T2D and associated complications are a major health concern worldwide. Lifestyle intervention is the primary treatment modality for individuals diagnosed with T2D. Diet and physical activity are at the core treatment armamentarium [1,2]. Physical Activity (PA) can even induce remission in recent T2D [3]. Aerobic exercise in the form of cycling can be helpful to reduce the burden of T2D and other non communicable diseases [4]. Cycling, as a form of exercise has vast potential for quick adoption by the young individuals with T2D. Rising incidence of T2D in the young individuals especially below 40 years makes it essential for adoption of such form of PA [5,6]. Though figures on prevalence of T2D in individuals below 40 years are sparse from India, a study from South India observed prevalence of 29.6% in age group of 30 to 39 years [7]. Another study from India, CINDI, reported prevalence of 35% in age group of 31 to 40 years [8]. Such early onset T2D is likely to have obese phenotype and a strong family history of diabetes. Managing T2D young is complex and impacts the course of disease differentially with a greater likelihood of complications at an early age and significant psychological burden of the disease [9].
It is well established that lifestyle intervention is effective at improving glycaemia, blood pressure and reducing complications [10] and is also recommended by guidelines [11,12]. However, there are not many programs done for its effective implementation in T2D especially in young so as to induce diabetes remission or to reduce glycaemic burden substantially. Implementing such program in motivated individuals can be helpful in long term [13]. Aerobic, resistance and/or combined exercise training improves glycaemia and blood pressure in T2D [14]. However, the evidence on effect of any such exercise intervention is relatively lacking in Indian young T2D individuals. In this retrospective study, we assessed effect of cycling exercise for six months on HbA1c%, BP, and weight in young T2D.
Materials and Methods
In this retrospective, observational study, participants were identified from a group of cyclists in a metro city from India. The inclusion criteria were: 1) young age (18 to <40 years); 2) known type 2 DM; 3) treated with ≤ 2 OADs; 4) baseline HbA1c above 7%; and 5) readings of HbA1c%, BP and weight available from records at baseline (i.e. before start of cycling program) and after six months of cycling. The exclusion criteria were: 1) patients of type 1 DM; 2) any patient receiving insulin; 3) involved in exercise other than cycling. This study was conducted at Delhi Diabetes Research Centre between September 2014 and May 2015.
All the participants were involved in cycling for distance of 25 km per day, for at least five days a week. Though optimal duration of lifestyle intervention is not clear, we selected minimum six months of cycling to ascertain that clinically meaningful difference in parameters assessed can be observed. Patients with T2D meeting specified criteria were identified. Clinical data were recorded from patient files. During cycling, patients had continued their medications. Based on age, we had divided participants into two groups as < 35 years and ≥ 35 years which were referred as very-young and young ages respectively. The study was conducted in accordance with ethical principles of Declaration of Helsinki and was approved from Institutional Ethics Committee. A verbal consent was obtained from all the participants to gain access to their medical records.
Statistical Analysis
Baseline and six-months data on HbA1c%, Systolic BP (SBP), Diastolic BP (DBP) and weight were obtained from patient records. Mean reduction in these parameters from baseline to six-month was assessed with paired sample t-test. Data presented as mean (SD) and mean reduction (95% confidence interval (CI)). Age groups wise comparison was done to assess effect of age. A p-value <0.05 was considered significant. Data analysis was conducted using SPSS software for windows version 15.
