A descriptive cross-sectional study was conducted among patients visiting Pacific Dental College and Hospital of Udaipur city, Rajasthan, India, during the month of July 2016. Ethical Committee of Pacific Dental College and Hospital granted the ethical clearance after reviewing the study protocol. An official permission was taken before conducting the study from the Principal of Pacific Dental College and Hospital. Following the investigators explanation on the purpose and details of the study, a written informed consent was obtained from all the participants. Patients attending Pacific Dental College and Hospital of Udaipur city available during the study period, patients who were consuming any form of tobacco, patients aged more than 18 years but less than 50 years, past tobacco users who continued their habit at least for one year were included in the study. While those patients who do not consume tobacco, who were not willing to participate, who were not brought up by their parents/orphans, were excluded from the study.
A structured questionnaire was developed and tested among a convenience sample of 20 patients, for overall acceptability of the language and length of the questionnaire. The parental bonding measure questionnaire was converted in local language (Hindi) for better understanding by the patient. For test-retest purposes 50 of the follow-up participants completed the questionnaire two weeks later. Test-retest reliability was found significant. Cronbach’s coefficient was found to be 0.80, which showed an internal reliability of the questionnaire. Content Validity Ratio (CVR) was figured as 0.87 in light of the conclusions communicated by a board of five academicians. Face validity was additionally surveyed and it was found that 92% of the participants observed the questionnaire to be simple.
Pilot study was conducted among 20 subjects before the main study to check the feasibility and validity of the study. Pilot study assessments were utilized for proper planning and execution of the main study and also to finalize the procedure, method and analysis of the samples.
Based on the results of pilot study, a total sample size attained was 130 using hypothesis testing (proportion) formula.
Section IV consisted of participant’s perception of their mother’s and father’s parenting behaviour using a modified version of the parental bonding instrument [10], adapted from the Whitehall study II, 1985 [11]. The questionnaire was converted to Hindi language for better understanding of the patient. Three latent constructs of subject‘s perception of parenting behaviours were identified for each parent, resulting in six variables: maternal warmth, maternal strictness, paternal warmth, paternal strictness, maternal expectation and paternal expectation. Four questions regarding understanding, loving, affectionate and trustworthy behaviour of the parent loaded on the warmth factor, and two questions regarding punishment and rules loaded on the strictness factor and one question regarding the expectation of parents to achievements of children. For good interpretability of the scores, the questions were consolidated on the basis of their factor loadings. Parental warmth was considered factor 1, parental strictness as factor 2 and parental expectation as factor 3 and factors with an Eigenvalue > 1 were considered.
Materials and Methods
The investigator distributed the questionnaire in the patient waiting area of the hospital. The purpose of the study was informed and explained to the participant. Those willing to participate in the survey were requested to fill in the written informed consent form. After obtaining written informed consent, the investigator collected information by questionnaire based interview. The investigator collected the detailed information on participants and parental tobacco usage habits. After collecting the required information, participants were given the questionnaire and were asked to rate each item of the parental bonding measures choosing the most appropriate response. They were guided that if they do not understand any item on the questionnaire, they can freely ask the investigator who was present during the complete course of time. Sufficient time was given to them to fill the questionnaire. The questionnaires were then gathered and checked for their completeness.
Statistical Analysis
Completed questionnaires were coded and spreadsheets were created for data entry. The data were analysed using Statistical Package for Social Sciences (SPSS) software program (version 22.0). Responses to all items of the Sections II and III were recorded as 1, 2 (ever users, never users). Participants who had the habit of tobacco chewing for at least one year or more than one year at any point in their life were considered as ‘ever users’ of tobacco consumption and participants who had chewed tobacco for less than one year in their lifetime were considered as ‘never users’. Descriptive statistics were used to summarize the demographic information and the survey data was analysed using the Chi-square test. Multiple logistic regression analysis was carried out to check association between parental and participant’s tobacco usage. Confidence level and level of significance were fixed at 95% and 5% respectively.
