Orthodontic treatment aims to achieve an ideal arrangement of the teeth over the basal bone for the functional efficiency, structural balance, and aesthetic harmony. Attainment of these goals is eased when the total tooth material is compatible with the available basal bone. Basal bone is a deciding factor of the available arch perimeter for the teeth to accommodate [1].
Malocclusions most commonly result from arch length–tooth size discrepancies wherein, the tooth material or the basal bone or both could be at fault and accordingly the discrepancy can be eliminated by addressing the problem of the tooth size and/or the basal bone. When the tooth material is at fault, a relative change in the total tooth material can be achieved by altering the tooth morphology (e.g., proximal stripping, aesthetic restorations etc.,) and even extraction of one or more teeth depending upon the severity of the discrepancy.
A promising, yet least explored method of altering the effective relation between the tooth material and basal bone is through the change in axial relation of the crown of the tooth in mesiodistal direction, or labiolingual direction.
Andrews LF, in 1972, emphasized the significance of crown angulation and inclination in attainment of optimum occlusion. Andrews postulated that the degree of crown angulation especially the maxillary anteriors, owing to their trapezoidal morphology, determine the amount of mesiodistal space they will occupy within the arch and thus have a potential space implication [2,3].
He further contended that the arch perimeter could also be influenced by degree of crown inclination. Looking from an occlusal view, the incisal edges of the normally aligned maxillary incisors form an arc. The radius of this arc determines the width of the dental arch and in turn the arch circumference. Labial crown torque of maxillary incisors, locate the contact points further labially to conform to the wider arch form, thereby increasing the effective tooth material and increased consumption of arch perimeter. Conversely, lingual crown torque relocates the contact points lingually so that the effective tooth material is reduced and thus results in reduced consumption of arch perimeter [4].
Based on this background, an in vitro study was conducted to quantify the change in the effective arch perimeter, by change in the degree of maxillary incisor crown angulation and inclination.
Materials and Methods
The present in vitro study was carried out in the Department of Orthodontics and Dentofacial Orthopedics, Sharad Pawar Dental College, DMIMS Wardha, Maharastra, India, in association with Department of Mechanical Engineering, VNIT Nagpur Maharastra, India. A working model was constructed in a way that a rigid block of acrylic holds molars, premolars and cuspids on both sides in a fixed position; and modeling wax supported central and lateral incisors.
The purpose behind preparing such working model was to restrict the tooth movement in incisor region only, preventing any reactionary tooth movement in posterior segment, to ensure that effect on the arch perimeter (if any) associated with the change in crown angulation and inclination was limited to the anterior segment only.
The study was carried out in two parts. In the first part, effect of varied crown angulation on the arch perimeter was studied; whereas in the second part, effect of crown inclination on arch perimeter was studied.
1. Study of Effect of Maxillary Incisor Crown Angulation on the Effective Arch Length
Maxillary incisors were arranged on the basic setup simulating spaced anterior segment using modelling wax [Table/Fig-1].
Basic setup with leveled slot posterior segment: a) Before removal of arch wire; b) After removal of arch wire; c) Right lateral view; d) Left lateral view.
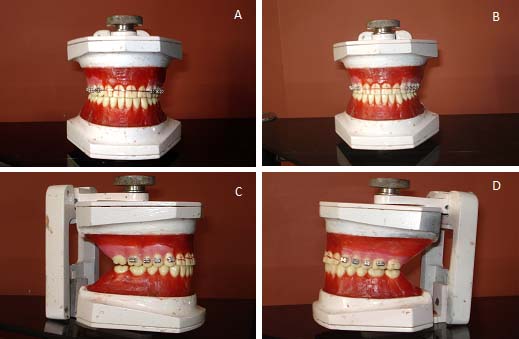
Standard edgewise brackets (0.022” x 0.028” slot) were bonded using light cure composite bonding adhesive (Transbond XT, 3M-Unitek) on the facial surface of all the incisors such that the vertical and horizontal axes of the brackets were along the vertical and horizontal reference lines marked on the facial surface of the crowns respectively [Table/Fig-2]. Marking of reference lines and verification of bracket positioning was done with the help of coordinate measuring machine (CMM Crysta-Apex C 544).