Results
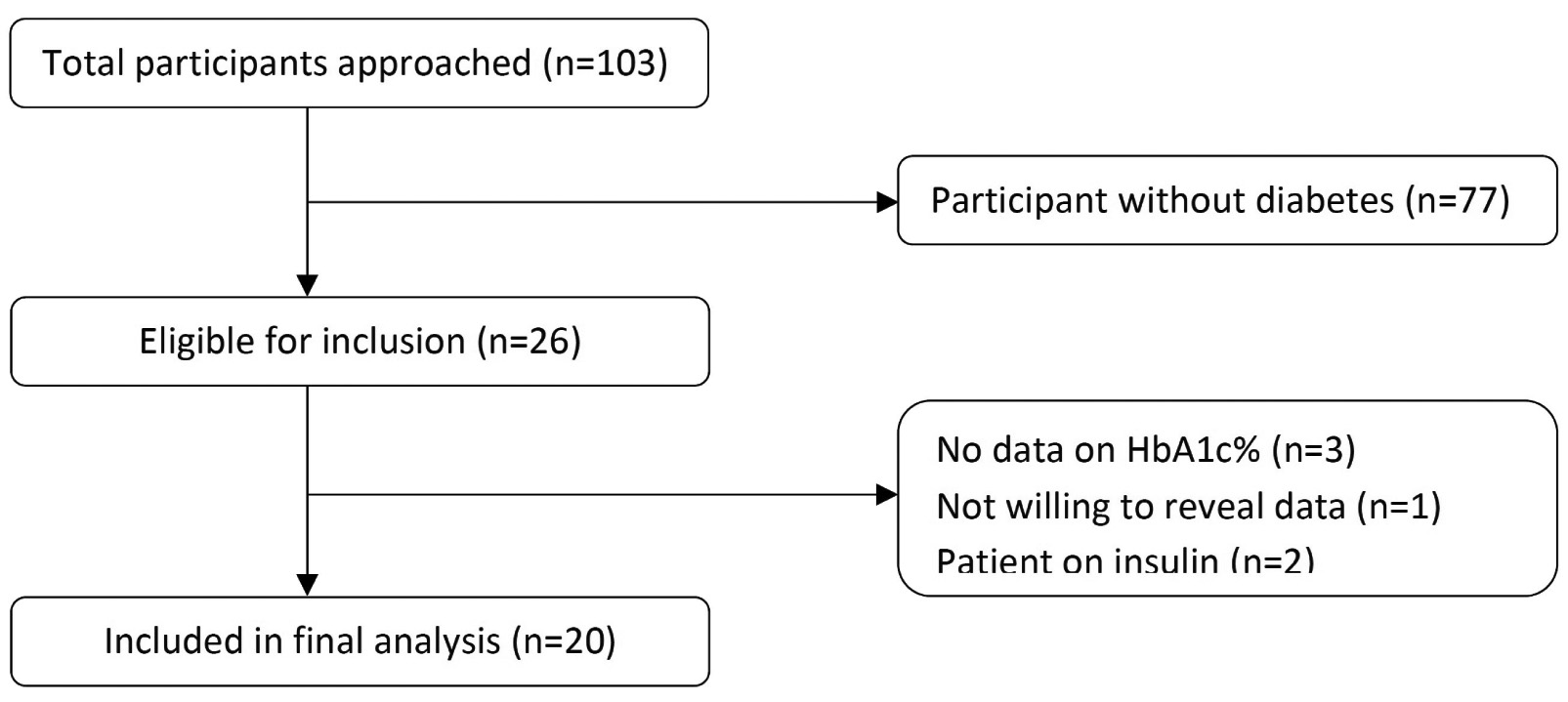
We approached 103 cyclists of which 26 had T2D. From these, 20 were included in final analysis whereas six were excluded because of non availability of data on follow up HbA1c levels (n=3), receiving basal insulin (n=2) and not willing to reveal records (n=1) [Table/Fig-1]. Mean (SD) age of the study population was 35.6±2.6 years with range from 29 to 38 years. All participants were males. Among participants evaluated for entry in to the study, none of the female participant had T2D and therefore no females were included in study. Mean HbA1c% at baseline (i.e., before the start of cycling program) and six-months after cycling were 9.14±0.27 and 7.96±0.19 respectively. [Table/Fig-2] depicts the change in HbA1c%, BP, and weight parameters. Change from baseline in HbA1c% to six months was statistically significant (mean reduction -1.18, 95% CI -1.12, -1.24; p<0.001). Similarly, reduction in systolic BP (mean reduction -5.2 mmHg, 95% CI -3.7, -6.6; p<0.001), diastolic BP (mean reduction -3.1 mmHg, 95% CI -1.7, -4.5; p<0.001) and weight (mean reduction -5.0 kg, 95% CI -4.41, -5.58; p<0.001) were statistically significant.
