Hypothyroidism is one of the most common endocrine disorders in India with a prevalence ranging from 3.9% to 10.95% [1,2]. It has been recognised that general awareness about hypothyroidism in India is poor and is associated with inadequate knowledge, wrong beliefs and practices in a significant proportion of patients [3]. The lacunae observed about knowledge and practices amongst the hypothyroid patients have resulted in several misconceptions, poor compliance and suboptimal management [3,4].
One of the important factors contributing to this gap observed is the lack of qualified physicians for treating hypothyroidism. Inadequate time spent by doctors for patient education is another contributing factor. Patient related factors include inadequate education, social beliefs and incorrect information acquired from the internet. Previous studies have consistently shown that knowledge, awareness and practices in hypothyroidism patients are impaired [3-5]. However, the previous studies from southern part of India have evaluated smaller cohorts and have shown great deal of variation in the extent of impairment of knowledge and practices in hypothyroid patients [6,7]. In addition, a comprehensive assessment on all the aspects of hypothyroidism was not considered in these studies. The present study was aimed to make a comprehensive assessment of gaps in the knowledge, faulty practices and misconceptions prevalent among a large cohort of hypothyroid patients from south India.
Materials and Methods
The present cross-sectional study was conducted at Vydehi Institute of Medical Sciences and Research Centre, Bengaluru, India, over a period of one year, from October 2015 to October 2016. A total of 244 consecutive patients for treatment of hypothyroidism were enrolled in the study. With the expected prevalence of 10% for hypothyroidism, a sample size of 244 was required to provide a confidence interval of 99%.
The study included primary hypothyroid patients with age more than 18 years, who were on treatment from at least last six months and were visiting the endocrinology OPD for the first time. Our study excluded patients who were newly diagnosed with hypothyroidism, who had a known secondary cause of hypothyroidism, history of neck irradiation, previous thyroid surgery, radio ablative therapy and who were incapable of answering or had a disease with significant mental retardation.
A structured questionnaire was prepared and used to assess data on the following:
Patient’s knowledge of the disease.
Common beliefs and misconceptions associated with hypothyroidism.
Practices followed with regard to the methods of medication intake and patient follow up.
The questionnaire had a total of 26 questions covering the above-mentioned aspects. The data collection form was divided into two sets of questions, wherein the first set of 14 questions was used to assess the knowledge of patients regarding hypothyroidism and the second set of 12 questions was used to assess the practices followed by the hypothyroid patients with regard to medication use and follow up [Appendix].
Patients were asked to fill the questionnaire during their routine OPD visit. For those patients who were not well versed in English, the questionnaire was read out in their own vernacular language and their responses to the questions were marked accordingly. Institutional Ethical Committee approval was taken for the study and a written informed consent was obtained from all the patients.
Statistical Analysis
The data was collected and tabulated using Microsoft Excel 2007 and was reported as mean, percentages and frequencies.
Results
The mean age of the study population was 36.6±12.2 years. The male to female ratio was 1:4 (49 versus 195). The mean age of female patients was 36.79±12.5 years and of male patients was 35.02±12.1 years. The mean duration of hypothyroidism was 6.14±14.3 years. The overall mean Thyroid Stimulating Hormone (TSH) was 6.1±7.4 µIU/ml. The study involved 76 patients (31.14%) who had attended primary school or less, 120 patients (49.18%) had attended secondary school and 48 patients (19.6%) were graduates.
In the present study, 161 patients (65.9%) had correctly identified the term ‘thyroid’ as a gland while 20.9% had misunderstood the term either as a swelling in the neck or as a disease involving neck. A total of 13.2% patients did not know the meaning of the term ‘thyroid.’ When asked about the location of thyroid gland in the body, 150 patients (61.4%) correctly knew that it is located in the neck, whereas 79 patients (32%) falsely thought it is present in the chest. While 5 patients (2.04%) thought it was located in the abdomen and 10 patients (4.09%) were totally unaware. When questioned about the facts of hypothyroidism, 100 patients (40.98%) were aware that hypothyroidism denotes decreased functioning of the thyroid gland, while 141 patients misunderstood hypothyroidism as either increased thyroid function (45 patients, 18.4%) or as swelling in the neck (99 patients, 40.6%).
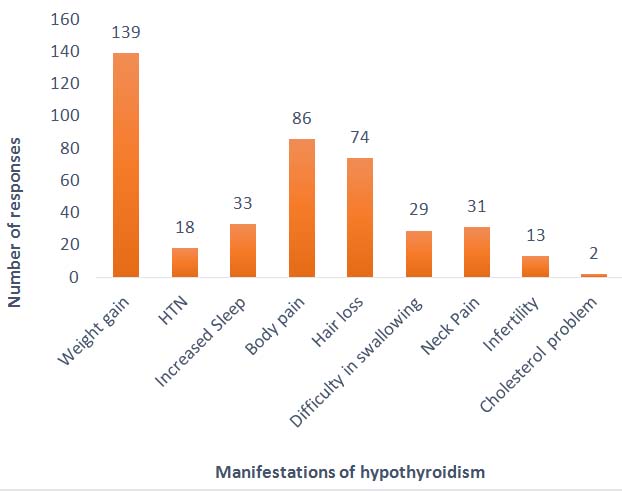
When assessed about who could likely to get hypothyroidism, 95 patients (38.9%) thought obese people are more likely to get it, followed by 67 patients (27.4%) who thought elderly are more affected and 32 patients (13.11%) believed women get more affected with hypothyroidism. a total of 28 patients (11.4%) believed those with a previous family history of hypothyroidism are more affected, whereas only 22 patients (9.0%) were aware hypothyroidism could affect all age groups. The responses of the patients, when enquired about the effects of hypothyroidism on general health, are given in.
