The prime requisite of a sound and holistic prosthodontic rehabilitation from both the patient’s and clinician’s perspective is to be able to satiate the yardsticks of function, retention, aesthetics and comfort to the fullest. It is thereby astoundingly hard to digest that speech being an indispensably significant function of the complete denture prosthesis, is often seen upon as heedless and inconsiderate by the patient. Adaptability in speech pronunciation of complete denture prosthesis is a subjective phenomenon; cannot be predicted to entirety. To diagnose and verify speech difficulties in a complete denture patient who finds it relatively difficult to affirm to new palatal contours of prostheses, we require some simple clinical aids.
Palatogram is a fairly simple, yet highly efficacious technique of assessment and verification of palatal contours, so as to improve and correct the existent speech deficiencies of affected sounds. In the present case report, readily available food colour in spray form was employed to produce and investigate inadequacies of various sounds. This case report highlights palatogram as an easy clinical technique that helps to correct, often delinquent speech difficulties, pertaining to the palatal contours of complete denture prosthesis.
Case Report
A 52-year-old male patient, with an occupational background of teaching in a secondary school reported to the Department of Prosthodontics with a presenting complaint of unsatisfactory levels of pronunciation and speech. Upon eliciting past dental history, he revealed of getting rehabilitated with complete dentures in the department of prosthodontia a month ago, with satisfactory aesthetics and function, however he continued to have speech problems with regards to the pronunciation. His altered speech was a matter of grave embarrassment for him, as it was reflected in his undermined performance while delivering lectures. After a thorough sequential diagnosis and excluding pertaining anatomical factors that could have resulted in his altered speech, it was concluded that the improperly carved palatal contour of the maxillary complete denture was the root cause for it. This case report narrates a technique of applying palatogram as a practical implication for customizing the palatal contour of a maxillary complete denture, with auto-polymerizing acrylic resin to improve the speech clarity.
Procedure
To commence with, patient was asked to pronounce all the words starting with consonants sounds for example s, sh, ch, n, k etc., because he specifically experienced a profoundly erroneous alteration in consonant speech, ever since the delivery of prostheses. An audio of those sounds were further recorded. He was then trained to pronounce these sounds individually and open the mouth without tongue contacting against the palate. Vowel “O” was merged with the consonant to be recorded, even though their combination is not a word; i.e., for listening him utter “k”, we used “ko”; for “ch”- “cho” and so on. Likewise it was combined with other consonants to avoid multiple graphic recordings [1].
Next the maxillary complete denture was evenly and uniformly sprayed with green coloured liquid, obtained by mixing edible food colours [Table/Fig-1]. Green colour was specifically chosen, as it imparted visually appreciable contrast against denture base. It was then inserted in patient’s mouth and correctly seated, taking appropriate caution that the sprayed palate did not touch elsewhere, before the sound was pronounced. Patient was asked to repeat the desired sound twice in a consecutive manner, during which definite palatal contact was confirmed by close observation. Patient was instructed to avoid any further deliberate tongue contact to the palate. Denture was carefully retrieved without perturbing the obtained palatal record. Palatogram of the sounds were generated by the action of tongue, wiping away the sprayed colour film, forming definite patterns during speech.
Evenly sprayed palatal area with green food colour liquid which immediately dries.