Flow chart of the participants included in the study.
Change in HbA1c, blood pressure and weight from before entry to six months after cycling. Paired sample t-test used
| Parameters | Baseline | 6 Months |
|---|
| HbAlc (%) |
| Mean±SD | 9.14±0.27 | 7.96±0.19 |
| Mean Change from baseline (95% CI) | - | -1.18 (-1.12, -1.24) p<0.001 |
| SBP (mmHg) |
| Mean±SD | 127.5±9.3 | 122.3±7.7 |
| Mean Change from baseline (95% CI) | - | -5.2 (-3.7, -6.6) p<0.001 |
| DBP (mmHg) |
| Mean±SD | 77.8±6.0 | 74.7±4.4 |
| Mean Change from baseline (95% CI) | - | -3.1 (-1.7, -4.5) p<0.001 |
| Weight (Kg) |
| Mean±SD | 82.3±3.3 | 77.3±2.3 |
| Mean Change from baseline (95% CI) | - | -5.0 (-4.41, -5.58) p<0.001 |
SBP: Systolic Blood Pressure, DBP: Diastolic Blood Pressure, SD: Standard Deviation, CI: Confidence Interval.
Further analysis stratified by age < 35 years (n=5) and ≥ 35 years (n=15) revealed similar results [Table/Fig-3]. Mean reduction in HbA1c% in two groups was -1.14 (95% CI -1.03, -1.25; p=0.018) and -1.2 (95% CI -1.12, -1.27; p<0.001) respectively. Similarly, SBP and weight were significantly reduced in both age groups. However, mean reduction in DBP reached significance only in patients aged ≥ 35 years (p=0.001) but not in those aged < 35 years (p=0.160).
Change in HbA1c, blood pressure and weight in patients aged <35 and ≥ 35 years. Paired sample t-test used.
| Parameters | N | Baseline | 6 Months | Mean Reduction(95% CI) | P-value |
|---|
| HbAlc (%) |
| Age < 35 | 5 | 9.04±0.21 | 7.90±0.14 | -1.14 (-1.03, -1.25) | 0.018 |
| Age ≥ 35 | 15 | 9.17±0.28 | 7.97±0.20 | -1.2 (-1.12, -1.27) | <0.001 |
| SBP (mmHg) |
| Age < 35 | 5 | 122.6±5.5 | 118.2±4.5 | -4.4 (-2.5, -6.2) | 0.003 |
| Age ≥ 35 | 15 | 129.1±9.9 | 123.6±8.1 | -5.5 (-3.5, 7.3) | <0.001 |
| DBP (mmHg) |
| Age < 35 | 5 | 76.8±4.1 | 74.0±3.2 | -2.8 (1.7, -7.3) | 0.160 |
| Age ≥ 35 | 15 | 78.1±6.6 | 74.9±4.8 | -3.2 (-1.5, -4.8) | 0.001 |
| Weight (Kg) |
| Age < 35 | 5 | 81.2±2.3 | 76.6±1.8 | -4.6 (-3.92, -5.30) | 0.001 |
| Age ≥ 35 | 15 | 82.7±3.5 | 77.6±2.4 | -5.1 (-4.46, -5.90) | <0.001 |
Discussion
In this retrospective evaluation of young T2D, we observed significant improvements in glycaemia, blood pressure and weight after a daily cycling during a six-month time period. Lifestyle intervention is known to provide these benefits. A systematic review of studies involving lifestyle intervention reported significant reduction in BMI (−0.29, 95% CI, −0.52 to −0.06, p = 0.014), HbA1c% (−0.37, 95% CI, −0.59 to −0.14, p = 0.001), SBP (−0.16, 95% CI, −0.29 to −0.03, p = 0.016), and DBP (−0.27, 95% CI = −0.41 to −0.12, p < 0.001) [10]. These results substantiate our finding of significant reduction in HbA1c, BP and weight after cycling. Similar findings have also been reported in a long term Look AHEAD trial. Compared to diabetes support and education, intensive lifestyle intervention was associated with greater weight loss (-6.15% Vs -0.88%, p<0.01) and significant reduction in HbA1c levels (−0.36% vs −0.09%; p<0.01), systolic (−5.33 vs −2.97 mm Hg; p=0.001) and diastolic (−2.92 vs −2.48 mmHg; p=0.01) blood pressure. Improvements in treadmill fitness and lipids like high density lipoprotein cholesterol and triglycerides occurred simultaneously [15]. In a study assessing effect of weight change after diagnosis of diabetes on glycaemic control; young age at diagnosis, male gender, lower level of obesity at baseline, weight gain/weight stable with lower weight variability and start of anti diabetic treatment were the important factors associated with inadequate glycaemic control [16]. Improvement in HbA1c by exercise training can be achieved to a level to significantly reduce the risk of complications associated with T2D [17]. These findings corroborate the need for integration of physical intervention in young males especially with obese T2D to improve weight and cardio metabolic risk factors.
