Primary Squamous Cell Carcinoma of Submandibular Salivary Gland: A Case Report
Manmohan Agarwal1, Lakshmi Agarwal2, Rajeev Saxena3
1 Consultant, Department of Oncosurgery, Pushpadi Cancer Care Center, Kota, Rajasthan, India.
2 Assistant Professor, Department of Pathology, Govt. Medical College, Kota, Rajasthan, India.
3 Professor, Department of Pathology, Govt. Medical College, Kota, Rajasthan, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Lakshmi Agarwal, 34A, Sreenathpuram, Near Ahinsa Circle, Kota-324005, Rajasthan, India.
E-mail: drlaxmiagarwal@gmail.com
Primary Squamous Cell Carcinoma (PSCC) of submandibular salivary gland is a rare occurrence. Careful clinical and histopathological examination is must to diagnose it. The treatment protocol of this rare disease is not clearly defined. Though surgery is primary treatment, role of adjuvant treatment is not clear. A 40-year-old male presented to us with asymptomatic upper neck swelling. Triple endoscopy, cross-sectional investigation and FNAC suggested primary squamous cell carcinoma of right submandibular salivary gland. He was treated with bilateral modified neck dissection and wide excision of sub mandibular gland with surrounding muscles. Post surgery, he had undergone interval chemotherapy followed by radiotherapy. The patient is still on regular follow up at an interval of three months without any evidence of disease recurrence. Though difficult to diagnose and treat this kind of rare variant of salivary neoplasms, awareness of the disease and aggressive treatment depending on histopathology report, can help patient to achieve health.
Extra Capsular Extension, Muco-epidermoid carcinoma, Salivary neoplasms
case report
A 40-year-old male, known tobacco chewer for last 20 years, nonsmoker, complained of gradually increasing swelling in right submandibular region since six months. It was not associated with any other complaints of oral or oro pharyngeal symptoms or any constitutional symptoms. There was no previous history of radiation to neck. Clinical examination of oral cavity and pharynx did not reveal any abnormality. There was a swelling of 3 x 3 cm at right submandibular region which was firm to hard in consistency and fixed to mandible. There were no palpable nodes found in the head and neck region of both sides. Triple endoscopy and other investigations were within normal limits.
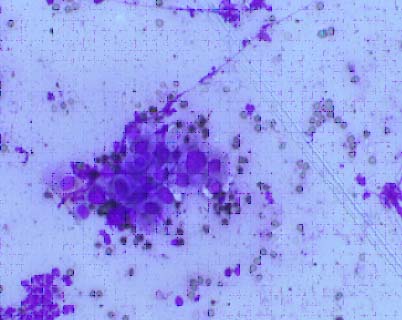
CECT of head and neck revealed a mass of 3 x 3 cm at submandibular region infiltrating digastric muscle and mylohoid muscle. Fine needle aspirate was done and differential diagnosis of squamous cell carcinoma and high grade mucoepidermoid carcinoma was made [Table/Fig-1].
Giemsa stain, 40X, Smear revealing the cluster of malignant squamous cells.
Sonography of neck (both sides) revealed multiple enlarged lymph nodes at level II/III of right side. Wide local excision of submandibular gland along with mylohyoid and digastric muscle excision with marginal mandibulectomy and bilateral neck dissections (comprehensive neck dissection of ipsilateral side and supraomohyoid neck dissection of contralateral side) were done [Table/Fig-2].
Post surgery bilateral neck dissection.

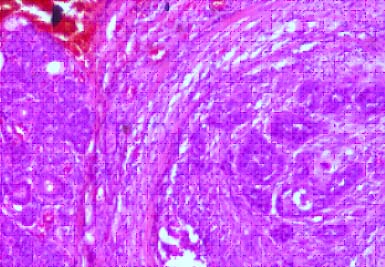
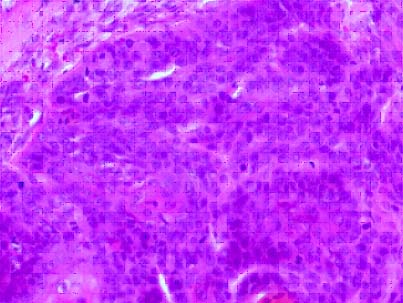
Specimen was sent for histopathology examination. Grossly, specimen of salivary gland showed an infiltrating grey white mass measuring 4 x 3 x 1.3 cm. On microscopy, submandibular gland showed well differentiated squamous cell carcinoma [Table/Fig-3,4].
H&E stain, 40X, showing normal salivary gland and malignant squamous cells.
H&E stain, 40X, showing malignant squamous cells.