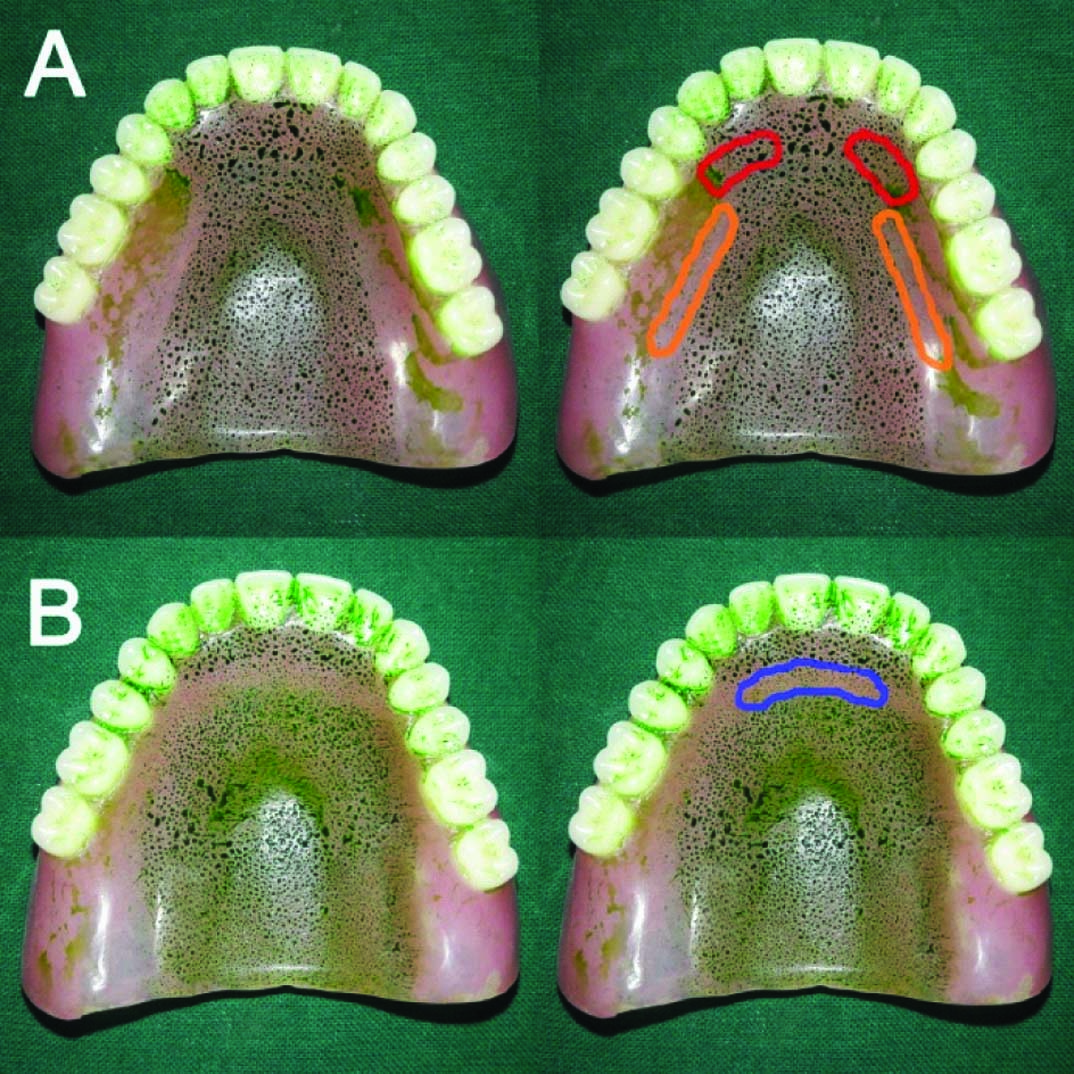
Defective sound palatograms so obtained were compared for reference with definite patterns of every sound. Lesser wipped off zones of green film while pronouncing “S” and “T” words, were indicative of incongruous tongue contacting against the palate, hinting at under-contoured palatal contours in the anterior segments, while broad smudge recorded over posterior slopes of palate reflected a heavy contact, thus pointing towards an over-contoured palate in those areas. Over and under-contours of palate were rightfully outlined and demarcated for easier identification and correction [Table/Fig-2]. Over-contoured region (posterior palatal slope) was then selectively relieved using acrylic trimming bur as a remedial measure [Table/Fig-3].
Palatograms for “s” and “T” sounds.
A. Red outlined area shows under- contoured palate while orange outline shows over-contoured area.
B. Violet outlined area shows under-contoured part of palate.
Over contoured area is selectively trimmed.