When assessed about the cause of hypothyroidism, 100 patients (40.98%) felt it was due to obesity, 94 patients (38.5%) attributed it to certain foods, 34 patients (13.9%) felt it is caused due to stress, wherein 10 patients (4.0%) thought it is a communicable disorder and six patients (2.45%) were unaware of the cause for the hypothyroidism [Table/Fig-1].
Patient perceptions of different manifestations of hypothyroidism. HTN-Hypertension
The details of some of the other aspects of knowledge and misbeliefs in participants with regard to hypothyroidism are given in [Table/Fig-2].
Assessment of knowledge and beliefs about hypothyroidism.
| Questions | BelieversN (%) | Non-believersN (%) | Not sureN (%) |
|---|
| Is hypothyroidism preventable? | 88 (36.0) | 146 (59.9) | 10 (4.1) |
| Is hypothyroidism curable? | 75 (30.7) | 152 (62.2) | 17 (6.9) |
| Can hypothyroidism affect your spouse / in-laws? | 25 (10.2) | 210 (86.0) | 9 (3.6) |
| Can hypothyroidism affect your children / blood relatives? | 103 (42.2) | 135 (55.3) | 6 (2.4) |
| Should endocrinologists be consulted for thyroid problems? | 159 (65.1) | 25 (10.2) | 60 (24.5) |
| Can your thyroid problem be cured by intake of iodized salt? | 69 (28.2) | 173 (70) | 2 (0.8) |
| Should thyroid medication be stopped after reports normalise? | 41 (16) | 203 (83.3) | 0 (0) |
On the assessment of knowledge on levothyroxine use, 99 patients (40.5%) believed that levothyroxine (LT4) should be taken life-long and 76 patients (31.1%) felt LT4 should be taken till further instructions from the doctor. A total of 41 patients (16.8%) felt that it could be discontinued once reports normalized. A total of 16 patients (6.55%) felt it should be continued till the symptoms subside and 12 patients (4.91%) thought it should be taken till their neck swelling subsides.
The practice patterns of hypothyroid patients with respect to levothyroxine usage and follow up visits are listed in [Table/Fig-3]. Only one-third of the patients gave a gap of one hour between levothyroxine and food intake. Only 99 patients (40.5%) performed periodic thyroid function tests. About 40.9% patients had missed their tablets at least once a week, whereas 36.88% of the patients were taking calcium/iron medications along with levothyroxine.
Practice patterns followed by hypothyroid patients.
| Questions | Responses, n (%) |
|---|
| What time of day you take your thyroid tablets? | Early morning – 200(81.9)Afternoon – 14(5.73)Night – 30(12.2) |
| Do you take your thyroid tablets before food? | Yes – 212(86.8)No – 32(13.1) |
| Time gap followed between levothyroxine and food intake (n=212) | 10 min – 64(30.1)20 min – 30(14.1)30 min - 22(10.3)40 min - 15(7.07)60 min - 81(38.2) |
| How frequently do you miss your thyroid tablet? | Once a week – 100(40.9)Twice a week – 22(9.01)Thrice or more – 28(11.4)Once / twice a month – 33(13.5)Never – 61(25) |
| How frequently do you visit your thyroid physician? | Once a month - 68(27.8)Once in 3-6 months - 95(38.9)Once in a year - 81(33.1) |
| How frequently have you stopped your medications in the last one year thinking you were normal? | Once – 28(11.4)Twice – 35(14.3)Thrice – 28(11.4)No – 153(62.7) |
| How often do you get your thyroid tested? | Every 3 months – 30(12.2)Every 6 months – 50(20.4)Every 9 months – 14(5.73)Every 12 months - 20(8.19)When doctor advises – 130(53.2) |
| Do you avoid cabbage or cauliflower in your diet? | Yes – 100(40.9)No - 136(55.7)Not sure - 8(3.3) |
| Do you feel thyroid medications are helping you in reducing your complaints? | Very much - 72(29.5)To some extent – 110(45)Not always - 45(28)Never - 17(6.96) |
| Have you taken alternative medications for hypothyroidism? | Ayurveda - 45(18.4)Siddha - 0(0)Yunani - 0(0)Homeopathy - 69(28.2)No - 130(53.2) |
| Do you take calcium / vitamin D / iron tablets along with thyroid medications? | Yes – 90(36.88)No – 154(63.11) |
| Has your doctor prescribed calcium or vitamin D along with thyroxine? | Yes - 80(32.7)No - 164(67.2) |
| Are you taking calcium / vitamin D as recommended by the doctor? (n=80) | Yes - 68(85.0)No - 12(15) |
Discussion
The findings of our study suggest that Indian patients with hypothyroidism have limited knowledge with regard to many aspects of the condition. Furthermore, there are inadequacies with regard to the standard practices of hypothyroidism and its long-term follow up.
