“Quirky Bulb” On the Lower Jaw: An Organizing Haematoma
Raghavendra Mahadev Naik1, Ramanjaneya Raju Pennemetsa2, Sudhakara Reddy3, Praveen Gadde4, Sruthi Rayapureddy5
1 Reader, Department of Oral Medicine and Radiology, Vishnu Dental College, Bhimavaram, Andhra Pradesh, India.
2 Reader, Department of Oral Patholgy, Vishnu Dental College, Bhimavaram, Andhra Pradesh, India.
3 Professor, Department of Oral Medicine and Radiology, Vishnu Dental College, Bhimavaram, Andhra Pradesh, India.
4 Senior Lecturer, Department of Public Health Dentistry, Vishnu Dental College, Bhimavaram, Andhra Pradesh, India.
5 Postgraduate Student, Department of Oral Medicine and Radiology, Vishnu Dental College, Bhimavaram, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Raghavendra Mahadev Naik, Reader, Department of Oral Medicine and Radiology, Vishnu Dental College, Bhimavaram-534202, Andhra Pradesh, India.
E-mail: dr.raghmn@gmail.com
Organizing Haematoma is a rare, non/neoplastic benign lesion with locally destructive behaviour that may mimic a malignancy. Usually symptoms do not occur, while the lesion remains localized. An Organized Haematoma is an encapsulated blood clot undergoing neovascularization and fibrosis. It has also been referred to as a hemophilic pseudotumour and/or a haematoma like tumour, which is rarely found in the head and neck region. Other reported cases have been related to trauma or an underlying haemangioma. However, most of the cases have no identifiable underlying pathology, trauma or systemic disease. We are reporting an unusual presentation of Organizing Haematoma over the edentulous mandible.
Blood clot, Mandible mass, Radiograph, Traumatic injuries
Case report
A 52-year-old female patient visited Vishnu Dental College and Hospital, Bhimavaram in the month of August 2014 with the chief complaint of swelling in the left lower front teeth region since three months. Patient was apparently normal before. She started developing a swelling in left mandibular anterior teeth region three months ago. She underwent extraction of teeth with no complications and reported edentulism of jaw since three months. The swelling initially started as peanut size and had slowly progressed to attain the present size. Patient reported no history of bleeding. She gave the history of difficulty in speech. She also reported that swelling has started only after the extraction of left mandibular canine, which was done three months back. Further, history revealed that she was under medication since one year for hypertension and diabetes.
Local examination of the lesion revealed solitary pedunculated growth, roughly oval in shape, measuring approximately 3x2.5 cm which was located on the edentulous ridge of left mandibular canine tooth region and extending lingually to the floor of the mouth, with no surface erosions [Table/Fig-1]. The swelling was found to be erythematous with areas of bluish tinge. The swelling was covered by necrotic debris on the surface and had corrugated appearance. On palpation all inspectory findings were confirmed with respect to size, shape and extent of the growth. The swelling was found to be soft to firm in consistency which was fluctuant, non tender and with no sign of bleeding. Necrotic debris over the growth was removed partially and there was no evidence of pus discharge.
Clinical photograph showing growth on the left edentulous mandibular anterior region.

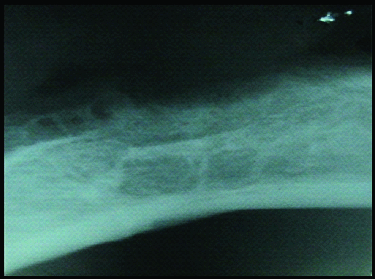
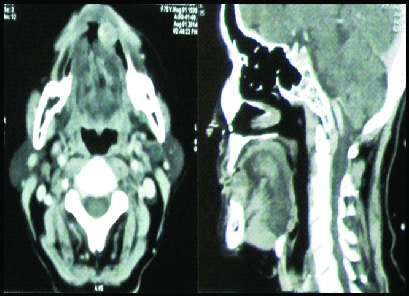
Provisional diagnosis was given as Peripheral giant cell granuloma of left edentulous mandibular anterior region. We advised intraoral periapical radiograph, which revealed multilocular radiolucency with delicate radiopaque striations [Table/Fig-2]. CT scan of this condition showed, focal well defined homogenously enhancing lesion measuring 1.6x1.4 that revealed focal soft tissue growth and the impression was given as soft tissue enhancing lesion in the floor of the mouth [Table/Fig-3]. Complete surgical excision of the lesion was done under local anaesthesia and sent for histopathological examination.