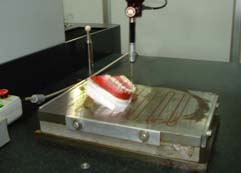
With the help of coordinate measuring machine, the horizontal and vertical reference lines were located and marked on the incisors.

This machine uses a laser probe tip to measure the features of an object. It has three axes; the probe moves along these axes to give an accurate measurement of the item that is being scanned and enables to locate point coordinates on three-dimensional structures, at the same time it integrate both dimensions and the orthogonal relationships.
Distal end of a 0.021“x0.027” NiTi arch wire was annealed and the arch wire was engaged to the bracket slots using steel ligature ties (0.010”). The distal end was cinched back [Table/Fig-3].
Distal end of the arch-wire was cinched back.

The setup was immersed in a hot water bath (50°C) for 15 minute. It was then recovered and bench cooled for overnight at room temperature. Fifty degree temperature was just sufficient to soften the modeling wax without melting it. This ensured that the modeling wax got uniformly softened to allow the tooth movement unhindered.
Following day, the interdental spaces were measured by coordinate measuring machine [Table/Fig-4]. Point at the maximum convexity (contact point) on the mesial and the distal surface of the incisors was located by laser probe. The distance between the distal contact point on the mesial tooth and the mesial contact point of the distal tooth was recorded as the interdental space between the two teeth. The space up to 0.001 mm could be measured with clinical accuracy by using coordinate measuring machine.
Measuring the interdental spaces using coordinate measuring machine.
This measurement acted as an initial measurement with 0° tip in all the incisors.
The arch wire was carefully removed and change in the arch perimeter with varied crown angulation was measured as under:
Measurement of change in the arch perimeter with varying crown angulation:
Step 1 : The brackets of the lateral incisors were removed using a debonding plier. Remnants of composite resin were carefully removed using a scaler. The bracket base was sandblasted and cleaned.
Step 2 : A line of 5° to the initial horizontal reference line was located with the help of coordinate measuring machine and marked on the facial surface of the lateral incisors so that a mesial crown tip was expressed upon wire engagement. Standard edgewise bracket (0.022“´ 0.028” slot) was rebonded on the facial surface, such that horizontal axis of the bracket was along this line.
Step 3 : Angular positions of the brackets were verified using coordinate measuring machine. Thus, by angulating the two lateral incisors by 5° each, total change of 10° of crown angulation was incorporated within the arch.
Step 4 : Interdental spaces in the anterior segment were measured using coordinate measuring machine.
Step 5“ Distal end of a 0.021”´0.027” NiTi arch wire was annealed and the arch wire was engaged to the bracket slots using steel ligature ties (0.010”). The distal end was cinched back. Interdental spaces in the anterior segment were remeasured using coordinate measuring machine to verify and ensure that there was no alteration in the tooth position or interdental spaces during wire engagement.
Step 6 : The setup was immersed in a hot water bath (50°C) for 15 minute. It was recovered and stored at room temperature for overnight. Following day the interdental spaces were measured by coordinate measuring machine.
Step 7 : The arch wire was carefully removed. The brackets of the central incisors were removed using a debonding plier. Remnants of composite resin were carefully removed using a hand scaler. The bracket base was sandblasted and cleaned.
Step 8 : With the help of coordinate measuring machine, a line of 5° to the initial horizontal reference line was located and marked on the facial surface of the central incisors as done for lateral incisors. Standard edgewise brackets (0.022” ´ 0.028” slot) were rebonded on the facial surface such that horizontal axis of the bracket was along this line.