The next line of correction was to achieve adequacy in palatal contour, with regards to the normal “s” curve after gauging the extent of deficiency. Homogenously kneaded coloured dough of tissue conditioning material (Mollosil, Detax, Germany) was spread over the outlined deficient area of the anterior palate. After denture insertion, patient was asked to repeat the defective sounds “so”, “to”, “sho” repeatedly for 10 minutes at a faster rate, so as to record the tongue activity during speech. The bulk of tissue conditioner was contoured to functional anatomy by tongue and a customized anterior palate was obtained [Table/Fig-4]. After validating the clarity of sibilant sounds, denture was removed from patient’s mouth. Waxed trial denture was processed normally after this maneuver.
Tissue conditioner with added red colour for contrast adapted to deficient area after prolonged speech.

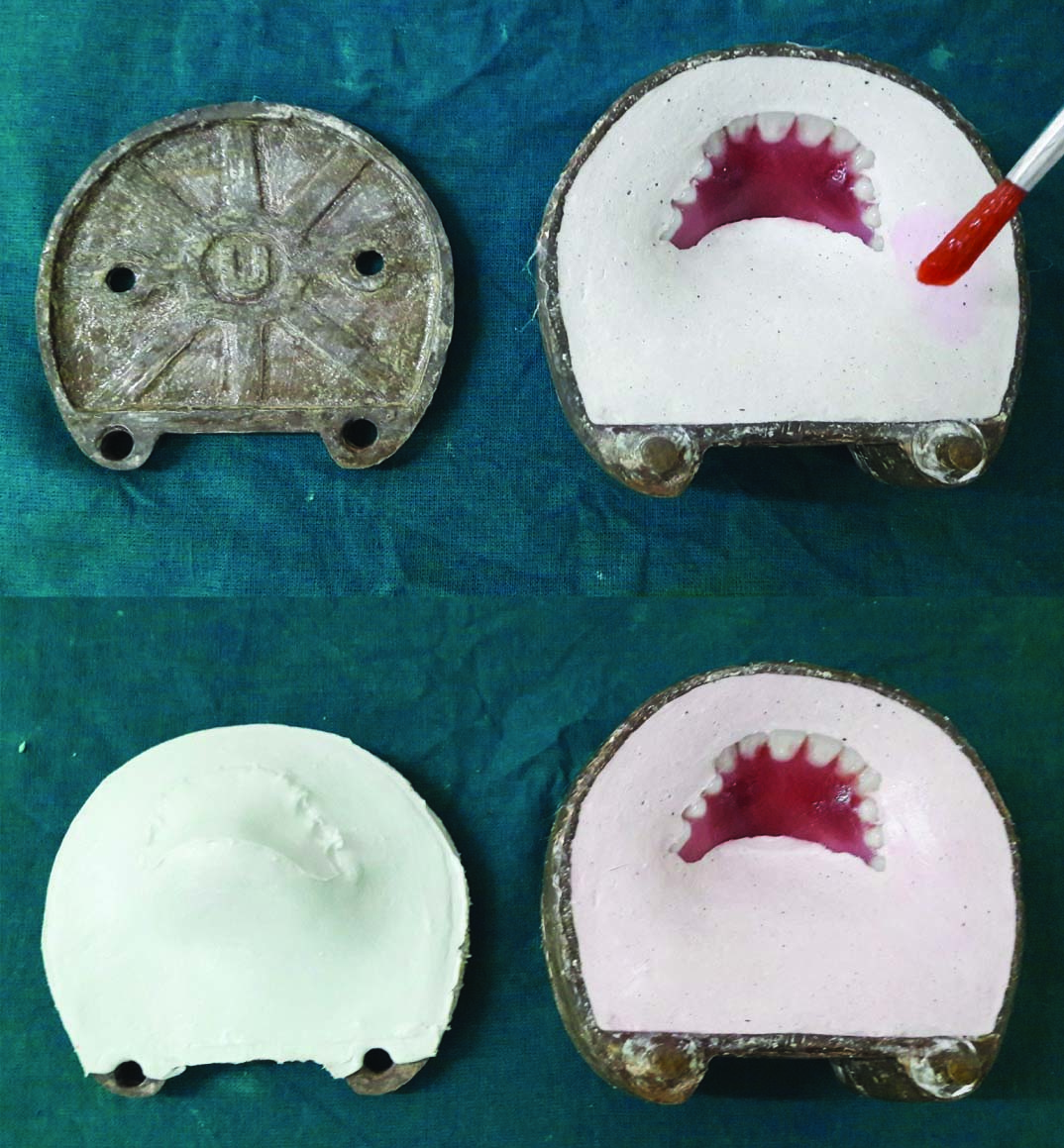
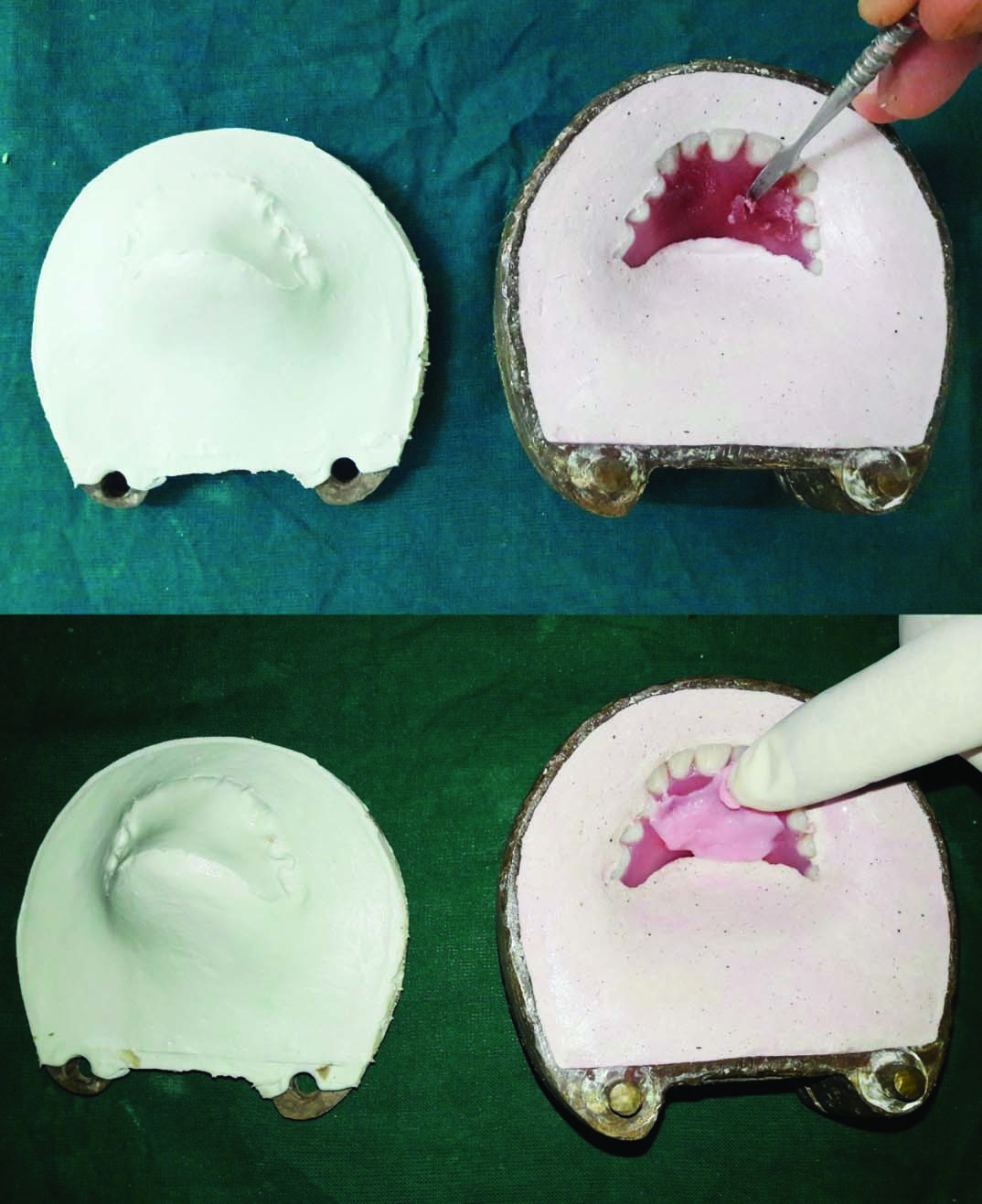
Petroleum jelly was applied onto intaglio surface of denture and was poured by dental plaster for easy retrieval. This poured denture was then flasked in such a way that plaster covered all the parts of denture except the area where tissue conditioner was applied. Uniform layer of cold mould seal was applied over the set plaster surface and was left to dry. Upper lid of flask was then placed and plaster was poured to generate the key-way [Table/Fig-5]. After setting of plaster, key-way was separated to remove the tissue conditioner using carver.
