Endoscopic Endonasal Approach of Blow Out Fracture Reduction- A Novel Technique
Vinod Felix1, Narendrakumar Veerasigamani2
1 Consultant, Department of Ear, Nose and Throat, SUT Hospital, Pattom, Trivandrum, Kerala, India.
2 Consultant, Department of Ear, Nose and Throat, Indoamerican Hospital, Vaikom, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Narendrakumar Veerasigamani, Consultant, Department of Ear, Nose and Throat, Indoamerican Hospital, Vaikom-686143, Kerala, India.
E-mail: dr.vinodfelix@gmail.com
Blunt trauma to orbit can lead to orbital blow out fracture. Computerized tomography of paranasal sinuses plays the main role in diagnosing it. Repairing the defect and restoring the orbital contents is a challenging task for the surgeon. Endoscopic endonasal approach in reduction of blow out fracture provides good cosmetic outcomes and grossly minimize surgical complications. We report a case of 18-year-old male presented with diplopia, restriction of eye movements and enophthalmos due to Road traffic accident. CT paranasal sinuses showed right side floor, medial orbital wall fracture with medial rectus muscle entrapment. We planned endoscopic endonasal approach to reduce the fracture and multilayered repair done using bone resected from choncha bullosa, fat and fascia lata. Patient relieved of symptoms post operatively without any complications.
Diplopia, Enophthalmos, Medial orbital wall
Case Report
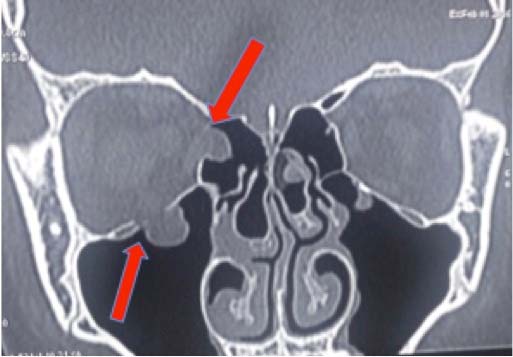
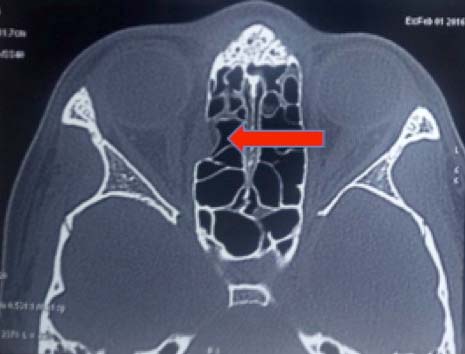
An 18-year-old male with the history of road traffic accident presented to ophthalmologist with right side diplopia, restriction of eye movements and severe ocular pain on movements. On examination patient had both vertical and horizontal diplopia, restriction of ocular movements and enophthalmos. Computerized tomography showed right side medial orbital wall fracture and medial rectus muscle entrapment, along with floor fracture without any muscle entrapment [Table/Fig-1,2]. The patient was given conservative treatment with parental antibiotics, oral analgesics and oral steroids. Vertical diplopia disappeared after one month duration. Apart from that other symptoms persisted. So, he was referred to us for further management. With the history, clinical examination and CT scan findings we planned endoscopic endonasal approach for reduction and restoration of orbital wall fractures.
Coronal cut showing fracture of medial orbital wall with medial rectus muscle entrapment and orbital floor fracture.
Axial cut showing fracture of medial orbital wall with medial rectus muscle entrapment.
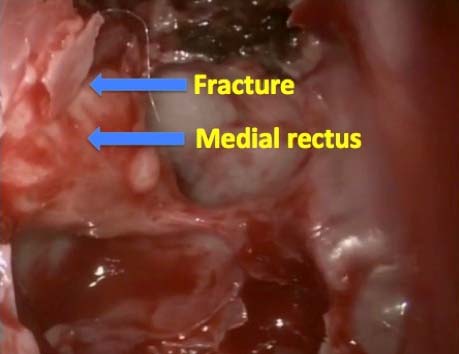
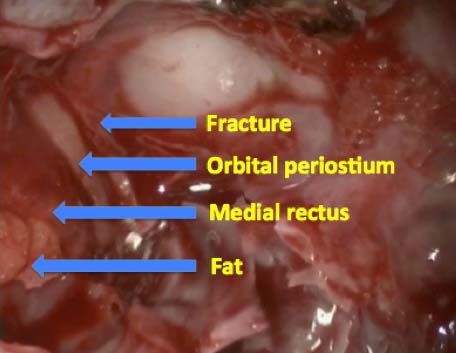
We started with resection of right side concha bullosa, middle meatal antrostomy. After removing the bulla, herniated medial rectus and orbital fat were clearly seen through the defect in lamina papyracea [Table/Fig-3]. The defect was enlarged to release the muscle entrapment and by applying pressure, the orbital fat herniating in the floor was reduced. The reconstruction of orbit was done multilayered. Fat harvested from thigh was kept over the medial rectus muscle [Table/Fig-4]. Fascia lata was tucked inside the defect [Table/Fig-5]. Bone of resected concha bullosa was placed over the fascia lata [Table/Fig-6] and foley’s catheter was inflated for further support. One more foley’s catheter was inflated in right maxillary sinus so that herniated fat in orbital floor was pushed into the orbit. Thus reconstruction was done for achieving normal restoration of orbit like thigh fat as orbital fat, fascia lata as orbital periostium and bone of concha bullosa as lamina papyracea. Postoperatively diplopia, restriction of ocular movements and enophthalmos disappeared completely [Table/Fig-7]. Both the foley’s catheters were removed after five days. Diagnostic nasal endoscopy and post op CT scans showed graft in situ and the entrapment of medial rectus muscle was released [Table/Fig-8,9].
Herniated medial rectus muscle and orbital fat.
Harvested fat kept over the medial rectus muscle.
Fascia lata was tucked inside the defect.

