Pleural and Mediastinal Lipomatosis with Subpleural Fat as a Mimicker of Pleural Effusion- A Rare Case Report
Navkiran Kaur1, Jasvir Singh2, Samrin Haq3, Sugandha Garg4, Simmi Bhatnagar5
1 Professor and Head, Department of Radiology, GMC Patiala, Patiala, Punjab, India.
2 Junior Resident, Department of Radiology, GMC Patiala, Patiala, Punjab, India.
3 Junior Resident, Department of Radiology, GMC Patiala, Patiala, Punjab, India.
4 Junior Resident, Department of Radiology, GMC Patiala, Patiala, Punjab, India.
5 Assistant Professor, Department of Radiology, GMC Patiala, Patiala, Punjab, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Jasvir Singh, Room No. 32, Doctor Hostel RHP, Patiala-147001, Punjab, India.
E-mail: jasvirsingh011789@gmail.com
Subpleural and mediastinal lipomatosis are benign intrathoracic conditions discovered incidentally on plain chest radiographs. However, diagnosis is usually made by Computed Tomography (CT). A case of both mediastinal and pleural lipomatosis associated with use of steroids in a 58-year-old male patient presented with complaints of breathlessness and dry cough is discussed in this case report. Intially, pleural effusion and bilateral upper lobe patchy opacities were suspected as a cause of breathlessness on the basis of chest x-ray findings. For which, CT scan of chest was advised.
CT scan, Lipoma, Pleural effusion
Case Report
A 58-year-old male patient came to our hospital with complaints of breathlessness and dry cough since 10 days. He was suffering from congestive cardiac failure and bilateral pedal oedema in the past and he was taking prednisolone 30 mg since last two years for the same. After that he was referred to Radiology Department for further evaluation. X-Ray and CT scan of chest were done. On X-ray, superior mediastinum widening was seen and bilateral upper zones appear hazy with blunting of left costophrenic angle was seen mimicking as pleural effusion [Table/Fig-1]. So, CT scan was advised. Due to deranged renal function tests, only Non-Contrast Enhanced Computed Tomography (NCCT) and High Resolution Computed Tomography (HRCT) scans of chest were possible which showed homogenous unencapsulated fat attenuating region involving the mediastinum and pleura bilaterally mainly in upper lobes and in left lateral costophrenic angle [Table/Fig-2,3] with a small patch of consolidation was also seen in superior segment of left lower lobe [Table/Fig-3c] which was later confirmed histologically [Table/Fig-4] (done for diagnostic purpose only). Fine Needle Aspiration Cytology (FNAC) was done and specimen was stained with haematoxylin and eosin showed well-differentiated adipocytes. No pleomorphism, necrosis, or mitotic activity was noted in the histological stained specimen. Other laboratory investigations were within normal limits including complete blood count, liver function tests, serum calcium levels. In routine urine examination and microscopy, the traces of albumin and 1-2 RBCs were noted. Patient was given antibiotic prophylaxis for patchy consolidation patch. Provisional diagnosis made after CT scan was mediastinal and pleural lipomatosis with a small patch consolidated patch. After provisional diagnosis differential diagnosis include pleural effusion and mesothelioma. Pleural lipoma serves as a mimicker of pleural effusion. On CT scan, effusion shows fluid attenuation (10-20 H.U.) while lipoma is a fat attenuation lesion. Sometime, pleural lipoma may mimics as mesothelioma. However, fat attenuation of pleural lipoma on NCCT scan and contrast enhancement of mesothelioma helps to differentiate these two entities. Final diagnosis was same as provisional after FNAC report. Patient was followed after three months, he was symptomatically improved. No other treatment was given.
Chest x-ray shows superior mediastinal widening with hazy bilateral upper zones and blunting of left costophrenic angle mimicking as pleural effusion (indicated by marker).

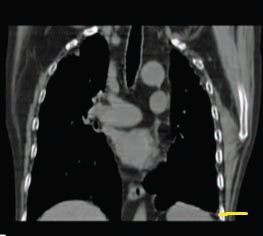
Coronal CT image shows blunting of left costophrenic angle due to pleural fat (indicated by marker).
Axial CT images show fat attenuating region around the pleura and mediastinum suggestive of pleural and mediastinal lipomatosis (indicated by marker in 3a,3b,3c) and a small patch of consolidation was seen in superior segment in left lower lobe (marked by star mark in 3c).

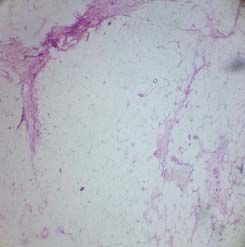
Photomicrograph of the biopsy material (stained with haematoxylin and eosin with 4x resolution) shows well-differentiated adipocytes consistent with diagnosis of lipoma.
Discussion
Lipomas are benign tumours composed of mature adipocytes. They are the most common soft tissue tumour seen in approximately 2% of the population. It is most common in the upper mediastinum. It is associated with iatrogenic steroid use, Cushing’s syndrome, obesity [1]. Mediastinal lipomatosis is a relatively common benign cause of mediastinal widening [1]. It is the result of increased deposition of normal unencapsulated fat [2]. Lipomas usually occur at the mediastinal, bronchial and pulmonary levels, a pleural lipomas are extremely rare [3]. Symptoms can include dysphagia, difficulty in breathing, dry cough and cardiac arrhythmias [4]. They constitute 1.6%–2.3% of all primary mediastinal tumours and predominantly involve the anterior mediastinum [5]. Routinely these are insidious in onset and on chest radiography they usually go unnoticed until a well-defined abnormal shadow is identified on radiograph [6]. Occasionally, a prominent epicardial fat pad can result in a mediastinal mass [7].
