Magnetic Resonance Imaging (MRI) is an imaging modality that has been developed and used since mid-1970s [1]. MRI has several advantages over computed tomography and ultrasonography.
One important feature is its non-invasiveness. A second feature that makes MRI particularly attractive is its capability for multiplanar imaging. A third advantage of MRI is its excellent tissue-differentiating capabilities. A fourth advantage of MRI is its intrinsic sensitivity to flowing blood. Both arterial and venous abnormalities can be assessed by MRI [1].
The indications for MRI for utero-ovarian lesions have expanded considerably over the past decade. The impetus behind these expanding indications is multifactorial. First, there has been widespread dissemination of MR hardware and software techniques that allow the routine acquisition of images with high spatial or temporal resolution. Second, the advent of minimally invasive therapies in the management of gynaecologic disorders has created a need for increased accuracy in the preoperative evaluation of these patients, Finally, in this era of cost containment, several studies have shown that the appropriate use of MR imaging in the diagnostic algorithm minimizes cost [2]. Some of the indications for MRI evaluation of the female genital tract are: infertility, congenital anomalies [3], ovarian and cervical lesions, pelvic inflammatory disease etc.
MRI of the adult female pelvis is a well-established tool in the evaluation of utero-ovarian lesions and is often used as a supplement to ultrasonography. The need for diagnostic surgical intervention has largely been eclipsed with the advent of MRI, which has become the imaging modality of choice for characterization of congenital Mullerian anomalies [4].
MRI is gaining momentum for staging gynaecologic malignancies. Ovarian cancer is the second most common pelvic tumour and the leading cause of death from gynaecologic malignancy. In patients with ovarian cancer, MRI determination of disease extent helps treatment planning either as a surgical roadmap or to identify non resectable patients. MRI staging is adjunct to clinical and surgical staging in women with cervical or endometrial cancer, respectively [5,6].
Therefore, an adnexal mass that appears suspicious at USG may be correctly diagnosed as a benign lesion at MR, preventing inappropriate radical surgery. MR is the most useful modality for evaluating adnexal lesions that are indeterminate at gray-scale ultrasound. Therefore, the study was carried out to assess the role of MRI in female pelvic mass lesion and to exploit the tissue characterization capability of MRI with few secondary aims like to study the spectrum of diverse nature of pelvic mass lesions, to determine the origin, tissue content and characterization of sonographically inconclusive uterine and adnexal masses, and to differentiate utero-ovarian lesions as neoplastic and non-neoplastic.
Materials and Methods
A prospective observational study was done in Department of Radiodiagnosis, Krishna Hospital, Karad, Maharashtra, India, for MRI pelvis with clinically suspected uterine and adnexal masses or with indeterminate diagnosis on ultrasonography. Over the study period of two years, from September 2014 to August 2016, 128 patients were referred for MRI pelvis, out of which 100 patients fulfilled our inclusion criteria and formed the sample size. Study was conducted after taking the institutional ethical clearance. Inclusion criteria were all patients with clinically suspected uterine and adnexal masses or with indeterminate diagnosis on sonography, non-pregnant females and patients of all age groups. Exclusion criteria were pregnant females, patients having any metallic implants, patients having history of claustrophobia, and all patients who do not consent to be a part of the study.
Ultrasonography pelvis and MRI pelvis of all the patients was done after obtaining the written informed consent in English as well as in regional language (Marathi) and imaging was done as per imaging protocol and images were stored in compact disc. All patients in our study underwent pelvic ultrasonography (SIEMENS ACUSON x300) by using both curvilinear (3-5 MHz) and linear (6-9 MHz) probes, with the patient in supine position. This is followed by pelvic MRI examination on a 1.5 Tesla scanner (SIEMENS TIM + DOT AVANTO). Scanning was performed after a fasting period of four to six hour prior to the examination to limit bowel motion. Imaging was in supine position with a Body matrix coil # Tim placed on the torso covering the entire imaging area. Initially a localizer scan was performed in transverse, sagittal and coronal orientation. This was followed by T1W/TSE {TE=10 ms / TR=500 ms} in sagittal planes; T2W/TSE {TE=80-90 ms / TR=4000-4200 ms} - axial, coronal and sagittal planes; STIR {TE=30-40 ms / TR=3500-4000 ms} -coronal planes, T1FS {TE=10 ms / TR=500 ms} – coronal and axial planes and T2FS {TE=80-90 ms / TR=4000-4200 ms} in axial and sagittal planes as required.
Gadolinium dimeglumine (Omniscan) 10 ml was administered as and when required. Nearly, 10 ml saline flush was also given after administration of gadodiamide. Post contrast T1FS {TE=10 ms/ TR=500 ms} images were obtained in axial, coronal and sagittal planes. Both gadolinium dimeglumine and normal saline were administered at the rate of 2 ml/sec. The parameters included matrix size of 192–256 × 256–512, field of view (appropriate to body habitus), 230–250 mm for the body coil, and 3-4 mm section thickness with an intersection gap of 30%-40%. Post processing was done by inbuilt software.
