Evaluation of the Relationship between Serum 25-Hydroxy Vitamin D and Hypertension in Hamadan, Iran-A Case Control Study
Behshad Naghshtabrizi1, Shiva Borzouei2, Pedram Bigvand3, Mohamad ali Seifrabiei4
1 Associate Professor, Department of Cardiology, Hamadan Medical School, Hamadan University of Medical Sciences, Hamadan, Iran.
2 Assistant Professor, Department of Internal Medicine, Hamadan Medical School, Hamadan University of Medical Sciences, Hamadan, Iran.
3 Junior Resident, Department of Internal Medicine, Babol Medical School, Babol University of Medical Sciences, Babol, Mazandaran, Iran.
4 Associate Professor, Department of Community Medicine, Hamadan Medical School, Hamadan University of Medical Sciences, Hamadan, Iran.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Mohamad Ali Seifrabiei, Associate Professor, Department of Community Medicine, Hamadan Medical School, Hamadan University of Medical Sciences, Hamadan-6517838736, Iran.
Introduction
Hypertension or high blood pressure is one of the main reasons of fatality in the world. The role of vitamin D in developing hypertension has not been proved yet. Some studies have shown positive correlation between low serum vitamin D level and hypertension. Due to this fact, recognising hypertension risk factors such as potential impact of low serum vitamin D level seems to be required.
Aim
This study was conducted to evaluate potential impact of serum vitamin D level on hypertension.
Materials and Methods
This case-control study had 188 subjects including 55 cases suffering from hypertension and 133 controls with normal blood pressure in Hamadan, Iran. After taking the medical history and physical examination, 5 cc of their blood was taken to measure their serum 25-Hydroxyvitamin D [25(OH)D] level through ELISA test. Data analysis was done by version 16.0 of SPSS software and used independent sample t-test and Chi-square test for related comparisons.
Results
Mean and standard deviation of serum 25(OH)D level in patients suffering from hypertension was 13.10±9.7 ng/ml and in control group was 20.87±10.34 ng/ml. This variance was statistically significant (p<0.001). Mean serum 25(OH)D level in both case and control groups was measured after gender and age stratification. Mean serum 25(OH)D level in cases and controls was 13.12±11.4 ng/ml and 21.38±11.47 ng/ml in males (p=0.016) and 13.10±9.91 ng/ml and 19.19±10.55 ng/ml (p=0.004) in females, respectively. Mean serum 25(OH)D level in under 50-year-old was 10.82±8.73 ng/ml and 20.07±11.17 ng/ml in cases and controls respectively (p<0.001). In over 50-year-old, there was no significant relationship between mean serum 25(OH)D and blood pressure levels (p>0.05).
Conclusion
According to this study, reverse relationship between serum 25(OH)D and blood pressure levels was seen.
High blood pressure, Risk factor, Vitamin deficiency
Introduction
According to statistics, one third of the US adult population (75 million people) and one billion people all over the world are suffering from hypertension [1]. According to a systematic review, hypertension prevalence is estimated to be about 23% and 50% in 30–55-year-old and over 55-year-old Iranians, respectively [2]. Hypertension or high blood pressure is considered as the main reason of fatality in the world, the most common reason of visiting physicians, and the simplest treatable and recognisable risk factor for diseases such as Cerebrovascular Accident (CVA), Myocardial Infarction (MI), Congestive Heart Failure (CHF), Peripheral Arterial Disease (PAD), Atrial Fibrillation (AF), and End Stage Renal Disease (ESRD) [1,3,4]. Despite reliable documents demonstrating the fact that medical therapy of hypertension will dramatically decrease the fatality, hypertension remains poorly controlled and is becoming more prevalent in both developed and developing countries [5,6]. Therefore, hypertension is considered as one of the main public health issues [1].
Hypertension affects more than 40% of US African-Americans; however, only 25% of white Americans have such a problem. African-Americans develop more severe and earlier hypertension, therefore, target organs involvement, and consequently premature disability and death is higher among them [3,7,8]. Vitamin D deficiency is associated with cardiovascular diseases such as Coronary Artery Disease (CAD), heart failure and hypertension [9].