Submesothelial layer of parietal pleura serves as a source of origin of pleural lipoma extending into the subpleural, pleural or extrapleural spaces [8]. On plain chest x-ray, they are discovered incidentally and appear as well defined, convex lesions forming obtuse angles with the pleura. Lipomas are vertically oriented in relation to the chest wall and appear denser than fat because of interface with air in the lung. These are benign tumours hence not associated with rib erosion [9]. CT chest helps to differentiate between benign and malignant pleural disease and determine the extent and location of disease. The radiological diagnostic criteria for pleural lipoma on CT is as follows: a nodular appearing well-defined area of homogeneous fat attenuation (ranging from -50 to −150 HU), which is not enhanced by an injected contrast medium, forming obtuse angles with the adjacent chest wall and causing displacement of adjacent pulmonary parenchyma and vessel [3,10]. On MRI, a well-defined homogenous mass that is hyperintense on T1 and moderately intense on T2-weighted images [11]. Fat-suppression sequences may aid in cases of diagnostic doubt. Differentiation between liposarcomas and lipomas may be challenging on CT images. In our case, both mediastinal and pleural lipomatosis were present, simultaneous occurrence of both is a rare entity as only eight cases of pleural lipomatosis has been reported and many cases of mediastinal lipomatosis have been reported. But no case of mediastinal lipomatosis in association with pleural lipomatosis has been reported which makes our case rare. Pleural fat was also seen in left lateral costophrenic angle mimicking as a pleural effusion which is often misinterpreted on conventional x-ray as a pleural effusion.
Liposarcomas are the malignant tumours of fatty tissue. In contrast to lipomas, they tend to produce symptoms. On NCCT scan, they are large soft tissue masses of fatty attenuation which infiltrate the surrounding tissues. On MRI, they show high signal intensity on T2- weighted images due to myxoid degeneration and low signal intensity on T1 weighted images. Because they grow slowly, the presenting symptoms are often due to mass effect (i.e., compression of the primary bronchi, oesophagus, phrenic nerve or vagus nerve) [11].
Treatment: Mediastinal lipomatosis usually treated by conservative measures that involves weight reduction. However, surgery might be needed in rare circumstances [12]. Tapering off steroids is usually needed in steroid induced lipomatosis [13]. Pleural lipomatosis transformation into a sarcoma is rare. So, no management is needed. However, recently it has been suggested that they have potential to grow, and also due to the advances in Video-Assisted Thoracic Surgery (VATS), they can be managed accordingly [3].
Conclusion
Pleural and mediastinal lipomatosis occurring simultaneously in same patient is a rare entity. Also, pleural lipomatosis can serve as a mimicker of pleural effusion. So, lipoma should be considered as one of the common aetiologies before labeling it as a case of idiopathic effusion. CT scan plays an important role in identifying the pleural as well as mediastinal lipomatosis in case of inconclusive x-ray findings. CT also helps in differentiating these entities from other causes of mediastinal widening and pleural based masses.
[1]. Brant WE, Helms C, Fundamentals of Diagnostic Radiology 2012 1st edLippincott Williams & Wilkins [Google Scholar]
[2]. Srichai MB, Computed Tomography and Magnetic Resonance of the Thorax 2007 Lippincott Williams & Wilkins [Google Scholar]
[3]. Jayle C, Hajj-Chahine J, Allain G, Pleural lipoma: a non-surgical lesionInteract Cardiovasc Thorac Surg 2012 14(6):735-38. [Google Scholar]
[4]. Cutilli T, Schietroma M, Marcelli VA, Ascani G, Corbacelli A, Giant cervico-mediastinal lipoma: a clinical caseMinerva Stomatol 1999 48:23-28. [Google Scholar]
[5]. Politis J, Funahashi A, Gehlsen JA, DeCock D, Stengel BF, Choi H, Intrathoracic lipomas: report of three cases and review of the literature with emphasis on endobronchial lipomaJ Thorac Cardiovasc Surg 1979 77:550-56. [Google Scholar]
[6]. Kato M, Saji S, Kunieda K, Yasue T, Nishio K, Adachi M, Mediastinal lipoma: report of a caseSurg Today 1997 27:766-68. [Google Scholar]
[7]. Fan CM, Lipomatous hypertrophy of the interatrial septum: Increased uptake of FDG PETAJR Am J Roentgenol 2005 184:339-42. [Google Scholar]
[8]. Sakurai H, Kaji M, Yamazaki K, Suemasu K, Intrathoracic lipomas: their clinicopathological behaviors are not as straightforward as expectedAnn Thorac Surg 2008 86:261-65. [Google Scholar]
[9]. Gaerte SC, Meyer CA, Winer-Muram HT, Fat-containing lesions of the chestRadiographics 2002 22:61-78. [Google Scholar]
[10]. Karlo CA, Stolzmann P, Frauenfelder T, Donati OF, Leschka S, Computed tomography imaging of subpleural lipoma in two men: two case reportsJ Med Case Rep 2010 4:380 [Google Scholar]
[11]. Davies CW, Gleeson FV, Davies RJ, BTS guidelines for the management of pleural diseases 2003 LondonArnold:210-37. [Google Scholar]
[12]. Nguyen KQ, Hoeffel C, Le LH, Phan HT, Mediastinal lipomatosisSouth Med J 1998 91:1169-72. [Google Scholar]
[13]. Sorhage F, Stover DE, Mortazavi A, Unusual etiology of cough in a woman with asthmaChest 1996 110:852-54. [Google Scholar]