Both ultrasonography and MRI were performed by same group of researchers. In MRI size, shape, signal intensity, character, and postcontrast enhancement of the lesions were observed. After the MRI it was the decision of the referring physician to operate or not, and whenever the patients were operated biopsy was done. In our study, four patients were not operated.
Statistical Analysis
The statistical software namely MedCalc 9.0.1, Systat 12.0 were used for the analysis of the data and Microsoft word and Excel have been used to generate graphs, tables etc. Descriptive and inferential statistical analysis has been carried out in the present study. Results on continuous measurements are presented on Mean±SD (Min-Max) and results on categorical measurements are presented in Number (%).
Results
The maximum number of patients were in the age group 51-60 (23) followed by 31-40 (18) and 20-30 (16). The range was between 10 and 80 years.
The maximum cases in USG diagnosis group were those of bulky uterus (10) followed by fibroid uterus (8) and bulky cervix + uterus (8). Distribution of lesions on USG, MRI and histopathology are mentioned in [Table/Fig-1].
Distribution of lesions – on USG, MRI, histopathology.
| Lesion | USG | MRI | Histopathology |
|---|
| Uterine | 48 | 48 | 48 |
| Ovarian | 25 | 40 | 41 |
| Adnexal | - | 4 | 5 |
| Inconclusive | 27 | 6 | - |
| Normal Study/NA | - | 2 | 6 |
| Total | 100 | 100 | 100 |
The maximum cases in MRI diagnosis group were those of fibroid uterus (22=46% of the uterine lesions) followed by endometrial carcinoma (10=21% of the uterine lesions) and carcinoma cervix (10=21% of the uterine lesions) [Table/Fig-1].
The maximum number of patients with ovarian lesions were having serous cystadenoma (right) n-6 (19.36% of ovarian lesions) and serous cystadenoma (left) n-6 (19.36% of ovarian lesions) followed by mucinous cystadenoma (right) n-5 (16.13% of ovarian lesions), mucinous cystadenoma (bilateral) n-3 (9.68% of ovarian lesions).
Internal and external Characteristics of the lesions on MRI were described in the [Table/Fig-2,3,4,5,6 and 7].
Well-defined/ill-defined - distribution of lesions studied.
| Lesion | Well-Defined | Ill-Defined | Not Applicable |
|---|
| Uterine | 24 | 24 | 2 |
| Ovarian/Adnexal | 46 | 4 | 0 |
| Total | 70 | 28 | 2 |
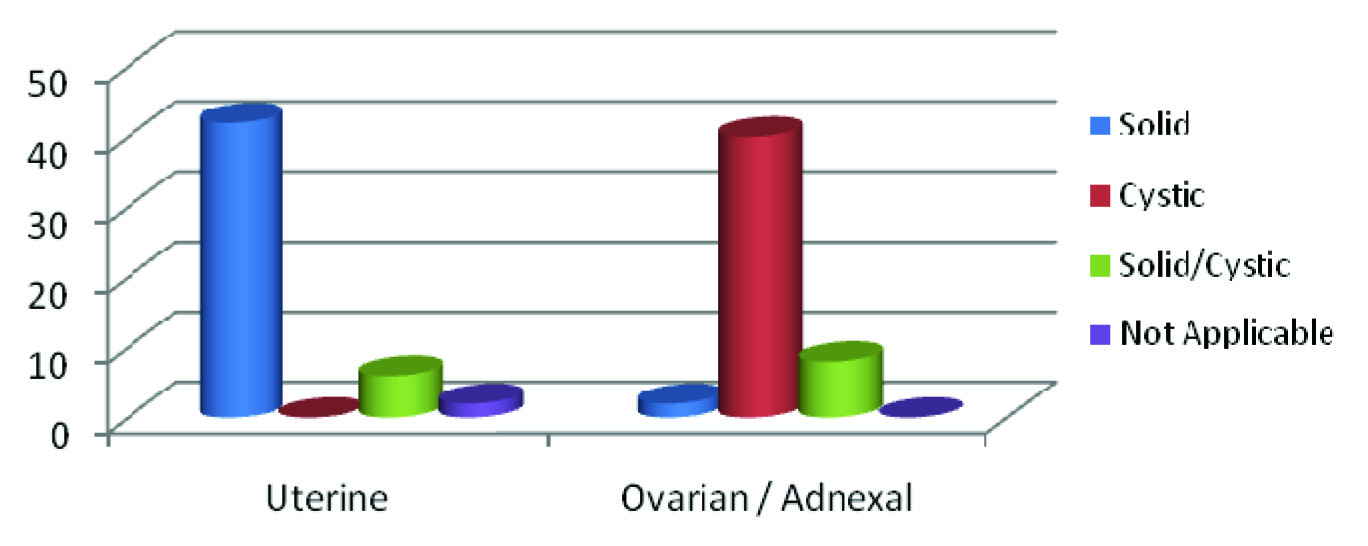
Solid/cystic - distribution of lesions studied.