It can be concluded that lower ultraviolet absorption and the consequent decline of skin’s ability in vitamin D synthesis is related to blood pressure changes. The mechanism by which vitamin D may regulate blood pressure is not firmly established. Initial studies by Li Y et al., and Li YC et al., suggested that vitamin D is a negative regulator of renin [10,11]. Some studies show that there is an association between vitamin D deficiency with augmented Renin –Angiotensin–Aldosterone System (RAAS) activity in humans, so there is an inverse correlation between Plasma Renin Activity (PRA) and 1,25(OH)2D [12,13], also the effect of improving endothelial function and the prevention of secondary hyperparathyroidism is being considered [14].
This case-control study was designed to show the relation of serum vitamin D level and hypertension in Hamadan, Iran.
Materials and Methods
This case-control study has been performed on 55 admitted patients suffering from hypertension as first presented to cardiovascular clinic of Ekbatan Hospital, Hamadan from January 2015 to January 2016. Sample size was calculated based on mean and standard deviation of vitamin D in hypertensive and normotensive groups according to previous study [15]. We considered 133 normotensive participants as control group (about 2-3 controls for each case) due to high prevalence of vitamin D deficiency in normal Iranian general population to improve our study power. Inclusion criteria for cases were people older than 18 years ranging from 25 to 89 years who were not under treatment for vitamin D deficiency and who were taking calcium supplements. People with diseases and medications which affect vitamin D and calcium absorption, pregnant women and secondary hypertensives were excluded from this study. Control group included 133 volunteers without hypertension or any other disease that affect vitamin D absorption and metabolism. Both groups were approximately alike in terms of age, gender, season referred, socioeconomic status (family income per month) and body mass amount.
In order to rule out secondary hypertension effects, medical history was taken and physical examination was done. Based on clinical suspicion, para clinical tests including complete blood count, erythrocyte sedimentation rate, serum electrolytes, serum calcium, lipid profiles, serum blood sugar, serum thyroid stimulation hormone and urinalysis were done and secondary hypertension was ruled out. After explaining the study and getting written consent, patients’ blood pressure was measured by Richter digital sphygmomanometer (German) considering standards of blood pressure measurement [16]. High blood pressure was considered when systolic and diastolic blood pressure was greater than 140 and 90 mmHg in all ages respectively. Their weight was measured by Prelchin digital scale (Italian) with an accuracy of 0.1 kg (fasting status), and their height was measured based on standards by Stature meter 2M (Chinese). A 5 cc of their blood was drawn and its serum was separated. Serum vitamin D level was measured by Elisa method at a temperature of -20OC in the laboratory. One member of the team designed the questionnaire including personal information, blood pressure level, height, weight and the serum vitamin D level, which was completed for each patient. BMI calculated via weight (kilogram)/height (meter2) formula. The same was performed on control group. Eventually, the data was stratified and analysed by version 16.0 of SPSS software using independent sample t-test and Chi-square test for related comparisons.
Results
A total of 188 individuals were studied in this study in which 55 (29%) were hypertensive cases and 133 (71%) were in the control group. In total, 49 individuals (26%) were males and 139 (74 %) were females aging from 25 to 89 years. Mean and standard deviation of patients age (suffering from hypertension) was 50.20±10.86 years, and of the controls was 48.8±13.23 years which did not show any significant difference (p=0.23). Other baseline characteristics of the two groups are shown in [Table/Fig-1].
