Synovial Sarcoma of Palmar Aspect of Hand and Survival: A Rare Case Report
Tapan Kumar Sahoo1, Ipsita Dhal2, Saroj Kumar Das3, Saroj Kumar Das Majumdar4, Dillip Kumar Parida5
1 Senior Resident, Department of Radiotherapy, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India.
2 Senior Resident, Department of Pathology, Lady Hardinge Medical College and Associated Hospital, New Delhi, India.
3 Senior Resident, Department of Radiotherapy, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India.
4 Assistant Professor, Department of Radiotherapy, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India.
5 Professor, Department of Radiotherapy, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Saroj Kumar Das Majumdar, Assistant Professor, Department of Radiotherapy, All India Institute of Medical Sciences, Bhubaneswar-751019, Odisha, India.
E-mail: sarojmajumdar@gmail.com
Synovial sarcomas of the hand are extremely rare entities than most soft tissue sarcomas. The location at finger is further rarer than carpus of the hand. Synovial sarcoma of the hand/finger initially confused with many diagnoses such as myositis, haematoma, synovitis, tendonitis, bursitis, and other inflammatory lesions and therefore needs careful handling of the case with proper evaluation. We report a case of synovial sarcoma of the palmar surface of the right hand at interface of thumb and index finger in a 22-year-old female. The case was initially misdiagnosed as an abscess/haematoma of the finger 10 years back and treated with wide local excision. Synovial sarcoma was diagnosed on microscopic examination of excised specimen. Patient developed recurrent lesion twice locally. During first recurrence, the patient was treated with wide excision followed by radiotherapy and chemotherapy. Second recurrence was with bony destruction at the same site and below elbow amputation was performed.
Amputation, Outcome, Recurrence, Wide excision
Case Report
A 22-year-old female presented with chief complain of swelling over index finger of the right hand. She had past history of swelling at the right hand involving junction of index finger and thumb 10 years back, and the history showed initial presentation of a swelling over palmar surface of the right hand between thumb and index finger. The primary physician clinically suspected the case as an abscess with haematoma during that period. After receiving repeated course of antibiotics the size of the lesion gradually increased with hard in consistency. Wide local excision was performed. Histopathological examination revealed plump of spindle shaped cells with oval to spindle nuclei and moderate amount of pale cytoplasm, arranged in fascicles and present in a collagenous background showing features of grade-2 biphasic synovial sarcoma. Immunohistochemistry examination revealed cytokeratin and EMA markers positive confirming diagnosis of synovial sarcoma. Patient was on regular follow up by primary physician and developed recurrent lesion at the same location after six years. The patient was treated with local excision with wider margins without any regional lymph node dissection and received external beam radiotherapy of 50 Gy in 25 fractions to local area followed by boost of 10 GY in five fractions to tumour bed after field shrinking. She received six cycles of chemotherapy with ifosfamide (6 mg/m2) and adriamycin (60 mg/m2) combination regimen on every three weekly basis after completion of radiotherapy. The patient was on regular follow up and doing normal activity with the right hand.
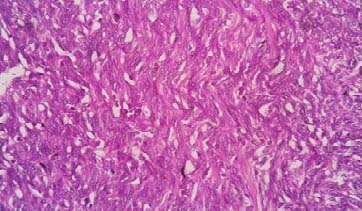
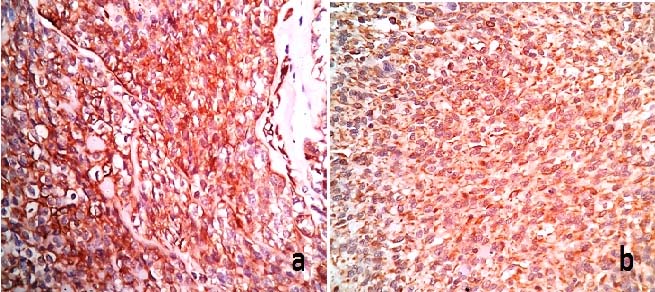
After three years of follow up, she reported to us with the recurrent lesion at the same location involving index finger of the right hand. On clinical examination, a hard globular mass of size 5 x 6 cm found in between thumb and index finger of palmar surface of the right hand [Table/Fig-1]. The lesion was non-tendered non-pulsatile and involved almost whole of the index finger. The patient was not able to do normal activity with the hand and she developed pain at rest. The MRI of the right hand showed a heterogeneous lobulated mass lesion of size 6.5 x 7.8 x 8.2 cm with poor definition of peripheral capsule, invading palmar aspect of flexor tendons, palmar arch extending up to inter metacarpal space and anterior aspect of wrist joint. Biopsy from the lesion showed features of biphasic synovial sarcoma [Table/Fig-2] with cytokeratin and EMA markers positive on immunohistochemical examination [Table/Fig-3]. Further systemic examination ruled out distant metastasis. Below elbow amputation was performed without any regional lymph node dissection. Histopathological examination of the operated specimen revealed features of biphasic synovial sarcoma with resected margin status negative of malignancy. The patient was planned for palliative chemotherapy with ifosfamide and adriamycin based regimen. However, the patient has not reviewed to us after surgery since last six months.