Fat planes - distribution of lesions studied.
| Lesions | Preserved | Not Preserved | Not Applicable |
|---|
| Uterine | 44 | 4 | 2 |
| Ovarian/Adnexal | 48 | 2 | 0 |
| Total | 92 | 6 | 2 |
Mass effect - distribution of lesions studied.
| Mass Effect | Present | Absent | Not Applicable |
|---|
| Uterine | 5 | 43 | 2 |
| Ovarian/Adnexal | 20 | 30 | 0 |
| Total | 25 | 73 | 2 |
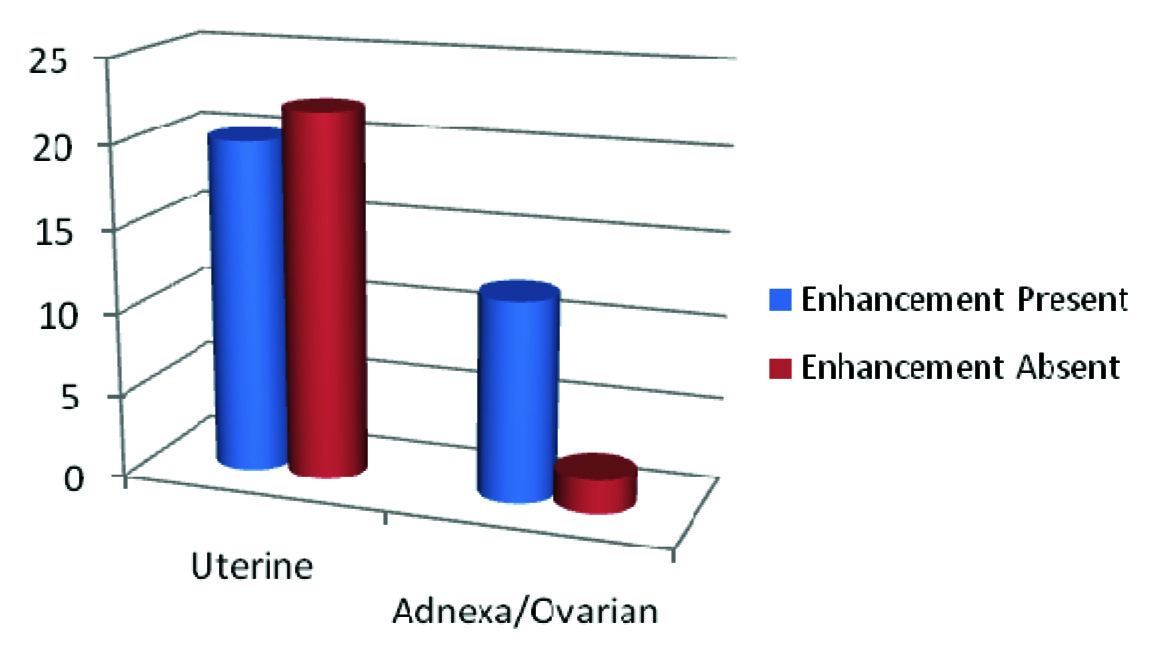
Gadolinium enhancement - distribution of lesions studied.
Internal characteristics of the ovarian/adnexal lesions.
| Characteristics | Epithelial cell tumours | Ovarian/adnexal lesions |
|---|
| SCA | MCA | MCAC | SCAC | RO/ACC | MO/AML | T-OCL | LOCC | DER MOID |
|---|
| Nodules | | 4 | 2 | | | | | | |
| Fat | | | | | 2 | | | | |
| Hemorrhage | | 2 | 2 | | | | 2 | 2 | |
| Calcifications | | | | | 2 | | | | 2 |
| Septations | 10 | 8 | 2 | 1 | 4 | 1 | 2 | | |
ISCA - Serous Cystadenoma; MCA - Mucinous Cystadenoma; SCAC - Serous Cystadenocarcinoma; MCAC - Mucinous Cystadenocarcinoma; RO/ACC - Right ovarian/adnexal cystic lesion; MO/A ML - Malignant ovarian/adnexal mass lesion; T-OCL - Tubo-ovarian cystic lesion; LOCC - Left ovarian complex cyst.
Neoplastic i.e., benign vs malignant and non-neoplastic distribution of lesions are mentioned in [Table/Fig-8,9].