Baseline characteristics of the case and control groups.
| Group | Case (55) | Control (133) | p-value |
|---|
| Age (years) mean±SD | 50.2 ±10.86 | 48.8 ±13.23 | 0.23 |
| Gender |
| Males | 22 (40%) | 27 (20.3%) | 0.11 |
| Females | 33 (60%) | 106 (79.7%) |
| Season referred |
| Spring and summer | 35 (63.6%) | 92 (69.17%) | 0.15 |
| Autumn and winter | 20 (36.4%) | 41 (30.83) |
| Socioeconomic status |
| Mean family income | 489 (Dollar/month) | 512 (Dollar/month) | 0.18 |
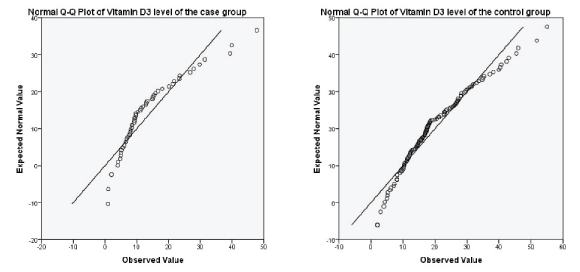
Vitamin D distribution was investigated through Q-Q Plot visual graph and Kolmogorov-Smirnov test in both the groups [Table/Fig-2]. Mean serum vitamin D level was measured in both case and control groups through t-test after making sure of its normality.
Testing for normality by using Q-Q Plot in case and control groups.
Cases (hypertensive group) had a lower serum vitamin D level. Mean and standard deviation of serum vitamin D level in cases was 13.10±9.7 ng/ml and in controls was 20.87±10.34 ng/ml. Mean difference of serum vitamin D in two groups with 95% confidence level was statistically significant (p<0.001) [Table/Fig-3].
Mean serum vitamin D level in hypertensive and control group.
| Group | Case | Control | p-value |
|---|
| Serum vitamin D (ng/ml) mean±SD | 13.10±9.7 | 20.87±10.34 | 0.000 |
After adjusting for gender, mean serum vitamin D in men was 13.12±11.14 ng/ml and 21.38±11.47 ng/ml in cases and controls, respectively. This variance among males was statistically significant (p=0.016). In women, mean serum vitamin D was 13.10±9.91 ng/ml in cases and 19.19±10.55 ng/ml in controls. This variance was statistically significant as well (p=0.004) [Table/Fig-4].
Serum vitamin D level according to gender.
| Gender | Group | Mean vitamin D serum level (ng/ml) | SD | p-value |
|---|
| Males (n=49) | Case (n=22) | 13.12 | 11.14 | 0.016 |
| Control (n=27) | 21.38 | 11.47 |
| Females (n=139) | Case (n=33) | 13.10 | 9.91 | 0.004 |
| Control (n=106) | 19.19 | 10.55 |
After age stratification, mean serum vitamin D level was 10.82±8.73 ng/ml in less than 50-year-old members of case group and 20.07±11.17 ng/ml in control group. This variance among less than 50-year-old people was statistically significant (p< 0.001). Mean serum vitamin D level in over 50-year-old people in case and control groups was 14.75±11.12 ng/ml and 17.21±7.64 ng/ml, respectively. This variance was not statistically significant (p=0.391) [Table/Fig-5].
Serum vitamin D level according to age.
| Age | Group | Mean vitamin D serum level (ng/ml) | SD | p-value |
|---|
| Under 50-year-old (n=136) | Case (n=23) | 10.82 | 8.73 | <0.001 |
| Control (n=113) | 20.07 | 11.17 |
| Over 50-year-old (n=52) | Case (n=32) | 14.75 | 11.12 | 0.391 |
| Control (n=20) | 17.21 | 7.64 |
Discussion
Our study showed significant difference between serum vitamin D level in hypertensive and normotensive participants.
Kota SK et al., showed systolic blood pressure, diastolic blood pressure and mean arterial blood pressure had increased among people with vitamin D deficiency and suggested that vitamin D deficiency is accompanied by Renin-Angiotensin-Aldosterone System activity (RAAS) [17].
Jorde R et al., showed that there is a relation between low serum vitamin D level and hypertension, although prescribing vitamin D could not prevent future hypertension [18]. Results of Jorde R et al., study, in terms of the relation between vitamin D deficiency and hypertension occurrence are the same as present study. According to Forman JP et al., serum 25(OH)D level has a reverse relation with hypertension development risk [15]. Caro Y et al., concluded that serum 25(OH)D level does not have any significant statistical relation with blood pressure [19].