A growth of size approximately 5 x 6 cm in palmar surface of the right hand with soft tissue swelling extending up to wrist joint.

H&E (40X) microsection showing presence of tumour tissue arranged in vague fascicles with individual cells having oval to spindle nucleus and moderate cytoplasm with occasional mitosis.
a) Positivity of Pan-CK in the tumour cells (40X); b) Positivity of EMA in the tumour cells (40X).
Discussion
Synovial sarcoma is a rare mesenchymal tumour with aggressive behaviour and accounts for 5%-10% of all soft tissue sarcomas [1]. Lower extremity is the most common site (60%) with predilection for knee, followed by upper extremities (23%) and the head and neck region (9%) [2]. Majority of cases occurs in adolescents and adults between the age group of 15-40 years and rarely in children [3]. The incidence of synovial sarcoma is more in males than that of females with a ratio of 1.2:1, whereas, the incidence for different ethnicity is similar [3]. Soft tissue sarcoma of the hand is rare consisting of 1% among all adult malignancies and 2% - 4% of limb and trunk tumours [4,5]. There is only limited different histological types of soft tissue sarcoma exist in the hand and the most frequent variants among these are synovial sarcoma, clear cell sarcoma, and epithelioid sarcoma [5,6]. Synovial sarcoma of the hand comprises only of 8.5% among these and surgeons usually find one to two undiagnosed cases throughout their carriers [7,8]. However, location particularly over palmar surface is extremely rare and also digit involvement is rarer than involvement of carpus of hands [9]. The present case occurs at palmar surface of the hand particularly in the digit. Synovial sarcoma is one of the most misdiagnosed malignancies of the soft tissues, due to slow growing pattern, benign radiological features, change in size of the tumour, and pain similar to the traumatic pain [10]. Therefore, synovial sarcoma cases are initially diagnosed as myositis, haematoma, synovitis, tendonitis, bursitis, and others and delay in diagnosis is common [10]. The present case initially suspected as abscess or haematoma supporting the literature.
A slow-growing mass is the typical presentation of synovial sarcoma [7]. Due to rare location, 38% - 95% cases are treated by unplanned excision before referral to a specialist oncological centre [7]. Mostly, it arises from para-articular regions in close association with tendon sheaths, bursae, and joint capsules [8]. Synovial sarcoma does not arise from synovial cells. It arises from undifferentiated mesenchymal cell, and has capacity for double epithelial and spindle cell differentiation. Histologically, two major subtypes occur: monophasic variant and biphasic variant. These are defined by the presence or absence of epithelial components without any prognostic differences [2]. Majority of synovial sarcomas express cytokeratins, EMA, calponin, BCL-2, and CD-99 on immunohistochemical examination [9]. Vimentins are also expressed in spindle cells of these tumours. The features of imaging are nonspecific and biopsy is mandatory in all cases for confirmatory diagnosis [10]. Radiological investigations, particularly, MRI is the choice for diagnosis and staging of synovial sarcoma [11]. Imaging study is necessary to know the extent of the disease for surgical planning and to detect distant metastasis. There is no significant correlation between previous surgical excision and the risk of local recurrence or overall survival in synovial sarcoma [7]. Absence of distant metastasis at the time of diagnosis shows favorable outcome for synovial sarcoma of the hand as in our case [8]. The present case shows late recurrence and absence of distant metastasis with a 10-year survival. Primary tumour size and initial status at presentation strongly affects survival [9,10]. Literature shows nearly 80% of patients have local recurrence and/or distant metastasis [9]. Factors for higher risk of recurrences are older age, male sex, larger tumour size (>5 cm), trunkal location or proximal tumours of the limb, bone or neurovascular involvement, pathologically incomplete excision, high proliferative index, p53 overexpression, and SYT-SSX fusion types [9,12]. The probable cause of tumour recurrence in the present case is larger tumour size at the time of initial presentation.
