosis and treatment of scapula-costal syndromeJAMA 1952 150:2527 [Google Scholar]
[11]. Andersen CH, Andersen LL, Zebis MK, Sjøgaard G, Effect of scapular function training on chronic pain in the neck/shoulder region: a randomized controlled trialJ Occup Rehabil 2014 24:316-24. [Google Scholar]
[12]. Lewis JS, Valentine RE, The pectoralis minor length test: a study of the intra-rater reliability and diagnostic accuracy in subjects with and without shoulder symptomsBMC Musculoskeletal Disorders 2007 8:64 [Google Scholar]
[13]. Schwartz L, A resume, with comments, of the available literature relating to posturePublic Health Rep 1927 42:1219-48. [Google Scholar]
[14]. Balzini L, Vannucchi L, Benvenuti F, Benucci M, Monni M, Cappozzo A, Clinical characteristics of flexed posture in elderly womenJ Am Geriatr Soc 2003 51:1419-26. [Google Scholar]
[15]. Forrester-Brown MF, Posture as a factor in health and diseaseBr Med J 1926 1:690-93. [Google Scholar]
[16]. Ferreira EA, Duarte M, Maldonado EP, Bersanetti AA, Marques AP, Quantitative assessment of postural alignment in young adults based on photographs of anterior, posterior, and lateral viewsJ Manipulative Physiol Ther 2011 34(6):371-80. [Google Scholar]
[17]. do Rosário JL, Photographic analysis of human posture: A literature reviewJournal of body work and movement therapies 2014 18(1):56-61. [Google Scholar]
[18]. Furlanetto TS, Sedrez JA, Candotti CT, Loss JF, Photogrammetry for postural evaluation: A systematic reviewWorld Journal of Orthopedics 2016 7(2):136-48. [Google Scholar]
[19]. Niekerk SM, Louw Q, Vaughan C, Grimmer-Somers K, Schreve K, Photographic measurement of upper-body sitting posture of high school students: A reliability and validity studyBMC Musculoskeletal Disorders 2008 9:113 [Google Scholar]
[20]. Senthil P, Sudhakar S, Radhakrishnan R, Effect of thoracic correction exercises in upper body dysfunction of 94-year-old male participant – a case reportJournal of Clinical and Diagnostic Research: JCDR 2016 10(12):YD01-YD02. [Google Scholar]
[21]. Kendall FP, McCreary EK, Muscles: Testing and Function 1983 3rd edBaltimore, MdWilliams & Wilkins:112-113.:116:27C315 [Google Scholar]
[22]. Sahrmann SA, Diagnosis and treatment of movement impairment syndromes 2002 St.Louis, MOMosby Inc [Google Scholar]
[23]. Allegrncci M, Whitney SL, Irrgang JJ, Clinical implications of secondary impingement of the shoulder in freestyle swimmersJ Orthop Sports Phys Ther 1994 20:307-18. [Google Scholar]
[24]. Jull GA, Falla D, Vicenzino B, Hodges PW, The effect of therapeutic exercise on activation of the deep cervical flexor muscles in people with chronic neck painManual Therapy 2009 14:696-701. [Google Scholar]