Step 9 : Angular positions of the brackets were verified using Coordinate Measuring Machine. Thus, by angulating the two central incisors by 5°each, total change of 20° of crown angulation was incorporated within the arch.
Step 4 to step 6, as described above, were repeated and measurements were obtained. Similarly the bracket angulation was changed with an increment of 5° upto 25° for both lateral and central incisors (one tooth type at each time), thereby further incorporating a total crown angulation of 30°, 40°, 50°, 60°, 70°, 80°, 90°, 100° within the arch. Step 1 to step 6 were repeated for each 10° increment in total crown angulation and records were made.
2. Study of Effect of Maxillary Incisor Crown Inclination on the Effective Arch Perimeter
Step I : Maxillary incisors were arranged on the basic set up simulating spaced anterior segment using modelling wax.
Step II : Pre-adjusted edgewise brackets (0.022” 0.028” slot, Roth system) were bonded using light cure composite bonding adhesive in inverted mode at the center of the facial surface of clinical crown of all the incisors.
Step III : Distal end of 0.018” NiTi arch wire was annealed and the arch wire was engaged to the bracket slots using steel ligature ties (0.010”). The distal end was cinched back. The set up was then immersed in a hot water bath (50°C) for 15 minutes. It was recovered and stored at room temperature for overnight.
This procedure expressed the built in tip incorporated in the bracket slots and thus leveled the slot in relation to second order bend. This step helped to negate the effect of in built tip of the bracket on the effective arch perimeter. Following day the arch wire was removed.
Step IV : Interdental spaces in the anterior segment were measured using coordinate measuring machine.
Step V : Distal end of a 0.021”´0.027” NiTi arch wire was annealed and the arch wire was engaged to the bracket slots using steel ligature ties (0.010”). The distal end was cinched back. Interdental spaces in the anterior segment were re-measured using coordinate measuring machine to verify and ensure that there was no alteration in the tooth position or interdental spaces during wire engagement.
Step VI : The set up was immersed in a hot water bath (50°C) for 15 minutes. It was recovered and stored at room temperature for overnight. Following day the interdental spaces were measured by coordinate measuring machine.
Step VII : The arch wire was carefully removed. The brackets of all the incisors were removed using a debonding plier. Remnants of composite resin were carefully removed using a scaler. The bracket bases were sandblasted and cleaned.
Step VIII : Brackets were rebonded in standard mode using light cure composite bonding adhesive at the center of clinical crowns of all the incisors and procedures from step III to step V were carried out.
Procedures from step II to step VII were repeated in similar manner using MBT prescription brackets (0.022” ´ 0.028” slot) and measurements were obtained.
Inverting the brackets ensured that the torque value was changed without changing the crown angulation. Thus, the effect of change in crown inclination of maxillary incisors on the effective arch perimeter was measured.
Statistical Analysis
The values were then subjected to statistical analysis for the comparison of the incisor crown angulation and effective arch perimeter; and for the comparison of incisor crown inclination and effective arch length, to determine significant correlation between these parameters. Student’s paired and unpaired t-test, Pearson’s correlation coefficient and descriptive statistical analysis’ (i.e., mean, standard deviation and standard error) were carried out for all the groups in this study.
Results
The mean values of the interdental spaces before and after the expression of total incisor angulation of 100° were 1.98 mm and 1.86 mm with standard deviation of 0.47 mm and 0.45 mm respectively. Findings of the study are tabulated in [Table/Fig-5,6] respectively. The difference between these mean values, as analysed through student’s paired t-test, was significant (p-value=0.001) [Table/Fig-7].