Neoplastic/non-neoplastic - distribution of lesions studied.
| Lesions | Neoplastic | Non Neoplastic | Not Applicable |
|---|
| Uterine | 48 | 0 | 2 (Normal study) |
| Ovarian/Adnexal | 48 | 2 | 0 |
| Total | 96 | 2 | 2 |
Benign/Malignant - distribution of lesions studied by MRI study.
| Lesions | Benign | Malignant | Not Applicable |
|---|
| Uterine | 28 | 20 | 2 (Normal study) |
| Ovarian/Adnexal | 42 | 8 | 0 |
| Total | 70 | 28 | 2 |
Discussion
MRI is an excellent tool in the tissue characterization of female pelvic mass lesions, differentiating non-neoplastic lesions from neoplastic lesions and benign from malignant lesions, apart from determining origin of the lesion in case of indeterminate diagnosis on ultrasonography.
A] Uterine Lesions
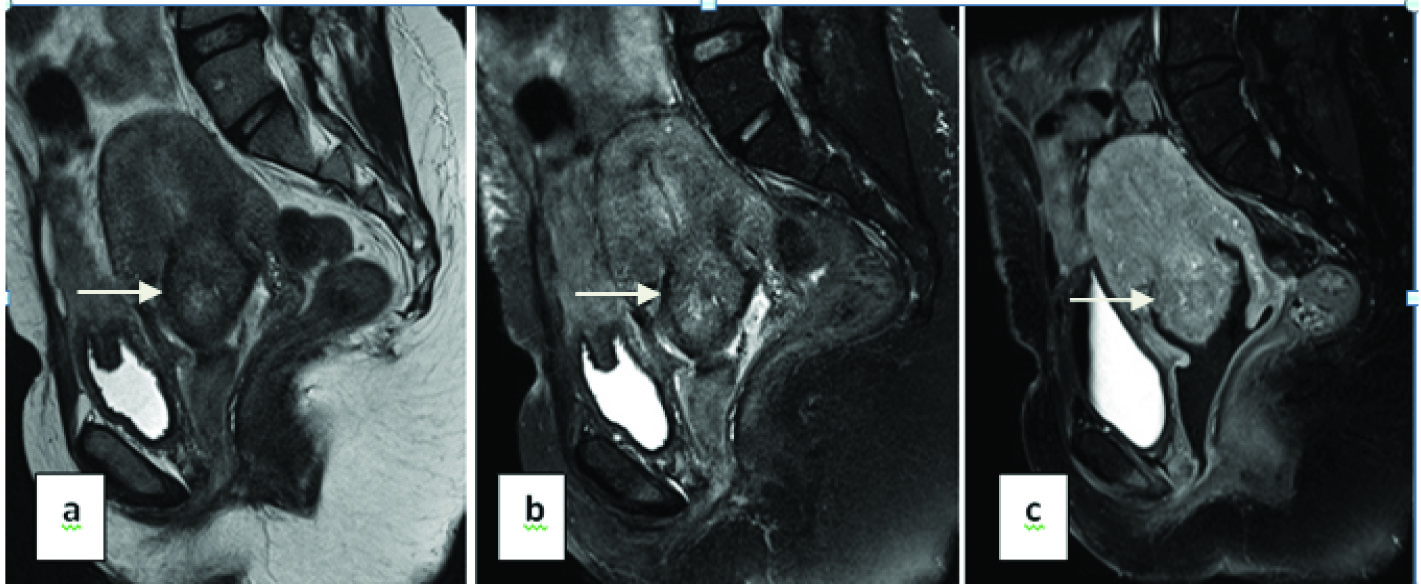
A1) Uterine fibroids [Table/Fig-10]: In the present study, among the uterine lesions uterine fibroids, only 16 (n=16→33%) were diagnosed with USG while 22 (n=22→46%) were diagnosed by MRI. This was similar to studies by Hamlin JD et al., where MR imaging to be more accurate than USG [7]. Two of the lesions were given a doubtful diagnosis of bulky cervix which was proved to be a uterine leiomyoma on HPE. In another two cases, which were diagnosed on USG as carcinoma endometrium turned out to be a uterine fibroid on MRI.
a) T2WI sagittal; b) T2FS sagittal; c) T1FS sagittal contrast images - showing altered signal intensities in posterior myometrium and displacing the endometrium anteriorly - Submucosal fibroid (arrows).