Denture with customized palate flasked with plaster and a plaster key-way prepared.
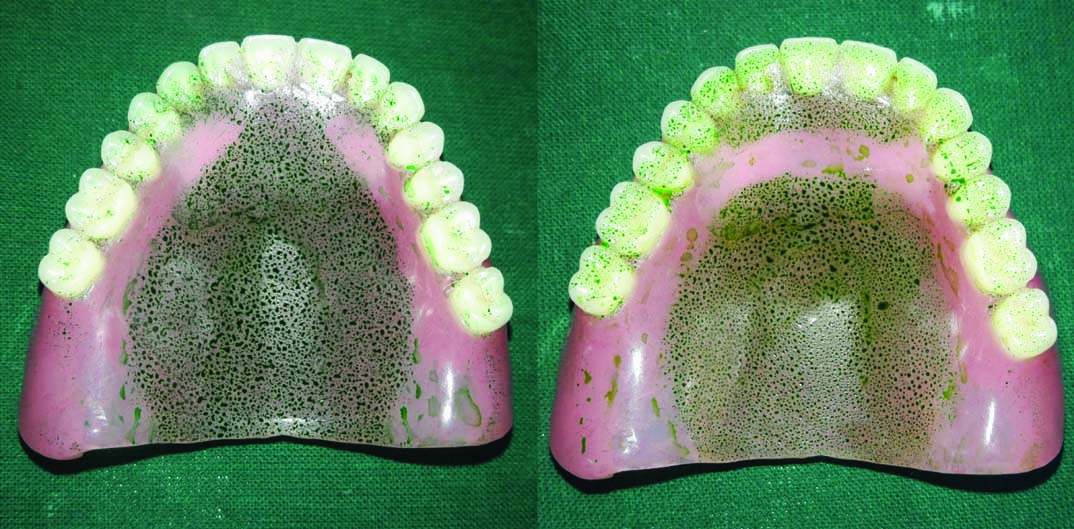
Auto-polymerizing acrylic resin was mixed and its optimized amount of mixture was placed in the space created, and the key-way was subsequently closed over it [Table/Fig-6]. Entire flask assembly was placed under bench press to squeeze out excess resin flash. Denture was carefully retrieved upon completion of polymerization. Edges of the added increment was finished using carbide burs, and customized palatal contour was polished with light pressure to yield a glossy surface [Table/Fig-7]. Intelligibility of s and sh sounds were evaluated again with the reformed denture’s palatal contours subjectively using audio records, as well as by using palatogram [Table/Fig-8].
Tissue conditioner removed and dough of auto-polymerised resin added to deficient area.
Polished denture with functional palate with polymerised resin in deficient area.

Verified palatograms for “S” and “T” sounds.