Nearly one-third of the patients did not know that thyroid is a gland; rather many misunderstood thyroid as a swelling in the neck. The results of our study are similar to that reported by Rai S et al., in which nearly one-third of the patients could not identify ‘thyroid’ as a gland [4]. In contrast, in a study done in Chennai, India, involving educated urban population, 79.41% had appropriately identified the term ‘thyroid’ as a gland [3]. This disparity could possibly be attributed to the differences in representation of participants from varying educational status between the different studies. Only 40.98% of the patients correctly identified the term ’hypothyroidism’ as decreased function of the thyroid gland. In other studies, the reported proportion of patients who could identify hypothyroidism as decreased function of the thyroid ranged from 49.2% to 55.88% [3-5,8].
It is often seen that patients commonly attribute many vague symptoms to hypothyroidism, especially those related to the neck such as sore throat and dysphagia. We tested the knowledge of our participants regarding some of the more established hypothyroid symptoms. In the present study, 56.9% felt that hypothyroidism is associated with weight gain. This was similar to previous studies, wherein 54.4%-70.5% of patients believed hypothyroidism causes weight gain [3-5]. Although it is well known that hypothyroidism can cause weight gain, it is seldom more than 2-4 kg [8]. This false attribution of excessive weight gain to hypothyroidism leads to the patient expecting unrealistic results from levothyroxine therapy. Hence, the patients should be counselled about proper diet and exercise for achieving weight loss and should be further stressed upon that weight gain may not be related to hypothyroidism.
In the present study, 40.98% patients believed that goitrogens need to be avoided in the diet. Most of the information seemed to be emanating from television and newspapers. No study has however evaluated in detail the effect of goitrogens on the course of hypothyroidism [9,10]. In the present study, 28.2% believed iodized salt could be used to treat hypothyroidism, while 46.7% of patients believed that alternative forms of medicine can cure hypothyroidism. These findings are in concordance with a previous study done by Singh A et al., [5].
A significant proportion of patients in our study believed that hypothyroidism can be cured with medications and that levothyroxine could be stopped when their thyroid function tests report normalized. Most of the patients in our study took levothyroxine early morning in the fasting state; however, only a third of the patients gave adequate gap between taking the tablet and having food or beverages [11-13]. Nearly two-thirds of the patients missed their medications at least once a week. When it came to follow up evaluation, only 40% of the patients came for regular follow up. Thyroid function tests were done only when their doctor had advised in majority of the patients.
Many factors could contribute to these gaps in the knowledge, awareness and practices noted amongst the hypothyroid patients. The most important factor could be the lack of expertise among treating physicians with regard to hypothyroidism [14]. This fact was observed in a study done at Tanzania, which had shown an insufficient knowledge among clinicians about thyroid disorders[15]. Another factor that needs to be addressed is inadequate time spent by the doctor on patient education. A previous study has also shown that intervention by a pharmacist could play an important role in addressing the lacunae about medication use [16]. Overall, it is noteworthy that allied medical services, staff nurses and medical educators play an important role along with the doctor in filling the gaps of knowledge and practices [17].
Patient driven factors like poor educational status, sociocultural beliefs and parental advice may be some of the other contributory factors [18]. Even among the educated folks, knowledge and awareness regarding hypothyroidism was found to be suboptimal and this could be due to inaccurate information obtained from the internet and electronic media [19].
There is a need for structured educational programmes to improve the understanding and awareness of hypothyroidism among general population [20]. It is surprising that while there are various media programmes for diabetes care, there are not enough educational activities for thyroid disorders. However, in a study by Crilly M et al., an educational booklet intervention in primary hypothyroid patients did not make a significant difference in the adherence to treatment or well-being [21]. It is thus imperative that the physician spends some time with the patients to educate them about proper practices.
Limitation
Our study might have been limited by its cross-sectional study design. Our study being conducted at a single centre makes the results to be less generalizable. Hence, we recommend multicentric studies to assess the effect of various demographic patterns and sociocultural differences on Knowledge, Attitude and Practice (KAP) in patients with hypothyroidism.
Conclusion
Our study highlights the high prevalence of inadequate knowledge, various misconceptions and faulty practices among hypothyroid patients. These factors may contribute to poor adherence to treatment and suboptimal patient outcomes.
Our study also emphasizes the importance of spending adequate time for comprehensive education of the patients in order to bridge the gaps in patient care. The results also suggest that healthcare providers could provide the patients with information sheets (attached as a supplementary in this article) explaining about the disease or to have a few pictorial/pamphlets about the truth and myths of the disease. These measures can advance their understanding of disease state, leading to value-added approach and superior outcomes.