Results
[Table/Fig-1]: A total of 130 adults participated in the study with an age range of 18-50 years (mean±SD; 30.4±8.5). Majority of the participants were males 97 (74.6%), Hindus 115 (88.5%), married 97 (74.6%) and were from upper socioeconomic status 59 (45.4%). Parental education status revealed that majority of mothers were illiterate 61 (46.9%) and fathers were educated till secondary level 35 (26.9%).
Demographic characteristics of study participants and their parents.
| Variable | N | % |
|---|
| Age (Years) |
| 18-27 | 47 | 36.2 |
| 28-38 | 59 | 45.4 |
| 39-49 | 24 | 18.5 |
| Gender |
| Male | 97 | 74.6 |
| Female | 33 | 25.4 |
| Education |
| Primary | 19 | 14.6 |
| Secondary | 47 | 36.2 |
| Higher secondary | 25 | 19.2 |
| Graduate | 28 | 21.5 |
| Postgraduate | 4 | 3.1 |
| Illiterate | 7 | 5.4 |
| Socioeconomic status |
| Upper | 59 | 45.4 |
| Upper middle | 28 | 21.5 |
| Middle | 26 | 20 |
| Lower middle | 11 | 8.5 |
| Lower | 6 | 4.6 |
| Marital status |
| Married | 97 | 74.6 |
| Unmarried | 33 | 25.4 |
| Religion |
| Hindu | 115 | 88.5 |
| Muslim | 15 | 11.5 |
| Maternal education |
| Primary | 17 | 13.1 |
| Secondary | 32 | 24.6 |
| Higher Secondary | 12 | 9.2 |
| Graduate | 8 | 6.2 |
| Postgraduate | 0 | 0 |
| Illiterate | 61 | 46.9 |
| Paternal education |
| Primary | 13 | 10 |
| Secondary | 35 | 26.9 |
| Higher secondary | 33 | 25.4 |
| Graduate | 21 | 16.2 |
| Postgraduate | 2 | 1.5 |
| Illiterate | 26 | 20 |
| Total | 130 | 100 |
[Table/Fig-2]: depicts participants and parental tobacco usage habits. Most of the participants were consuming tobacco in the smoking form. Parental smoking and smokeless tobacco usage was more prevalent in case of paternal side i.e., 89 (68.5%) and 62 (47.7%) respectively.
Tobacco usage habits among study participant’s and their parents.
| Tobacco Use | N | % |
|---|
| Participant’s smoking tobacco |
| Ever | 91 | 70 |
| Never | 39 | 30 |
| Participant’s smokeless tobacco |
| Ever | 76 | 58.5 |
| Never | 54 | 41.5 |
| Paternal smoking |
| Ever | 89 | 68.5 |
| Never | 41 | 31.5 |
| Maternal smoking |
| Ever | 12 | 9.2 |
| Never | 118 | 90.8 |
| Paternal tobacco chewing |
| Ever | 62 | 47.7 |
| Never | 68 | 52.3 |
| Maternal tobacco chewing |
| Ever | 21 | 16.2 |
| Never | 109 | 83.8 |
[Table/Fig-3]: shows the association of demographic variables with participants tobacco use. A statistically significant association was found between gender, education and socioeconomic status and participant’s tobacco use (p≤0.05).
Association of demographic variables with study participant’s tobacco use.