In our study, we only assessed the individuals who performed cycling with a group of cyclists. However, even recreational or commuter cycling can be helpful as reported in a Danish cohort study. In adults aged 50 to 65 years, study reported lower risk of incident T2D with increasing duration of cycling per week (multivariable adjusted hazard ratios were 1, 0.87, 0.83, 0.80 and 0.80 for 0, 1–60, 61–150, 151–300, and >300 minutes/week of total cycling respectively) performed as recreational or commuter cycling [18]. A model analysis of cycling promotion for work and schools in Florence reported lower rate of incident T2D, acute myocardial infarction and stroke with overall significant decrease in economic burden [4]. This finding suggests cycling, either recreational or commuter, even in late ages lowers risk of incident T2D. Promoting cycling in all forms, in office goers, school children or virtually in every individual is thus needed to derive maximum benefits. Cycling from early ages can be beneficial on incremental basis.
To ascertain any difference in benefits derived from cycling in very-young (<35 years) and young (≥ 35 years), we found similar benefits across both age groups. This suggests cycling benefits all ages either young or old. Benefits that can obtained with aerobic exercise training in T2D individuals include reduction in HbA1c, improvement in VO2max, reduction in low density lipoprotein and increase in insulin sensitivity [2,19].
Limitation
In this retrospective evaluation from a single city with limited number of cyclists, number of participants was limited. As only males were assessed, generalizability of results is limited and need validation in a large sample with inclusion of both genders. We evaluated effect only on three parameters - HbA1c, BP and weight. Additive benefits on lipids and other cardiometabolic factors need to be evaluated to ascertain benefits in reducing overall cardiovascular risk. We only looked at T2D individuals. Comparison of the findings with control is essential to know the differences in benefits achieved in relation to diabetes. Post cycling effect on weight and the outcomes in T2D need to be evaluated as weight changes after exercise are known to adversely affect the disease course and outcomes [16,20]. Effect of combined resistance training was not evaluated since greater benefits can be derived with combined aerobic and resistance exercise [2,14]. Limited number of participants in age group comparison limits the generalisability of these results.
Conclusion
In young (18 to <40 years) T2D individuals, cycling exercise over six months is associated with significant improvement in HbA1c, BP and weight. The effect is consistent in young adults <35 and 35-40 years age. Cycling should be promoted in all individuals with or without T2D as exercise is known to reduce incident T2D and improve cardio metabolic risk factors substantially. Adoption of cycling can be easy and involvement in a cycling group can be helpful in maintaining adherence especially in young T2D individuals. The benefits derived from exercise therapy can have major impacts on health related expenditures in T2D.
SBP: Systolic Blood Pressure, DBP: Diastolic Blood Pressure, SD: Standard Deviation, CI: Confidence Interval.