Discussion
Tongue and hard palate are rightly considered upon as speech enunciators as they add distinctness, and efficaciously aid in articulation of various sounds. Tongue acts as prime articulator for consonants. To effectuate pronunciation of vowels, it congruently changes its shape and size with little or no contact with specific areas of the teeth, alveolar ridge and hard palate [2].
Anterior teeth positioning, occlusal plane, vertical dimension of occlusion and palatal contour altogether, work on tandem and ensure optimum phonetics in complete denture. Palatal contour thus remains as the sole factor influencing speech, when other three factors are physiologically and mechanically accurate or well compensated [2,3]. Proper pronunciations require accurate approximation of tongue with the palatal contour. Intelligible speech, especially the sibilant sounds, requires normal motor function of tongue musculature and a customized palatal contour having dynamic tongue impression. In treatment with complete dentures, aesthetics, function, retention and comfort are harped upon at every step of denture fabrication, but phonetics is more often than, mistakenly an ignored facet! [4,5].
Usually an acclimatization period of few weeks is stipulated for adaptation towards achieving and executing good phonetics [1,6,7]. However, elderly patients often take a longer period, quite understandably so, because of the altered neuromuscular co ordinations or some of them continue to fumble around and falter with their altered state of speech thereafter [6]. Sibilant sounds are usually affected more due to non physiological palatal contours of newly delivered prosthesis [2-4,8].
Sounds of consonants affected by palatal contour exclusively and their manner of production in Hindi and English are shown respectively [9].
Palatal श /sh/ (ship), ष /sh/ (shut) and र /r/ (rust) {fricatives}
च /cha/ (chirp), छ /chha/ , ज /jj/ , झ /jh/ , क्ष /ksh/ {affricatives}
Linguo alveolar स /s/ (sun), ल /l/ (love)
Palatal Z(azure), ch (chat), j (jump)
Linguo alveolar s (sun), z (zebra)
Unblemished phonetics necessitates the tongue to seal the posterior palatal denture surface and direct a flow of air anteriorly, against an alveolo-palatal prominence, beginning at the premolars, which becomes progressively thicker around molars. This prominence is missing in majority of delivered maxillary prosthesis [2]. Tongue approximates the lateral palatal alveolar region of posterior maxilla during /s/ sound articulation to form a medial groove on its dorsal surface behind central incisors. Anterior and lateral palatal area contours thus determine the stream of air ejected through that groove and hence pronunciation of sibilant /s/ and /sh/ sounds [1,2,4,7,8]. /S/ sound is heard or perceived as a frontal lisp and whistle if the anterior palatal area is over-contoured or under-contoured respectively depending on degree to which air stream is impeded [4,10].
Tanaka H inferred that a reverse “S” curve exists in the natural anterior palate, in sagittal section from the study of the relationship between palatal contour and speech intelligibility. Palatal contour being crucial for pronunciation of the “S” and “SH” sounds were not found to be accurate in majority of maxillary complete denture. Sounds “T,” “D,” “N”and “L,” are produced when the tongue is placed firmly against the anterior hard palate [7]. Premature contact due to excessive thickness in anterior area can result in the “T” sounding like a “D” [2,4].
A palatogram is a static record of tongue and palatal contours of the maxillary complete denture during sound articulation which can be diagnostically used as a simple test for phonetics evaluation [2,4,11].
Similar palatogram patterns are achieved from every individual for a given sound which can be used as reference. The uniqueness of the patterns in different individuals, so generated can be attributed to anatomic variations like tongue size, arch shape and size and palatal contours [2]. Palatograms serve as a guiding force for alterations and customization of palatal contours, such that, speech deficiencies of sibilant sounds are corrected, or the period of adaptation to new prosthesis gets reduced [12].
Pronunciation of the consonant sounds alone involves merging two or more sounds, for example, when pronouncing the “T” sound, the vowel sound “ee” is also hiddenly coupled up. Thus, two or more palatal contacts are made, and it becomes cumbersome to record palatogram of any consonant alone. As per Allen’s protocol, “o” is the only vowel whose articulation consistently does not involve tongue touching the palate [13]. It was combined with other consonants to achieve an accurate singular consonant palatogram, even though the combination might not yield up a proper word.