Intraoral periapical radiograph showing multilocular radiolucency at left edentulous mandibular anterior region.
CT images showing mass on the left edentulous mandibular anterior region.
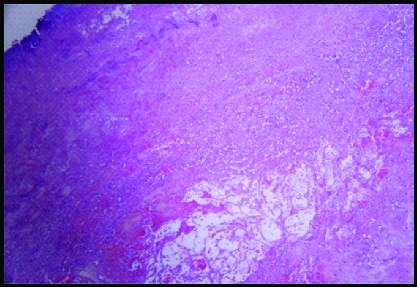
Histopatholgical examination revealed fibrinopurulent membrane overlying haematoma. Bacterial colonies and numerous candidal hyphae were evident at the periphery. Centre of the lesion showed numerous chronic inflammatory cells, hemorrhagic areas, few blood vessels and young fibroblasts suggesting infected Organizing Haematoma [Table/Fig-4]. Postoperative evaluation of the mandibular anterior region after six months revealed normal healing and bone formation [Table/Fig-5].
Histopathology of infected organizing haematoma.
Post treatment photograph showing complete resolution of swelling after six months.

Discussion
When we hear the word haematoma, we often associate it with a postoperative complication that requires incision and drainage and possible intravenous antibiotics when infected. The term haematoma is defined as a swelling or mass of blood that is usually unclotted and is confined to an organ, tissue, or space, and is caused by a break in a blood vessel. Nevertheless, haematomas may be present for months and can often be very debilitating to the patient [1].
Haematomas may develop spontaneously due to a traumatic event or they may develop slowly in a chronic expanding form following surgery or vascular defect. It occurs because the wall of a blood vessel has been damaged and blood has leaked into tissues where it does not belong, finally resulting in significant swelling [2]. It is interesting that our patient gave a history of extraction of teeth in the mandibular anterior region and initiation of the swelling after the extraction. Accordingly, the possible cause for the Organizing Haematoma in the present case appears to be the extraction of teeth in the anterior part of the mandible.
The most plausible theory regarding the etiology and pathophysiology of Organizing Haematoma is chronic haematomas resulting from various causes, such as trauma, surgery, or underlying bleeding tendency, that can develop into Organizing Haematoma. During this process, chronic haematomas undergo several pathophysiologic events including angiogenesis, neovascularization, and surface fibrosis. This complex process results in progressive expansion and local bony erosion associated with Organizing Haematoma [3]. The present case had a similar sequence of events and also showed multilocular radiolucency with delicate radiopaque striations. Differential diagnosis of organizing haematoma is a challenge because the radiographic and CT findings usually are not very specific. Clinical histories of trauma, surgery or hemophilia may be significant clues for Organizing Haematoma [4].
Conclusion
Organizing Haematoma is a rare oral non neoplastic condition and general dental practitioner is often the first professional to detect and establish the diagnosis of this uncommon condition. Extraction of teeth is a regular procedure carried out by dentists and trauma is the major cause for Organizing Haematoma, which may be because of these extractions. So, to avoid inappropriate treatment of this condition, dentists should consider Organizing Haematoma as one of the differential diagnosis for the post surgical slow growing swellings with bony changes.
[1]. Suzuki H, Inaba T, Hiraki N, Hashida K, Wakasugi T, Kadokawa Y, Endoscopic sinus surgery for the treatment of Organized haematoma of the maxillary sinusKurume Med J 2008 55:37-41. [Google Scholar]
[2]. Ohta N, Watanabe T, Ito T, Kubota T, Suzuki Y, Ishida A, Clinical and pathological characteristics of Organized haematomaInt J Otolaryngol 2013 2013:539-642. [Google Scholar]
[3]. Park JY, Lee IH, Song CJ, Kim K, Kim SS, Positron Emission Tomography-CT, CT, and MR Imaging Findings of Tumour-Mimicking Organized Haematoma in the Maxillary Sinus: Two Case ReportsJ Korean Soc Radiol 2011 65:113-17. [Google Scholar]
[4]. Hsu WS, Liu SF, Chu ST, Tseng HH, An Organizing haematoma in the parapharyngeal spaceJ Chin Med Assoc 2009 72:94-97. [Google Scholar]