Change in the interdental spaces with varying degree of crown angulation of maxillary incisors.
| Crown Angula-tion | Time of recording spaces in relation to tip expression | Interdental spaces (in mm) |
|---|
| Left lateral and left cuspid | Left lateral and left central | Left central and right central | Right central and right lateral | Right lateral and right cuspid | Total |
|---|
| 0° | - | 0.55 | 0.4 | 0.65 | 0.45 | 0.6 | 2.65 |
| 10° | Before | 0.55 | 0.4 | 0.65 | 0.45 | 0.6 | 2.65 |
| After | 0.493 | 0.366 | 0.649 | 0.412 | 0.545 | 2.465 |
| 20° | Before | 0.492 | 0.367 | 0.648 | 0.413 | 0.546 | 2.466 |
| After | 0.488 | 0.321 | 0.569 | 0.345 | 0.538 | 2.261 |
| 30° | Before | 0.489 | 0.319 | 0.568 | 0.348 | 0.539 | 2.263 |
| After | 0.448 | 0.282 | 0.56 | 0.318 | 0.496 | 2.104 |
| 40° | Before | 0.448 | 0.281 | 0.561 | 0.318 | 0.496 | 2.104 |
| After | 0.44 | 0.253 | 0.452 | 0.289 | 0.494 | 1.928 |
| 50° | Before | 0.44 | 0.252 | 0.454 | 0.288 | 0.494 | 1.928 |
| After | 0.414 | 0.211 | 0.45 | 0.243 | 0.463 | 1.781 |
| 60° | Before | 0.413 | 0.213 | 0.449 | 0.242 | 0.463 | 1.78 |
| After | 0.414 | 0.19 | 0.349 | 0.219 | 0.46 | 1.632 |
| 70° | Before | 0.413 | 0.191 | 0.35 | 0.218 | 0.46 | 1.632 |
| After | 0.401 | 0.153 | 0.349 | 0.18 | 0.451 | 1.534 |
| 80° | Before | 0.402 | 0.154 | 0.348 | 0.18 | 0.451 | 1.535 |
| After | 0.4 | 0.147 | 0.287 | 0.172 | 0.45 | 1.456 |
| 90° | Before | 0.4 | 0.147 | 0.288 | 0.171 | 0.45 | 1.456 |
| After | 0.387 | 0.125 | 0.286 | 0.151 | 0.438 | 1.387 |
| 100° | Before | 0.387 | 0.125 | 0.286 | 0.151 | 0.438 | 1.387 |
| After | 0.386 | 0.111 | 0.239 | 0.135 | 0.438 | 1.309 |
Change in the interdental spaces with varying degree of crown inclination of maxillary incisors.
| Bracket mode | Time of recording spaces in relation to torque expression | Interdental spaces (in mm) |
|---|
| Left lateral and left cuspid | Left lateral and left central | Left central and right central | Right central and right lateral | Right lateral and right cuspid | Total |
|---|
| Roth inverted | Before | 0.5 | 0.35 | 0.45 | 0.385 | 0.4 | 2.085 |
| After | 0.52 | 0.39 | 0.512 | 0.425 | 0.414 | 2.261 |
| Roth standard | Before | 0.52 | 0.39 | 0.512 | 0.425 | 0.413 | 2.26 |
| After | 0.231 | 0.018 | 0.053 | 0.064 | 0.12 | 0.486 |
| MBT inverted | Before | 0.5 | 0.55 | 0.4 | 0.55 | 0.45 | 2.45 |
| After | 0.523 | 0.585 | 0.486 | 0.591 | 0.479 | 2.664 |
| MBT standard | Before | 0.522 | 0.586 | 0.485 | 0.59 | 0.48 | 2.663 |
| After | 0.146 | 0.124 | 0.002 | 0.129 | 0.106 | 0.507 |
Difference in the mean values of interdental spaces before and after. expression of angulation analysed through paired t-test.
| Interdental spaces | Mean | N | Std. Deviation | Std. Error Mean | Mean difference ± SD | t | df | p-value (p<0.05 = significant) |
|---|
| Before expression of angulation | 1.98 | 10 | 0.47 | 0.14 | 0.12 ± 0.05 | 7.43 | 10 | <0.001 Significant |
| After expression of angulation | 1.86 | 10 | 0.45 | 0.13 |
The co-relation between incisor crown angulation and the interdental spaces was negative and statistically significant as indicated by Pearson’s co-relation coefficient r= -0.985 and p-value <0.001 [Table/Fig-8].