| Variables | Total N | Smoking Tobacco Use | Smokeless Tobacco Use |
|---|
| Ever n (%) | Never N (%) | Ever N (%) | Never N (%) |
|---|
| Age |
| 18-27 | 47 | 29 (61.7) | 18 (38.3) | 29 (61.7) | 18 (38.3) |
| 28-38 | 59 | 46 (78) | 13 (22) | 34 (57.6) | 25 (42.4) |
| 39-49 | 24 | 16 (66.7) | 8 (33.3) | 13 (54.2) | 11 (45.8) |
| p-value | 0.178 | 0.818 |
| Gender |
| Male | 97 | 75 (77.3) | 22 (22.7) | 49 (50.5) | 48 (49.5) |
| Female | 33 | 16 (48.5) | 17 (51.5) | 27 (81.8) | 6 (18.2) |
| p-value | 0.002* | 0.002* |
| Education |
| Primary | 19 | 5 (26.3) | 14 (73.7) | 19 (100) | 0 |
| Secondary | 47 | 33 (70.2) | 14 (29.8) | 31 (66) | 16 (34) |
| Higher Secondary | 25 | 18 (72) | 7 (28) | 13 (52) | 12 (48) |
| Graduate | 28 | 27 (96.4) | 1 (3.6) | 4 (14.3) | 24 (85.7) |
| Postgraduate | 4 | 4 (100) | 0 | 2 (50) | 2 (50) |
| Illiterate | 7 | 4 (57.1) | 3 (42.9) | 7 (100) | 0 |
| p-value | <0.001* | <0.001* |
| Socioeconomic status |
| Upper | 59 | 41 (69.5) | 18 (30.5) | 34 (57.6) | 25 (42.4) |
| Upper Middle | 28 | 19 (67.9) | 9 (32.1) | 20 (71.4) | 8 (28.6) |
| Middle | 26 | 22 (84.6) | 4 (15.4) | 10 (38.5) | 16 (61.5) |
| Lower middle | 11 | 7 (63.6) | 4 (36.4) | 6 (54.5) | 5 (45.5) |
| Lower | 6 | 2 (33.3) | 4 (66.7) | 6 (100) | 0 |
| p-value | 0.149 | 0.032* |
| Marital status |
| Married | 97 | 68 (70.1) | 29 (29.9) | 59 (60.8) | 38 (39.2) |
| Unmarried | 33 | 23 (69.7) | 10 (30.3) | 17 (51.5) | 16 (48.5) |
| p-value | 0.965 | 0.349 |
| Religion |
| Hindu | 115 | 83 (72.2) | 32 (27.8) | 64 (55.7) | 51 (44.3) |
| Muslim | 15 | 8 (53.3) | 7 (46.7) | 12 (80) | 3 (20) |
| p-value | 0.134 | 0.072 |
Test applied: Chi-square test,
p≤ 0.05 statistically significant
[Table/Fig-4]: A statistically significant association was found between parental smokeless tobacco use and participants smoking and smokeless tobacco usage (p=0.014 and 0.001) respectively. In case of smoking tobacco use, only maternal smoking was significantly associated with participant’s smoking use (p=0.017).
Association of parental tobacco use with participants tobacco use.
| Parental Tobacco Use | Total N | Participant’s Tobacco Use |
|---|
| Smoking | Smokeless |
|---|
| Ever N (%) | Ever N (%) |
|---|
| Paternal Smoking |
| Ever | 89 | 64 (71.9) | 58 (65.2) |
| Never | 41 | 27 (65.9) | 18 (43.9) |
| p-value | 0.484 | 0.022* |
| Maternal Smoking |
| Ever | 12 | 12 (100) | 9 (75) |
| Never | 118 | 79 (66.9) | 67 (56.8) |
| p-value | 0.017* | 0.222 |
| Paternal Smokeless |
| Ever | 62 | 37 (59.7) | 49 (79) |
| Never | 68 | 54 (79.4) | 27 (39.7) |
| p-value | 0.014* | 0.001* |
| Maternal Smokeless |
| Ever | 21 | 15 (71.4) | 19 (90.5) |
| Never | 109 | 76 (69.7) | 57 (52.3) |
| p-value | 0.876 | 0.001* |
Test applied: Chi-square test,
p≤ 0.05 statistically significant
[Table/Fig-5]: The combination of three factors explained for variance in maternal and paternal measures respectively. The factor loadings were assessed using rotated pattern matrix and factor loading plots. All except two measures, {maternal (M7) and paternal expectation (P7)}, were loading heavily on either of the two latent factors. These two factors were dropped from further study for better explanation of latent constructs. The measures that stacked on the same factors were consolidated together through basic summation to register “warmth” and “strictness” factors for each parent.