Bone of resected concha bullosa kept over the fascia lata.

Postoperatively no restriction of occular movements in all directions.

Coronal cut shows fracture was reduced well and fat in orbital fat was restored.

Axial cut shows graft in situ with entrapment of medial rectus muscle was released.

Discussion
An orbital blowout fracture is due to sudden rise of intracranial pressure in the orbit, which is followed by forceful impact on the orbit. The role of orbital reconstruction is to regain the orbital volume and its shape with suitable materials [1]. Smith first coins the term Blow out fracture in 1957 [2]. The incidence of the medial orbital wall fracture in orbital injury is about 0-10%, with a male-to-female ratio of 5:1 and most injuries involve the left orbit [3].
The symptoms of blow out fractures are diplopia, restriction of gaze, orbital pain and enophthalmos. The diplopia and restriction of gaze may be temporary, which subsides after few weeks of conservative treatment. But presence of enophthalmos is a valuable indicator for surgery when it is >2 mm [4]. The endoscopic endonasal approach gives great visualization of the fracture site, thereby helps to remove the bony fragments during reduction and reconstruction of orbital walls without a scar [5,6].
Among the orbital walls, weakest part is orbital floor because the bone is supported on each side but without support in the middle with thickness of 0.27 mm. In contract to orbital floor, medial wall is supported by numerous bony septa of ethmoid air cells making it strong enough not to fracture and deform easily [7]. So entrapment of the extraocular muscle between the fractures is less seen in medial orbital wall compared to floor of orbital wall. Comparing to vertical diplopia (from fracture floor of orbital wall), horizontal diplopia (from medial orbital wall fracture) can be easily adapted by patients [4].
The pathogenesis of pure blow out fractures can be explained in two theories [7],
Hydraulic theory- proposed by Pfeiffer in 1943 states that direct impact to the eyeball thereby increase in intaorbital pressure with hydraulic transmission and displaying the eyeball posteriorly [8].
Buckling theory- describes by Lefort states that impact strikes to any part of rim and force is transferred to the weak walls of orbit causing fracture and distortion [9].
Nolasco FP et al., classified medial orbital wall fractures into four types [3]. They are:
Type I- Pure medial wall fracture, Type II- Medial wall and floor fracture, Type III- Medial wall, floor and trimalar fracture and Type IV, Medial wall, orbital floor and complex fractures (i.e., maxillary, naso-orbital and frontal fractures).
The Type I and Type II fractures are probably explained by the hydraulic theory, whereas the Type III and Type IV fractures best fit with the buckling theory.
Eyeball symptoms like diplopia, vision disturbances and enopthalmos are more common with the Type I and Type II fractures where as hypoesthesia is noted with the Type III and IV fractures. Our case falls in Type II, as fracture site involves in medial wall and floor of the orbit.
Computerized tomography provides accurate diagnosis and surgical plan approach of blow out fractures. The various approaches for exploring blow out fractures are conjunctival approach, subciliary incision, medial brow incision, medial canthal incision, incision above and below the medial canthal ligament, open sky approach and the ethmoidal approach [10]. Two endoscopic techniques are transnasal and transorbital. The transnasal endoscopic technique is very precise for releasing entrapment of the intraorbital tissues without loss or damage to the orbital contents and gives better results. Moreover in local anesthesia, vision and extraocular movements of the patients with blow out fractures can be crosschecked whether it is rectified post surgerically [11]. Using synthetic materials prevents reherniation of orbital contents, like silastic sheet, hydroxyapatite ceramic, porous polyethylene sheet and titanium mesh implants are used, but their long time presence can induce granulation, resulting in failure rates. Autogenous grafts harvested from ribs, calvaria, iliac bone, or the maxillary sinus wall is also used [12]. A successful blow out fracture reconstruction depends on proper planning for surgical approach, precise surgical dissection and exact selection of type, size and contour of the reconstruction material [13].