Correlation of crown angulation and arch perimeter.
| Variable | Mean | Std. Deviation | N | Correlation ’r’ | p-value (p<0.05 = signif-icant) |
|---|
| Difference | 1.78 | 0.39 | 10 | -0.985 | 0.001 |
Total increase of positive torque by 80° (from -40° to +40°), as achieved through Roth prescription brackets, reduces the interdental space by 1.77 mm and an increase of positive torque by 108° (from -54° to +54°), as achieved through MBT prescription brackets, reduces the interdental space by 2.16 mm [Table/Fig-9].
Change in the interdental spaces with varying degree of crown inclination of maxillary incisors.
| Bracket Prescription | Bracket Mode | Inclination of incisors in degree | Total change in incisior inclination | Mean interdental spaces in mm |
|---|
| Right central incisor (RC), Left central incisor (LC) | Right lateral incisor (RL), Left lateral incisor (LL) | Before expression of Torque | After expression of Torque | Difference |
|---|
| Roth | Inverted | -12° (RC) + -8°(RL)-12° (LC) + -8°(LL) | From -40° to +40° = 80° | 2.26 | 0.48 | 1.77 |
| Standard | + 12° (RC) + +8°(RL)+ 12° (LC) + +8°(LL) |
| MBT | Inverted | -17° (RC) + -10°(RL)-17° (LC) + -10°(LL) | From -54° to +54° = 108° | 2.66 | 0.5 | 2.16 |
| Standard | + 17° (RC) + +10°(RL)+ 17° (LC) + +10°(LL) |
The correlation between the crown inclination and change in the interdental spaces was positive with Pearson’s correlation coefficient ‘r’=1.00. This correlation is statistically significant with p-value<0.001(p<0.05) [Table/Fig-10].
Correlation of crown inclination and arch perimeter.
| Incisor inclination | Change in interdental spaces | Correlation ’r’ | p-value (p<0.05 = significant) |
|---|
| 800 | 1.77 | 1.00 | 0.0001 Significant |
| 1080 | 2.16 |
Discussion
1. Effect of Crown Angulation on the Arch Perimeter
In the present study, increasing the angulation of the maxillary incisors produced a statistically significant reduction in the interdental spaces. The effect of producing a 10o change in angulation in the arch reduced the interdental spaces by an average of 0.12 mm (SD=0.05).
There was a significant negative correlation between the incisor angulation and interdental spaces. Pearson’s correlation coefficient r= -0.985 was observed between the two parameters indicating that, the relation between these two parameters was fairly proportional. This indicates that, a change of 0.012 mm of arch length could be effected by an increase of 1° of incisor angulation.
Studies to quantify the space implication associated with the change in crown angulation have not been reported in the literature. The results of this study were new. The correlation between the two parameters has however been suggested by various researchers [2,4-6].
Hussels W and Nanda RS [4] using a mathematical model, demonstrated that approximately 1 mm of space between two maxillary incisors can be closed by tipping both the central incisors by 3° each [4].
Relation between the crown angulation and arch perimeter observed in the current study were in accordance with Andrews’ contention that, increase in the mesio distal crown angulation requires additional space within the arch [2,3].
The relation between the crown angulation and the arch perimeter obtained in this study were comparable to those of Tuverson DL (1980), who demonstrated that 2 mm of excess space could be absorbed by angulating upright upper incisor [5].
The amount of crown angulation that can be successfully altered, in terms of stability, will be dictated by the nature and the amount of the root divergence of the tooth. Thomas Mulligan (2003) has reported that 90-95% cases of diastema, treated using this concept do not require retention [7].