It was demonstrated in a study done by Li L et al., that serum vitamin D and PTH levels have no significant relationship with blood pressure level or hypertension risk among Chinese people [20]. Kashi Z et al., showed no significant relationship between blood pressure, serum 25(OH)D, calcium and parathyroid hormone levels [21].
In our study, the variance of average level of serum 25(OH)D in the people suffering from hypertension and healthy people was significant (p<0.001); in other words, the average level of serum vitamin D level in healthy people was significantly more than people suffering from hypertension. Present study findings were in accordance with the results of Forman JP et al., Kota SK et al., and Jorde R et al., [15,17,18], however, our results had nothing in common with Caro Y et al., Li L et al., and Kashi Z et al., studies [19-21]. A significant relationship between 25(OH)D serum level and blood pressure in both males (p=0.016) and females (p=0.004) was found after gender stratification. Although when results were evaluated after age stratification, there existed a significant relationship between serum 25(OH)D and blood pressure levels in under 50 year-old group only (p<0.001). This relation was not significant in over 50-year-old group (p=0.391).
There is a controversy among the studies on the role of the serum vitamin D as a supplement to prevent or treat hypertension. It seems that vitamin D and blood pressure levels have inverse relationship. Unknown factors may play a role on relation between serum vitamin D and blood pressure levels especially in old ages.
Judd S et al., have reported a 9% decrease in mean systolic blood pressure in hypertensive patients who received calcitriol compared to placebo group [22]. As Snijder MB has reported in his study, vitamin D mechanism impact on blood pressure may be indirect based on its role in parathyroid hormone performance [16]. Further studies with more samples are required in which all possible factors are taken into account.
Limitation
This study has some limitation. An important limitation in this research was about sample size and disproportionate number of female and male participants in the study. Another limitation is regarding the use of convenient sampling method to collect data in cases and controls. Consequently, the sample may not be representative of the actual hypertensive and normotensive population.
Conclusion
Considering the significant difference in serum vitamin D level between hypertensive and normotensive participants, it is suggested that serum 25(OH)D is inversely associated with blood pressure, so recognising people with vitamin D deficiency is imperative.
[1]. Andreoli T, Benjamin I, Griggs R, Wing E, Carpenter AA, Cardiovascular diseaseCecil Essentials of Medicine 2010 8th ed:174 [Google Scholar]
[2]. Haghdoost AA, Sadeghirad B, Rezazadehkermani M, Epidemiology and heterogeneity of hypertension in Iran: a systematic reviewArchives of Iranian medicine 2008 11(4):444-52. [Google Scholar]
[3]. Victor RG, Douglas Mann, Douglas P. Zipes, Petter Libby, Robert O. Bonow, Systemic Hypertension: Mechanisms and DiagnosisBraunwald`s Heart Disease; a textbook of cardiovascular medicine 2015 10th edPhiladelphia, PAElsevier Sanders:934-951. [Google Scholar]
[4]. Delavari A, Horri N, Alikhani S, Mahdavi A, Hosseini SM, Haghighi S, Hypertension :epidemic, awareness, treatment, and control in over 20 year-old IraniansScientific journal of Iran Medical Council 2006 24(4):372-80. [Google Scholar]
[5]. James P, Oparil S, Carter B, Pharm D, Cushman W, Dennison C, Evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC8)JAMA 2013 311(5):14 [Google Scholar]