In the course of our case report, over-contoured regions, diagnosed and marked using palatogram were selectively trimmed and verified again using palatogram for obtaining a restructured functional palatal contour. Auto-polymerizing acrylic resin was used to correct the deficient palatal areas by virtues of its ease of handling, time saving maneuver, inexpensive nature and dimensionally stability. The lateral palatal contours, as such is a low-stress region, thus mechanical and aesthetic properties (adhesive strength and colour stability) of auto-polymerizing acrylic resin are adequate enough for facilitating such corrections. Alginate, impression waxes and tissue conditioners are the materials of choice to gauge deficiencies of palatal contours at try in and follow up visits. Many other mediums like occlude aerosol, pressure indicating paste, gothic arch tracing ink and gypsum products can be used to record palatogram. Patient’s demand of using an inert and safe recording material encouraged author to use food colour. Its green colour was in contrast to denture and had an added psychological benefit of being non-hazardous even if accidentally swallowed by patient.
Conclusion
Thereby to put in a nutshell, initial deviations from natural speech soon after prosthetic rehabilitation is quite a normal occurrence, and thus for better comparison, pre-treatment speech assessment is necessary. Patient’s adaptability should be improved by conditioning them about such immediate speech aberrations, and when encountered, they ought to be justifiably corrected. Palatogram plays an indispensable diagnostic role in identifying such discrepancies, and verification of the corrected palatal contours. Being an easy, simple and inexpensive technique, it is very useful in patients with speech difficulties of complete denture patients.
[1]. Allen LB, Improved phonetics in denture constructionJ Prosthet Dent 1958 8:753-63. [Google Scholar]
[2]. Farley DW, Jones JD, Cronin RJ, Palatogram assessment of maxillary complete denturesJ Prosthodont 1998 7:84-90. [Google Scholar]
[3]. Sharry JJ, Complete denture prosthodontics 1974 3rdNew YorkMcGraw-Hill:130-148. [Google Scholar]
[4]. Hansen CA, Singer MT, Correction of defective sibilant phonation created by a complete maxillary artificial dentureGen Dent 1987 35:357-60. [Google Scholar]
[5]. Terrell WH, Fundamentals important to good complete denture constructionJ Prosthet Dent 1958 8:740-52. [Google Scholar]
[6]. Zarb GA, Bolender CL, Eckert S, Jacob R, Fenton A, Mericske-Stern R, Prosthodontic treatment for edentulous patients: complete dentures and implant-supported prostheses 2003 12th edSt. LouisElsevier Health Sciences:386-7.:417 [Google Scholar]
[7]. Tanaka H, Speech patterns of edentulous patients and morphology of the palate in relation to phoneticsJ Prosthet Dent 1973 29:16-28. [Google Scholar]
[8]. Runte C, Lawerino M, Dirksen D, Bollmann F, Lamprecht-Dinnesen A, Seifert E, The influence of maxillary central incisor position in complete dentures on /s/ sound productionJ Prosthet Dent 2001 85:485-95. [Google Scholar]
[9]. Jain AR, Venkat Prasad MK, Ariga P, Palatogram revisitedContemporary Clinical Dentistry 2014 5:138-41. [Google Scholar]
[10]. Palmer JM, Structural changes for speech improvement in complete upper denture fabricationJ Prosthet Dent 1979 41:507-10. [Google Scholar]
[11]. The glossary of prosthodontic termsJ Prosthet Dent 2005 94:59 [Google Scholar]
[12]. Adaki R, Meshram S, Adaki S, Acoustic analysis and speech intelligibility in patients wearing conventional dentures and rugae incorporated denturesThe Journal of Indian Prosthodontic Society 2013 13(4):413-20. [Google Scholar]
[13]. Rothman R, Phonetic considerations in denture prosthesisJ Prosthet Dent 1961 11:214-23. [Google Scholar]