The amount of crown angulation that can be successfully altered, without compromising aesthetics was studied by Wolfart S et al., (2004). They reported that significant symmetrical angulation of incisors and minor changes in the angulation of one or both lateral incisors are aesthetically acceptable [8].
2. Effect of Crown Inclination the Arch Perimeter
In the present study, it was observed that increase of positive torque by 80° (from-40° to +40°; Roth prescription) reduces the interdental space by 1.77 mm and an increase of positive torque by 108° (from -54° to +54°; MBT prescription) reduces the interdental space by 2.16 mm. This change was statistically highly significant. Pearson’s correlation coefficient shows a perfect positive correlation between the two parameters with ‘r’=1.00.
Results indicated that, increasing labial crown inclination could increase the space consumption within the arch. On the contrary, space can be gained within the arch, by incorporating a lingual crown inclination. The range, up to which the inclination can be altered, will be dictated by the width of the alveolar bone.
The result obtained in the present study was comparable with those obtained in the study carried out by Tuverson DL, O’Higgins ES et al., with the help of a diagnostic set up, showed that as much as 1 mm [5,6]. of additional dental arch length may be gained by increasing the lingual axial inclination of upright maxillary anterior teeth.
Sangcharearna Y and Hob C, showed a negative linear correlation between the incisor inclination and change in the molar relationship, which in turn is indicative of space implication of incisor inclination [9].
Hussels W and Nanda RS, through a mathematical model, showed that the arch length could be affected by incisor inclination [4].
Limitation and Future Prospects
Quantitative results of this study were obtained assuming that complete expression of applied tip and torque was achieved after full slot wire engagement of the brackets using 0.021”0.027” NiTi wire. Considering the fact that stiffer wires of similar dimension are more effective in relation to torque expression, further studies are required to assess the accuracy of this study using stiffer wire in similar set up. Furthermore, in vivo studies are required to gauge the clinical validity and applicability of the same.
Oocclusal forces are dissipated along the long axis of the tooth. Thus, the force dissipation might be redirected with the altered axial positioning of the tooth and in turn will have an impact on the periodontium. Longterm assessment of altered tooth angulation on the periodontal health is therefore needed for its accountability in biological environment.
Considering the variability of the tooth morphology in natural dentition, experimental as well as clinical studies are required to assess the impact of tooth morphology on the space implication. Long-term evaluations of the cases are also needed to determine the clinical liability in terms of retention and stability of the treatment results attempted with this approach.
Conclusion
Andrews realized that attainment of all the six characters of optimum occlusion might not be possible in cases of Bolton’s ratio discrepancy. Although it is not unusual in orthodontic treatment to look for prosthesis, retainers and/or restorative measures to overcome or prevent such situations, orthodontists must not depend entirely on such measures to resolve the problem of instability. Insight of the quantified relation between axial relation of a tooth and the arch perimeter can be useful in such clinical scenarios.
This will also aid in fnishing and detailing of Class II with anterior interocclusal arch length discrepancies as there ia a tendency of spacing between upper anterior teeth or mandibular anterior crowding to occur during the terminal stages of treatment or after the removal of the appliance. In such situation this will help to camouflauge the anterior interocclusal arch length discrepancies (Bolton’s ratio discrepancy) and thereby results in more stable treatment outcome.
Study showed that, with increase in crown angulation and lingual crown inclination, there was an increased consumption of arch perimeter. This increase was found to be linearly proportional. Increase in incisor crown angulation by 1-degree results in consumption of approximately 0.012 mm of arch perimeter. Similarly a consumption of 0.021 mm of arch perimeter was found with an increase of per degree of crown inclination.
Quantifying the space implication of crown angulation and inclination helps to accurately predict the amount of alteration in the axial relation required and can be included in space analysis. Thus, this approach helps the clinician to foresee the treatment out-come, thereby helps in better execution of orthodontic treatment. Results obtained by such an approach are conservative, rapid, predictable, computable and stable.