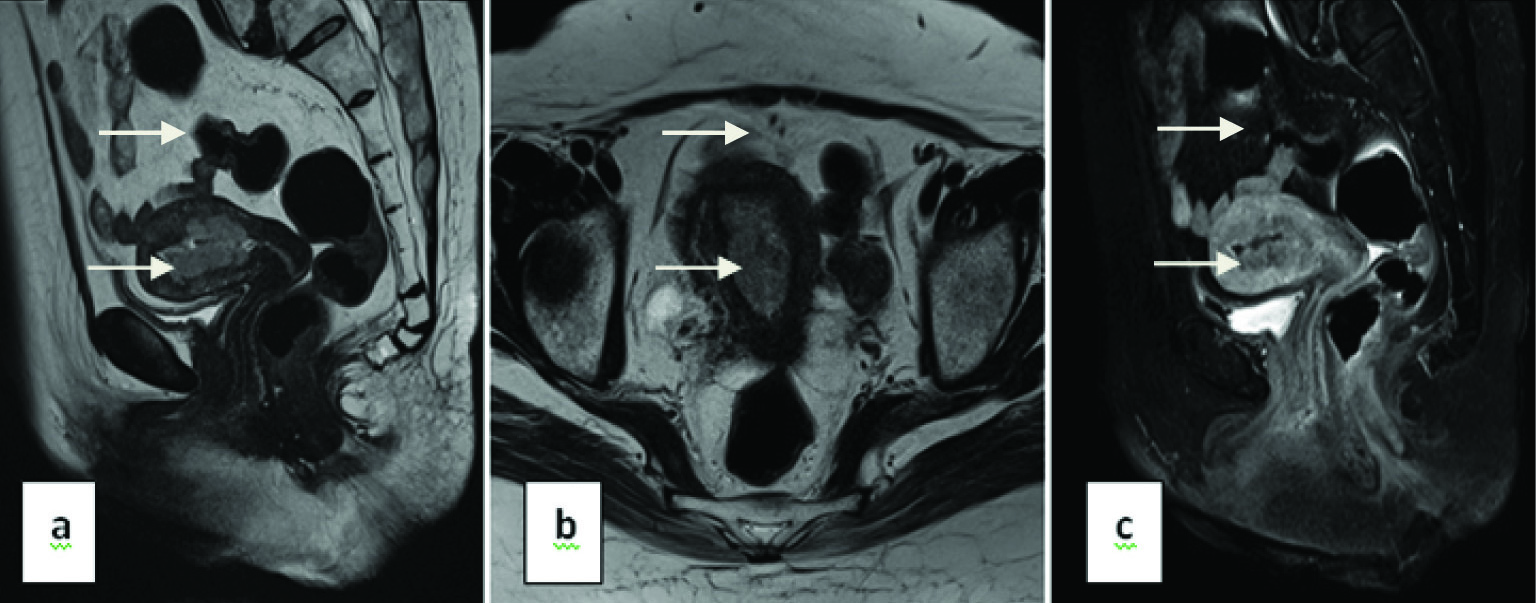
A2) Endometrial carcinoma [Table/Fig-11]: MRI could diagnose only 10 (n=10→21%) endometrial carcinomas of all uterine lesions. two of which turned to be uterine leiomyoma on HPE.
a) T2W sagittal; b) T2W Axial c) T1FS Sagittal contrast images - Well defined diffuse circumferential lesion causing thickening of the endometrium involving anterior and posterior endometrial wall showing heterogenous enhancement (less enhancement than normal myometrium) with interruption of junctional zone indicating myometrial invasion (>50%) – CA endometrium (arrows).
Patients typically present between the fifth and eighth decades of life, with a mean age of presentation was 64 years. The most common clinical manifestation was abnormal vaginal bleeding. The differential diagnosis for endometrial cancer includes cervical cancer, endometrial polyps, and mesenchymal tumours of the uterus. Distinguishing between these entities is easier in smaller tumours [8,9].
A3) Adenomyosis [Table/Fig-12]: There were four cases of adenomyosis (n=4→8%) of all uterine lesions. Two of the lesions appeared as ill-defined ovoid/diffuse region of thickening with small high T2 signal regions whereas the other lesions had a striated appearance. However, on HPE the lesion with striated appearance turned out to be normal proliferative endometrium.
a) T2W sagittal; b) T2W axial; c) Bulky uterus with thick endometrium with endometrial collection. Both anterior and posterior myometrium shows multiple tiny haphazardly distributed T2 hyperintense areas. Endo-myometrial borders are hazy – Adenomyosis (arrow).