Wide excisions followed by adjuvant radiotherapy and adjuvant chemotherapy are the treatment strategies for synovial sarcoma of the hand [8]. According to Gaurish SKS et al., regional lymph node dissection is not required for synovial sarcoma of the hand and also not performed in our case [8]. A 1 to 2 cm resection margins should be taken into consideration [10]. The role of adjuvant chemotherapy and its efficacy is still a question [9]. The adjuvant radiotherapy has a higher rate of local disease control, but without any benefit on survival rates [9,10]. The most commonly used drugs are ifosfamide and doxorubicin [9]. Several cases of synovial sarcoma were reported with recurrence and metastasis [2]. Lung is the most common site of distant metastasis [2]. The estimated five-year survival rate of synovial sarcoma is 27% to 55% [9,13]. Literature showed 10-year survival for distal tumours (hand and foot) was more in comparison to proximal extremities (65% vs 48%) [14]. According to Casal D et al., a 63-year-old women with a known case of synovial sarcoma of the hand after completion of surgery, chemotherapy and radiotherapy developed recurrence after a gap of eleven and half years without any distant metastasis, and died after twelve and half years of initial diagnosis [9]. The present case has two times local recurrence without any distant metastasis within a period of 10 years indicating good survival.
Conclusion
Synovial sarcoma of the hand mimics many other diseases like cystic lesions, myositis, haematoma, synovitis, bursitis, tendonitis, acute suppurative infections, etc. Therefore, synovial sarcoma should be ruled out while handing hand pathology, particularly in the young patient, due to commonly affected age group. Careful early diagnosis of the disease can improve survival rates. Due to the rarity of site of the disease, the long-term survival and prognosis of the disease is unclear and needs further evaluation.
[1]. Goldblum JR, Flope AL, Weiss SW, Malignant soft tissue tumours of uncertain typeIn: Enzinger & Weiss’s Soft Tissue Tumours 2013 6th ednPhiladelphiaElsevier:1052-1070. [Google Scholar]
[2]. Laila C, Ikram B, Mohamed S, Abdelkrim D, Siham T, Abdelmajid M, Synovial sarcoma of hand presenting as a cystic massOpen Journal of Orthopedics 2012 2:59-61. [Google Scholar]
[3]. Sultan I, Rodriguez-Galindo C, Saab R, Yasir S, Casanova M, Ferrari A, Comparing children and adults with synovial sarcoma in the surveillance, epidemiology, and end results program, 1983 to 2005: an analysis of 1268 patientsCancer 2009 115:3537-47. [Google Scholar]
[4]. Morrison BA, Soft tissue sarcomas of the extremitiesProc (Bayl Univ Med Cent) 2003 16:285-90. [Google Scholar]
[5]. Pradhan A, Cheung YC, Grimmer RJ, Peake D, Al-Muderis OA, Thomas JM, Soft-tissue sarcomas of the hand: oncological outcome and prognostic factorsJ Bone Joint Surg [Br] 2008 90B:209-14. [Google Scholar]
[6]. Outani H, Hamada K, Oshima K, Joyama S, Naka N, Araki N, Clinical outcomes for patients with synovial sarcoma of the handSpringer Plus 2014 3:649 [Google Scholar]
[7]. Murray PM, Soft tissue sarcoma of the upper extremityHand Clin 2004 20:325-33. [Google Scholar]
[8]. Gaurish SKS, Avinash J, Kulkarni M, Patel DS, Zode AB, A rare case of monophasic synovial sarcoma of the hand: Cytological and immunohistopathological studyOncology, Gastroenterology and Hepatology Reports 2015 4(2):116-18. [Google Scholar]
[9]. Casal D, Ribeiro AI, Mafra M, Azeda C, Mavioso C, Mendes MM, A 63 year old woman presenting with a synovial sarcoma of the hand: A case reportJ Med Case Rep 2012 6:385 [Google Scholar]
[10]. Siegel HJ, Sessions W, Casillas MA Jr, Said-Al-Naief N, Lander PH, Lopez-Ben R, Synovial sarcoma: clinicopathologic features, treatment, and prognosisOrthopedics 2007 30:1020-27. [Google Scholar]
[11]. Garg PK, Mohnaty D, Jain BK, Goel S, Singh B, Giant subcutaneous synovial sarcoma: An interesting caseJ Clin Diagn Res 2013 7:3014-15. [Google Scholar]
[12]. Wolden SL, Alektiar KM, Sarcomas across the age spectrumSemin Radiat Oncol 2010 20:45-51. [Google Scholar]
[13]. Athanasian EA, Bone and soft tissue tumoursGreen’s Operative Surgery 2011 Volume 2PhiladelphiaChurchill Livingstone:2141-2191.Edited by: Wolfe SW, Hotchkiss RN, Pederson WC, Kozin SH [Google Scholar]
[14]. Deshmukh R, Mankin HJ, Singer S, Synovial sarcoma: the importance of size and location for survivalClin Orthop Relat Res 2004 419:155-61. [Google Scholar]