Rotated factor loadings (pattern matrix) of maternal and paternal bonding measures.
| Item | Factor 1 | Factor 2 | Factor 3 |
|---|
| Maternal |
| M1–How much was she worried about your problems? | 0.528 | 0.013 | –0.412 |
| M2 – How much could you confide in her about things that were bothering you? | 0.699 | 0.021 | –0.059 |
| M3 – How much love and affection did she give you? | 0.151 | 0.222 | –0.668 |
| M4 – How much time and attention did she give you when you needed it? | 0.531 | 0.066 | –0.218 |
| M5 – How strict was she with the rules for you? | 0.149 | 0.825 | –0.045 |
| M6 – How harsh was she when she punished you? | 0.174 | 0.809 | –0.193 |
| M7 – How much did she expect you to do your best in everything you did? | 0.065 | 0.181 | –0.733 |
| Paternal |
| P1 – How much was he worried about your problems? | 0.440 | –0.269 | –0.508 |
| P2 – How much could you confide in him about things that were bothering you? | 0.867 | 0.042 | 0.078 |
| P3 – How much love and affection did he give you? | 0.488 | 0.093 | –0.340 |
| P4 – How much time and attention did he give you when you needed it? | 0.737 | 0.090 | 0.111 |
| P5 – How strict was he with the rules for you? | –0.009 | 0.786 | –0.130 |
| P6 – How harsh was he when he punished you? | –0.210 | 0.599 | –0.541 |
| P7 – How much did he expect you to do your best in everything you did? | 0.056 | –0.096 | –0.869 |
| Percent of Variance | 42.646 | 13.516 | 8.348 |
Kaiser-Meyer-Olkin = 0.802 Barlett’s Test of Sphericity: Chi-square = 568.79 df = 91; p-value ≤ 0.001
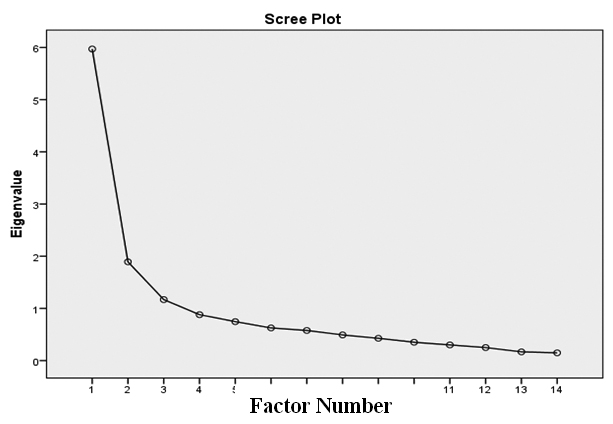
[Table/Fig-6]: shows the rotated pattern matrix for maternal and paternal bonding measures. Both of them showed adequate Kaiser-Meyer-Olkin measure for sampling adequacy (0.802 for maternal and paternal instrument).
Scree plot of paternal and maternal bonding measures.
[Table/Fig-7]: When parental bonding and participants tobacco usage was assessed, maternal warmth index was the only factor which is significantly associated with both participants smoking as well as smokeless tobacco use. Other components like maternal and paternal expectation, paternal warmth and strictness showed significant association with participants smokeless tobacco use only.
Association of parental bonding index with participant’s tobacco use.
| Parental Bonding Index Measures | Participant’s Tobacco Usage |
|---|
| Participant’s Smoking Habit | p- value | Participant’s Smokeless Habit | p-value |
|---|
| Ever | Never | Ever | Never |
|---|
| Mean ± SD | Mean ± SD |
|---|
| Maternal warmth index | 2.81 ± 0.73 | 2.44 ± 0.78 | 0.047* | 2.50 ± 0.75 | 3.03 ± 0.66 | 0.002* |
| Maternal strictness index | 2.68 ± 0.94 | 2.58 ± 0.98 | 0.657 | 2.52 ± 0.92 | 2.87 ± 0.96 | 0.110 |
| Maternal expectation index | 3.01 ± 1.01 | 2.70 ± 1.04 | 0.112 | 2.73 ± 1.13 | 3.22 ± 0.92 | 0.037* |
| Paternal warmth index | 2.75 ± 0.77 | 2.45 ± 0.75 | 0.409 | 2.45 ± 0.71 | 3.00 ±0.74 | 0.001* |
| Paternal strictness index | 2.68 ± 0.93 | 2.87 ± 0.89 | 0.622 | 2.55 ± 0.93 | 3.04 ± 0.84 | 0.018* |
| Paternal expectation index | 2.91 ± 1.06 | 3.04 ± 1.12 | 0.220 | 2.73 ± 1.05 | 3.29 ± 0.90 | 0.024* |
Test applied: Independent sample t-test,
p≤ 0.05 statistically significant
[Table/Fig-8]: depicts the findings of multinomial logistic regression analyses with odd’s ratios (95% CI). There were significant effects for different parental smoking habit on participant’s adverse habits. The risk of smoking among participants increased when mothers smoke (OR 8.3, 95% CI 0.6-0.9). The risk of participants tobacco use was also significantly increased with the paternal smokeless habit (OR 4.5, 95% CI 2-10.1) and maternal smokeless habit (OR 4.5, 95% CI 0.9-22.2).