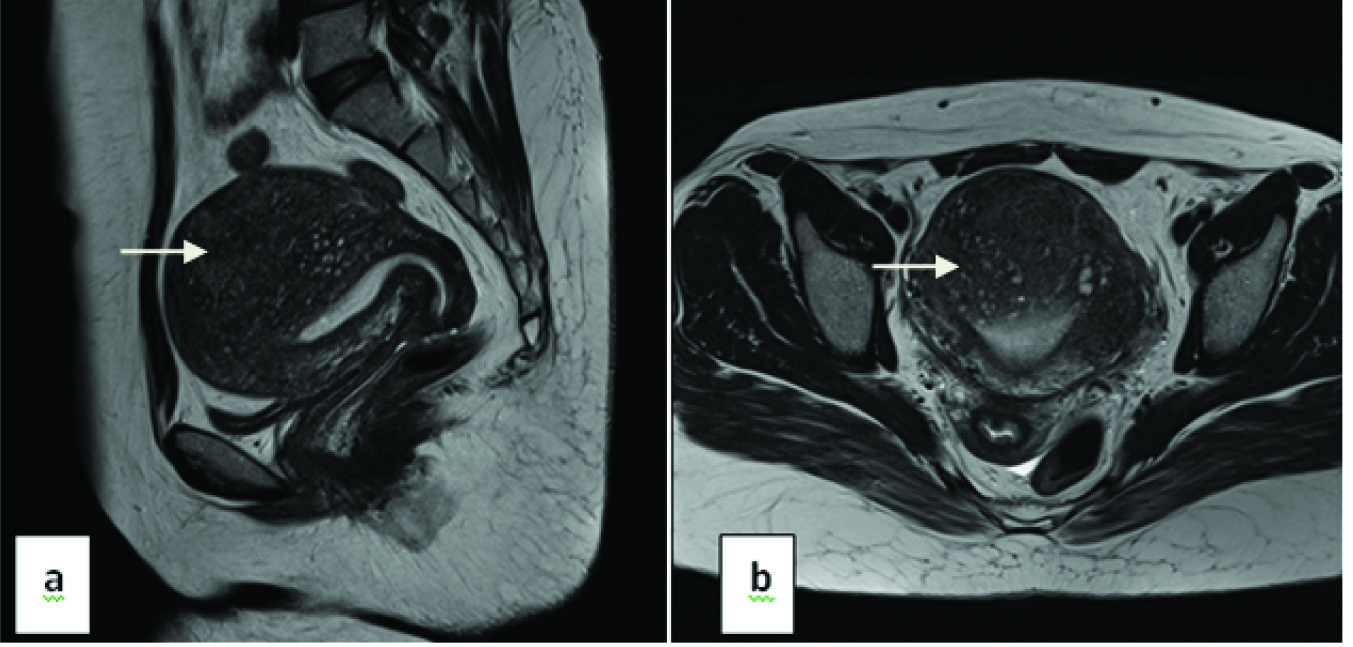
MR imaging is also an accurate, noninvasive modality for diagnosing adenomyosis with a high sensitivity (78%–88%) and specificity (67%–93%) – according to a study done by Reinhold C et al., [10].
A4) Carcinoma cervix: MR imaging could diagnose 10 (n=10→21%) cases of carcinoma cervix of all uterine lesions.
Patients typically present between the fouth and seventh decades of life, with a mean age at presentation of 56 years. The mean age was 53 years according to a study by Yamashita Y et al., [11]. Another study by Reinhold C et al., and McCarthy S et al., showed the mean age to be 45 years [12,13].
According to a study by Szklaruk J et al., where they had a maximum of squamous cell carcinomas – 90%, followed by adeno-squamous carcinoma [14]. Appearance and extension of each lesion vary according to the stage of the lesion, ranging from stage IB (six cases) to IIIA (one case).
B] Ovarian and Inconclusive Ovarian/Adnexal Lesions
Out of the 50 ovarian and adnexal lesions, origin of 27 (54%) lesions could not be made out by USG, whereas origin of only 6 (12%) lesions could not be made out and 44 (88%) lesions could be made out by MRI. Inconclusive lesions were later proved to be three ovarian and three adnexal in origin by HPE. According to a similar study done by Dwivedi AN et al., they showed that MRI was 97.7% sensitive and 73.1% specific for diagnosing mass of ovarian origin [15].
Out of the 50 ovarian and adnexal lesions, 23 lesions were right sided, 15 left sided, eight were bilateral. The laterality of 4 lesions could not be made out because of the large size of the tumours which were crossing the midline and as the ovaries could not be seen separately.
Out of the 50 ovarian and adnexal lesion 48 (96%) were neoplastic and 2 (4%) were non-neoplastic on MRI. Our findings were more or less similar to a study done by Sohaib SA et al., which shows 91%-93% overall accuracy for differentiating benign from malignant tumours [16].
B1) Epithelial tumours: There were 28 (58%) epithelial tumours of the 50 ovarian/adnexal lesions. There were 12 serous cystadenomas (six patients had right and six patients had left serous cystadenoma) [Table/Fig-13] which comprise 25% of the ovarian/adnexal neoplasm studied.
a) T2W sagittal; b) T2W axial; c) T1FS axial - A large well defined solid cystic lesion in pelvis with enhancing multiple septations (arrow) within it – Serous cystadenoma.