Perineural and lymphovascular invasion were present. Total 15 lymph nodes were identified and four nodes revealed tumour deposits (4/15). Extra Capsular Extension (ECS) was present. The mucicarmine stain was negative which ruled out mucoepidermoid carcinoma. Diagnosis of PSCC of submandibular gland was made. The case was discussed in the tumour board. Due to lack of established guidelines and presence of multiple positive nodes with pathological stage pT2, N2b, M0, patient was planned for interval chemotherapy followed by concurrent chemoradiotherapy. The patient received three cycle of chemotherapy (cisplatin 50 mg/m2 and paclitaxel 175 mg/m2) followed by EBRT (60 gy) to the neck with weekly cisplatin. The patient is still on regular follow up at an interval of three months.
Discussion
PSCC represents less than 1% of salivary gland tumours. Roughly 80% of PSCC arise in the parotid gland and 20% in the submandibular gland [1]. Flynn MB et al., conducted a study of 370 malignant parotid tumours over a period of 20 years out of which only eight (2%) were reported to be primary squamous cell carcinoma [2]. PSCC occurs in the 6th to 8th decades. Male to female ratio is 2:1. It has been associated with a history of prior radiotherapy; with a latent period of 15-30 years [1]. It is considered as relatively high grade, aggressive salivary carcinoma. Five year disease specific survival is approximately 25-30% [3].
Patients with PSCC of sub mandibular gland usually presents as a hard mass, often fixed, with a short history of one year or less. The tumour is often asymptomatic as in the present case but 20% of patients may have a painful mass. Neck metastases occur in nearly 50% of patients [3], which were also observed in this patient.
Differential diagnosis for the present case considered were: (1) High grade mucoepidermoid carcinoma; (2) a metastasis or direct invasion from a cutaneous or mucosal squamous carcinoma of the head and neck; (3) a metastasis from a distant primary carcinoma; or (4) primary squamous carcinoma. Histologically, squamous carcinoma in a major salivary gland is a keratinizing tumour that cannot be differentiated from the secondary/metastatic squamous cell carcinoma. Clinically, the precise identification of origin is also frequently unclear. Histologic grading of the squamous element seems to have no prognostic value [4,5]. The presence of squamous component indicates an aggressive tumour regardless of the origin and nature of the disease [5].
There is limited literature regarding the treatment modalities of PSCC of salivary gland [6,7] as with other primary salivary tumours, the initial therapeutic approach irrespective of origin is surgical excision. Additional treatment, whether radiation or chemotherapy, depends on the extent of tumour distribution [8]. Role of postoperative chemo-radiation for salivary gland malignancy is not well established [9]. The stage of tumour is the most important prognostic factor. In the present case, the patient was treated with interval chemotherapy and adjuvant chemoradiotherapy due to the presence of multiple metastatic nodes in the neck which further signifies the increase in the probability of distant failure.
Conclusion
PSCC of submandibular gland is a rare and aggressive tumour with poor prognosis. Its diagnosis is a challenge to pathologist as differentiating from metastatic tumours or other primary malignant tumours such as mucoepidermoid carcinoma is difficult. Hence, timely diagnosis and aggressive management by surgery, chemotherapy and radiotherapy can help in prolonging patient’s survival.
[1]. Barnes L, Eveson JW, Reichart P, Sidransky D, Pathology and genetics of head and neck tumours 2005 LyonIARC Press:245 [Google Scholar]
[2]. Flynn MB, Maguire S, Martinez S, Primary squamous cell carcinoma of the parotid gland: The importance of correct histological diagnosisAnn Surg Oncol 1999 6(8):768-70. [Google Scholar]
[3]. Shivakumar T, Nair VS, Joshi P, Chaturvedi P, A review of Salivary gland neoplasms and its managementOtolaryngology Online Journal 2014 4(3):41-60. [Google Scholar]
[4]. Manvikar V, Ramulu S, Ravishanker ST, Chakravarthy C, Squamous cell carcinoma of submandibular salivary gland: A rare case reportJ Oral Maxillofac Pathol 2014 18(2):299-302. [Google Scholar]
[5]. Taxy JB, Squamous carcinoma in a major salivary gland. A review of the diagnostic considerationsArch Pathol Lab Med 2001 125:740-45. [Google Scholar]
[6]. Cortesina G, Airoldi M, Palonta F, Current role of chemotherapy in exclusive and integrated treatment of malignant tumours of salivary glandsActa Otorhinolaryngol Ital 2005 25(3):179-81. [Google Scholar]
[7]. Lagha A, Chraiet N, Ayadi M, Krimi S, Allani B, Rifi H, Systemic therapy in the management of metastatic or advanced salivary gland cancersHead and Neck Oncology 2012 4:19 [Google Scholar]
[8]. Bell RB, Dierks EJ, Homer L, Management and outcome of patients with malignant salivary gland tumoursJ Oral Maxillofac Surg 2005 63(7):917-28. [Google Scholar]
[9]. Speight PM, Barrett AW, Salivary gland tumoursOral Diseases 2002 8:229-40. [Google Scholar]