[6]. Weber M, Schiffrin E, White W, Mann S, Lindholm L, Kenerson J, Clinical practice guidelines for the management of hypertension in the community: A statement by the American Society of Hypertension and the International Society of HypertensionJ Clin Hypertens 2014 16(1):14-26. [Google Scholar]
[7]. Rostand SG, Vitamin D, blood pressure, and African Americans: toward a unifying hypothesisClinical journal of the American Society of Nephrology: CJASN 2010 5(9):1697-703. [Google Scholar]
[8]. Fiscella K, Winters P, Tancredi D, Franks P, Racial disparity in blood pressure: is vitamin D a factor?Journal of general internal medicine 2011 26(10):1105-11. [Google Scholar]
[9]. Yilmaz S, Sen F, Ozeke O, Temizhan A, Topaloglus S, Aras D, The relationship between vitamin D levels and non dipper hypertensionBlood pressure Monit 2015 20(6):330-34. [Google Scholar]
[10]. Li Y, Qiao G, Uskokovic M, Xiang W, Zheng W, Kong J, Vitamin D: a negative endocrine regulator of the renin-angiotensin system and blood pressureThe Journal of steroid biochemistry and molecular biology 2004 89-90:387-92. [Google Scholar]
[11]. Li YC, Kong J, Wei M, Chen ZF, Liu SQ, Cao LP, 1,25-Dihydroxyvitamin D(3) is a negative endocrine regulator of the renin-angiotensin systemThe Journal of clinical investigation 2002 110(2):229-38. [Google Scholar]
[12]. Resnick L, Muller F, Laragh J, Calcium regulating hormones in essential hypertension. Relation to plasma rennin activity and sodium metabolismAnn Intern Med 1986 105:649-54. [Google Scholar]
[13]. Vaidya A, Williams JS, The relationship between vitamin D and the renin-angiotensin system in the pathophysiology of hypertension, kidney disease, and diabetesMetabolism: clinical and experimental 2012 61(4):450-58. [Google Scholar]
[14]. Brewer L, Michos E, Reis J, Vitamin D in atherosclerosis, vascular disease and endothelial functionCurr Drug Targets 2011 12:54-60. [Google Scholar]
[15]. Forman JP, Giovannucci E, Holmes MD, Bischoff-Ferrari HA, Tworoger SS, Willett WC, Plasma 25-hydroxyvitamin D levels and risk of incident hypertensionHypertension (Dallas, Tex 1979) 2007 49(5):1063-69. [Google Scholar]
[16]. Snijder MB, Lips P, Seidell JC, Visser M, Deeg DJ, Dekker JM, Vitamin status and parathyroid hormone levels in relation to blood pressure: a population-based study in older men and womenJournal of internal medicine 2007 261(6):558-65. [Google Scholar]
[17]. Kota SK, Kota SK, Jammula S, Meher LK, Panda S, Tripathy PR, Renin-angiotensin system activity in vitamin D deficient, obese individuals with hypertension: An urban Indian studyIndian journal of endocrinology and metabolism 2011 15(Suppl 4):S395-401. [Google Scholar]
[18]. Jorde R, Figenschau Y, Emaus N, Hutchinson M, Grimnes G, Serum 25-hydroxyvitamin D levels are strongly related to systolic blood pressure but do not predict future hypertensionHypertension (Dallas, Tex 1979) 2010 55(3):792-98. [Google Scholar]
[19]. Caro Y, Negron V, Palacios C, Association between vitamin D levels and blood pressure in a group of Puerto RicansPuerto Rico health sciences journal 2012 31(3):123-29. [Google Scholar]
[20]. Li L, Yin X, Yao C, Zhu X, Wu X, Vitamin D, parathyroid hormone and their associations with hypertension in a Chinese populationPloS one 2012 7(8):e43344 [Google Scholar]
[21]. Kashi Z, Mirmiran P, Mehrabi Y, Hedayati M, Azizi F, Association of blood pressure, serum vitamin D, calcium and PTH in individuals over 40 in east Tehran 2003 :261-70. [Google Scholar]
[22]. Judd S, Raiser S, Kumari M, Tangpricha V, 1,25-dihydroxy vitamin D3 reduces systolic blood pressure in hypertensive adults: a pilot feasibility studyThe Journal of steroid biochemistry and molecular biology 2010 121(1-2):445-47. [Google Scholar]