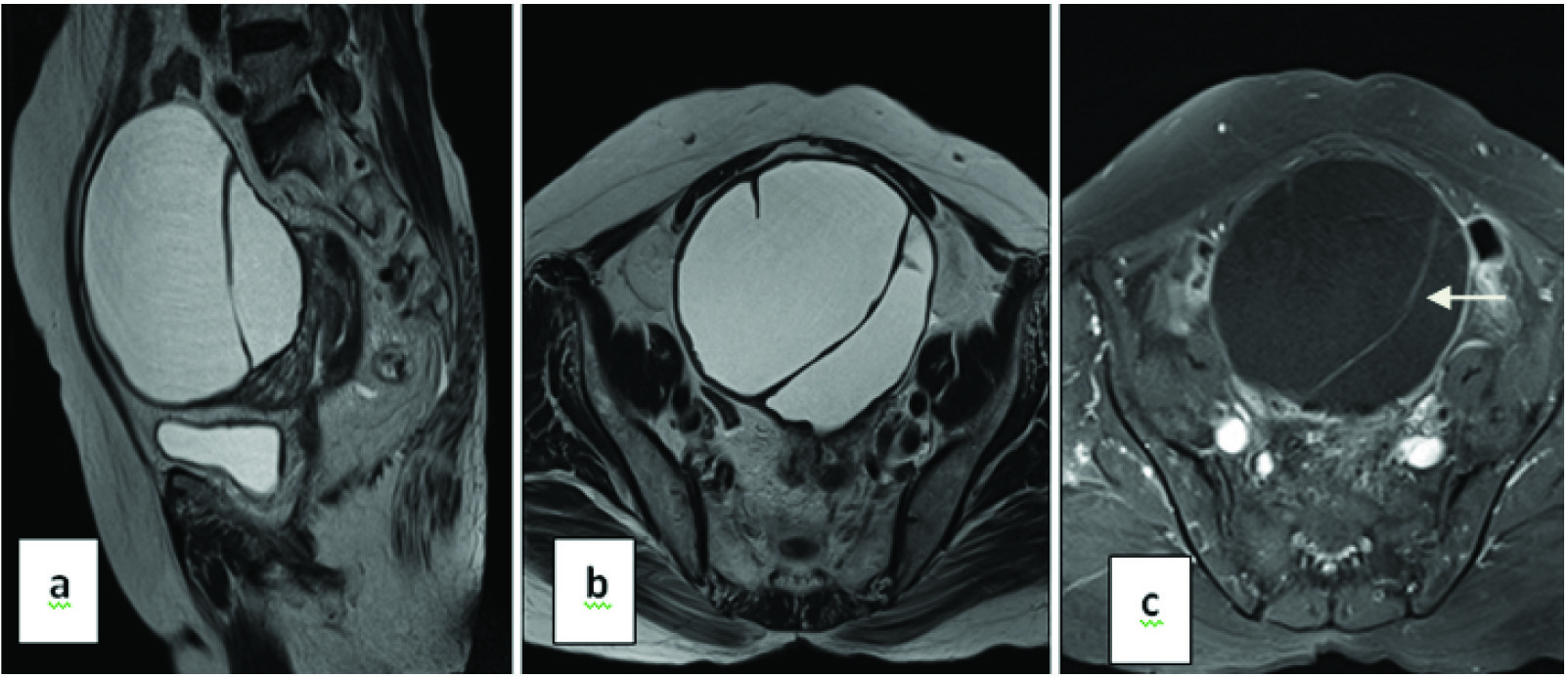
Serous cystadenomas comprise approximately 20% of the benign ovarian masses. They present as complex thin-walled, unilocular- or multilocular cysts, with variable sizes, sometimes achieving more than 20 cm. The image of its interior shows echogenic contents, possibly also revealing areas of papillary projections [17].
In our study there were 10 (21%) mucinous cystadenomas out of the 48 neoplastic ovarian lesions. This was similar to a study done by Seidman JD et al., mucinous ovarian tumours are less common than serous neoplasms. They represent 20% of all ovarian tumours and approximately 10% of all malignant ovarian tumours [18].