Multinomial logistic regression analysis with participant’s tobacco use as dependent variables.
| Parameters | N (%) | Participant’s Smoking Habit | Participant’s Smokeless Habit |
|---|
| OR (95% CI) |
|---|
| Paternal Smoking |
| Ever | 89 (68.5) | 1.3 (0.58-3.31) | 1.5 (0.66-3.60) |
| Never | 41 (31.5) |
| Maternal Smoking |
| Ever | 12 (9.2) | 8.3 (0.6-0.91)* | 1.4 (0.28-7.03) |
| Never | 118 (90.8) |
| Paternal Smokeless |
| Ever | 62 (47.7) | 3.2 (0.14-0.75)* | 4.5 (2.0-10.1)* |
| Never | 68 (52.3) |
| Maternal Smokeless |
| Ever | 21 (16.2) | 8.8 (0.26-2.8) | 4.5 (0.92-22.2)* |
| Never | 109 (83.8) |
p≤ 0.05 statistically significant
Discussion
The present study was conducted among 130 patients visiting Pacific Dental College and Hospital of Udaipur city, Rajasthan. This research scrutinized the association between parental and study participants’ tobacco usage and also investigated the association between perceived parental bonding measures and study participants’ tobacco usage. In the previous researches parental influence on their children was seen in either smoking or smokeless habit. Vuolo M et al., found out in his study that parental smoking was strongly associated with adolescent smoking [12]. Similarly, El-Amin et al., reported that parental smokeless tobacco chewing significantly increases the child’s probability of starting the tobacco use [13]. But this research adds to the literature by examining association of both maternal and paternal smoking as well as smokeless tobacco use individually with adults’ tobacco usage along with examining psychosocial intergenerational risk transmission in connection to tobacco usage.
Our study revealed that the prevalence of tobacco use in smoking as well as smokeless form was high among the participants which were in agreement with the other studies conducted by Kaur J et al., and Gupta V et al., who reported high prevalence of tobacco use among cinema attendees and rural-urban-slum urban areas [14,15]. Finding of this study was also consistent with Global Adult Tobacco Survey (GATS) India [6] where they reported current tobacco use in any form was high among adults. When compared to parental side, tobacco use was prevalent among paternal side both in smoking (68.5%) and smokeless form (47.7%).
In the present study no significant difference was observed between participants’ age and their tobacco use. However, our study indicated remarkable significant tobacco usage gender differences. Remarkably our study showed high prevalence of tobacco use among females (27%) which was higher as compared to other studies conducted by Kaur J et al., Gupta V et al., and Rani M et al., [14-16]. The distinction might be due to regional variation, age limit and heavily influence of social pressures and psychological needs including: environmental influences, peer influences, personal factors such as stress, beliefs, poverty etc. Our study showed that smokeless tobacco use was highest among low educated participants and from lower socio-economic status which was similar to the finding of the study conducted by Dixit AM et al., [17]. This might be due to the fact that poor and less educated individuals are less informed of health dangers of tobacco utilization.