In our case we used multilayered autogenous grafts like fat, fascia lata and conchal bone. As placing a cartilage/bone/silastic directly over exposed medial rectus muscle, would cause adherence of muscle to that and limitation of muscle movement. Here we have attempted to reconstruct the fracture, as in normal anatomy. So we layered few small fat pieces over the bare muscle like extraconal orbital fat, this would also help in tackling enophthalmos. For reconstructing orbital periosteum, fascia lata was used and conchal bone was used to reconstruct lamina papyracea thus providing great support and prevents reherniation of orbital contents.
Conclusion
Endonasal microscopic approach gave good results but there were limitations like difficulties in visualizing entire surgical field. This limitation was overcome by preferring the endonasal endoscopic approach along with angled endoscopes, which is excellent in visualization of clear delineation of all the fracture edges. It also enabled repositioning of all the prolapsed orbital contents and reconstruction of the orbital wall with cosmetically better by avoiding a scar.
[1]. Moon SJ, Suh HS, Park BY, Kang SR, Safety of silastic sheet for orbital wall reconstructionArch Plast Surg 2014 41:362-65. [Google Scholar]
[2]. Smith B, Regan WF Jr, Blow-out fracture of the orbit; Mechanism and correction of internal orbital fractureAm J Ophthalmol 1957 44(6):733-79. [Google Scholar]
[3]. Nolasco FP, Mathog RH, Medial orbital wall fractures: Classification and clinical profileOtolaryngol head neck surg 1995 112(4):549-56. [Google Scholar]
[4]. Sung YS, Chung CM, Hong IP, The correlation between the degree of enopthalmos and the extent of fracture in medial orbital wall fracture left untreated for over six months: A retrospective analysis of 81 cases at a single institutionArch Plast Surg 2013 40(4):335-40. [Google Scholar]
[5]. Gerbino G, Zavattero E, Viterbo S, Ramieri G, Treatment of orbital medial wall fractures with titanium mesh plates using retrocaruncular approach: Outcomes with different techniquesCraniomaxillofac Trauma Reconstr 2015 8(4):326-33. [Google Scholar]
[6]. Jin HR, Shin SO, Choo MJ, Choi YS, Endonasal endoscopic reduction of blow out fractures of the medial orbital wallJ Oral Maxillofac Surg 2000 58:847-51. [Google Scholar]
[7]. De Visscher JG, Van der Wal KG, Medial orbital wall fracture with enophthalmosJ Craniomaxillofac surg 1988 16(2):55-59. [Google Scholar]
[8]. Pfeiffer RL, Traumatic enophthalmosArch Ophthalmol 1943 30:718-26. [Google Scholar]
[9]. Le Fort R, Experimental study of fractures of the upper jawPlast Reconstr Surg 1972 50:497-506.:600-607. [Google Scholar]
[10]. Naraghi M, Kashfi A, Endonasal Endoscopic treatment of medial orbital wall fracture via rotational repositioningAm J Otolaryngol 2002 23:312-15. [Google Scholar]
[11]. Rajasekar MK, Vivek M, Narendrakumar V, Endoscopic endonasal approach of orbital medial wall reconstruction using septal cartilage: A rare surgical case reportClin Rhinol An Int J 2015 8(1):30-33. [Google Scholar]
[12]. Van der Wal KG, de Visscher JG, Bone grafting for enophthalmos due to a medial wall fracture: Case report with 13-year follow upJ Craniomaxillofac Surg 1999 27:177-79. [Google Scholar]
[13]. Gabrielli MF, Monnazzi MS, Passeri LA, Carvalho WR, Gabrielli M, Vieira EH, Orbital wall reconstruction with titanium mesh: Retrospective study of 24 patientsCraniomaxillofac Trauma Reconstr 2011 4(3):151-56. [Google Scholar]