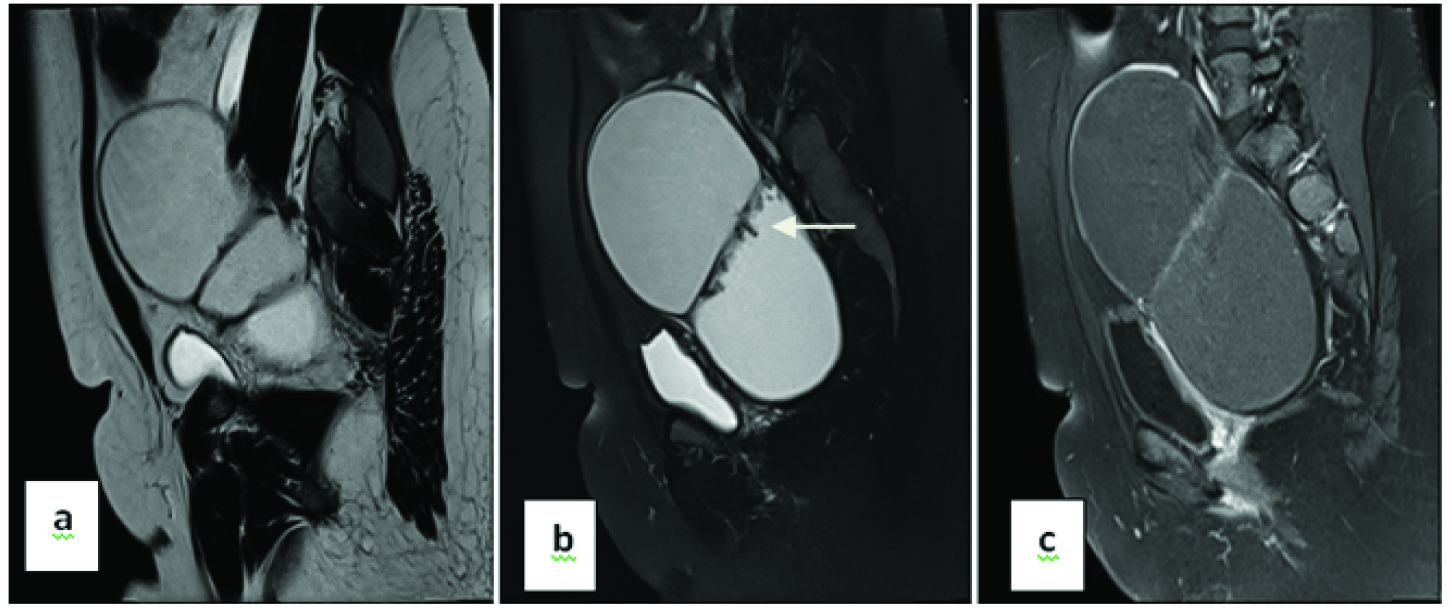
Two cases were mucinous cystadenocarcinoma [Table/Fig-14] which comprises 4% of the ovarian neoplasms in the present study.
a) T2W sagittal; b) T2FS sagittal; c) T1FS sagittal contrast images- Left adnexa shows large lobulated cystic lesion showing variable signal intensity and peripheral enhancement with papillary projections (arrow) and thick enhancing septations (~5 mm) - mucinous cyst adenocarcinoma.
B2) Germ cell tumours: We found two cases of dysgerminoma during the course of the study. The patients were 11 and 13-year-old. Most cases occur in adolescence and early adulthood, although it may occur at any age according to Shaaban AM et al., [19].
MR imaging revealed a solid mass divided into lobules by fibrovascular septa. The septae showed intense enhancement after administration of contrast material. This finding corroborates with Shaaban AM et al., who state that dysgerminomas have low signal intensity relative to muscle on T1- weighted images and are isointense or slightly hyperintense on T2-weighted images [19]. Usually, septa are hypointense isointense on T2-weighted images and are difficult to appreciate on T1-weighted images, with intense enhancement after administration of contrast material.
There were four patients who had dermoid. Two patients had bilateral dermoid. Caruso PA et al., found that 10% of dermoid were bilateral [20]. Three of the four dermoid were unilocular (75%) and it corroborates with Outwater EK et al., who states that 88% of benign cystic teratomas are unilocular [21].
At MR imaging, the sebaceous component of the dermoid cysts had very high signal intensity on T1-weighted images similar to that of retroperitoneal fat. The signal intensity of the sebaceous component on T2-weighted images was variable, usually near that of fat. There was complete drop in signal intensity on fat sat sequences. This correlates with study done by Guinet C and Kido A et al., [22,23].
Limitation
Potential problems in MRI detection of ovarian lesions include difficulty in determining the adnexa of origin of a large mass. The organ of origin is also difficult to determine in larger adnexal lesions. Secondly, the duration of the study was small so few cases of each tumour type could be collected. A longer duration study with larger number of cases would show a better picture. Thirdly, chances are that only ultrasonographically complex lesions were referred for MR examination which could also have introduced some sort of bias. It is also possible that cases with disseminated uterine and ovarian malignancy were not referred for MR evaluation.
Conclusion
In conclusion it can be said that due to excellent depiction of pelvic anatomy and absence of ionizing radiation, MRI is an excellent tool for the assessment of disorders of the uterus and ovary. MRI is a better modality for detecting, characterization of various diseases, staging patients with carcinomas where accurate diagnosis will make an impact on their surgical and medical management planning in comparison with USG.
ISCA - Serous Cystadenoma; MCA - Mucinous Cystadenoma; SCAC - Serous Cystadenocarcinoma; MCAC - Mucinous Cystadenocarcinoma; RO/ACC - Right ovarian/adnexal cystic lesion; MO/A ML - Malignant ovarian/adnexal mass lesion; T-OCL - Tubo-ovarian cystic lesion; LOCC - Left ovarian complex cyst.