Parents can play a very important role in initiation of tobacco use by a young child or adolescent if they use tobacco products in front of their children and the habit that has developed its root in adolescence remains till adulthood and later stages of life. Our results also demonstrated a strong influence of parental tobacco habits on participants tobacco use. We found that paternal smokeless tobacco use was highly associated with participants smoking as well as smokeless habit. A study conducted by Borracci RA et al., also demonstrated that smoking as meagre as one cigarette for each month amid adolescence was emphatically connected with adult tobacco consumption, inferring that many adult smokers could be avoided if smoking was not started in youthfulness [18]. This might be due to that children consider their parents and adults as role models and try to imitate them [19]. When children observe their parents are consuming tobacco, they may indirectly perceive the psychological and physiological rewards of the habit and this coupled with children‘s natural tendency to imitate parents, that could lead to initiation of habit. Such pathways of initiation would be stronger in societies which are interdependent such as India. Maternal tobacco use was also found to be significantly associated with participants tobacco use. The reasons for the apparently more important role of mothers than fathers smoking on adolescent habit are unclear, but might be related to the fact that mothers tend to be more present at home than fathers or that many young adolescents might be closer to their mother than fathers.
Our study revealed that perceived parental bonding measures were significantly associated with participant’s habit. Sociocultural context and family dynamics in India differ from those in the Western world [20]. In developing country such as India, there is a strict adherence to gender roles where the thought of stern father and sympathetic mother has been reported [21]. But strictness can control behaviour temporarily, but they do not help the child to self-regulate. This observation was observed in our results that paternal strictness, which included questions on punishment and enforcement of rules, was significantly associated with the participant‘s habit of tobacco consumption. High paternal strictness may have negatively affected the child‘s psychosocial development contributing to tobacco usage later in life. Along with strictness, paternal warmth and expectation were also associated with participant’s habit.
Our findings demonstrated that parental tobacco habit had significant impact on the participants’ tobacco use. Participants’ whose parents had habit of smoked or smokeless tobacco were more likely to develop tobacco habit. This might be explained by one of the pathways through which children acquire behaviours from their parents are explained by social learning theory [19]. The child can initiate the habit by direct or indirect interaction with a parent. When children observe their parent‘s chewing tobacco, they may indirectly perceive the habit and in order to imitate parents whom they consider their role models, can lead to initiation of the habit of using tobacco. At this phase, parental reinforcement can modify the child‘s behaviour; when the negative reinforcement is absent, the child assumes that the habit is acceptable in the family [21]. A recent systematic review on the social context of smokeless tobacco use summarized the themes which evolved from different qualitative studies assessing determinants of initiation. These themes explain other sociocultural determinants that were familial standards and doubts about beneficial effects of tobacco and purchasing tobacco products for the family members which develops curiosity in them to taste or use the product [22].
Results suggested that parental tobacco usage habits had a direct effect on participant’s tobacco habits. Moreover, parental bonding was also associated with participant’s tobacco usage. The fact that parenting style was highly associated with adult tobacco usage might suggest that they are useful target for preventive intervention. Rather intervention should focus on both parental tobacco specific practices and parental behaviour. These findings suggest that interventions targeted solely at tobacco-specific parenting practices may not be sufficient to deter adolescent tobacco usage and that attempts to change more general parent acceptance and behavioural control may be warranted, even though they may be more difficult to achieve.
Limitation
There were few limitations in the present research. First and foremost, the conditions like tobacco specific practices of both participants and their parents were solely based on the self-perception of the study subjects. We have not done any clinical or objective examination to confirm it. Secondly, there can be other influential factors also affecting these conditions which are not being considered in this study. So the results withdrawn are solely based on subjective perceptions. More such surveys need to be carried out in other parts of the country in order to build comprehensive strategies on anti-tobacco campaigns.
Conclusion
The present study concluded that the tobacco consumption habit shows intergenerational continuity in families. In the intergenerational psychosocial transmission of tobacco consumption habit, mother and fathers play comparable roles. The results suggested that the parental habit of tobacco use is a component of the complex shared social, genetic and environmental factors that contribute to an individual‘s tobacco use. Also participants’ perception of the relationship with their parents well explained this association. Parental bonding measures were significantly associated with the participants’ tobacco habits.
Test applied: Chi-square test,
*p≤ 0.05 statistically significant
Test applied: Chi-square test,
*p≤ 0.05 statistically significant
Kaiser-Meyer-Olkin = 0.802 Barlett’s Test of Sphericity: Chi-square = 568.79 df = 91; p-value ≤ 0.001
Test applied: Independent sample t-test,
*p≤ 0.05 statistically significant
*p≤ 0.05 statistically significant