Chondroid Syringoma: Fine-needle Aspiration Cytology of a Rare Entity at an Unusual Site
Sangeeta Lamba1, Annu Nanda2, Uma Kumar3
1 Senior Specialist and Head, Department of Pathology, ESIC Hospital, Rohini New Delhi, India.
2 Professor, Department of Pathology, ESIC Hospital, Rohini, New Delhi, India.
3 Specialist, Department of Pathology, ESIC Hospital, Rohini, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Uma Kumar, Room No. 128, Department of Pathology, ESIC Hospital, Sector 15, Rohini, New Delhi-110089, India.
E-mail: dr.uma.path@gmail.com
Chondroid syringoma, also known as benign mixed tumour of the skin, is a rare benign adnexal tumour. It is a biphasic tumour, composed of both epithelial and mesenchymal components and constitutes <0.01% of all primary skin tumours. It is mostly located in the head and neck region, followed by the hand, foot, axillary region, abdomen, penis, vulva and scrotum. The arm is a rare site of involvement. Making a correct diagnosis of chondroid syringoma is important to guide the clinician in optimal management. We present a case of chondroid syringoma on the left arm in a 37-year-old male. Fine-needle aspiration was performed and diagnosed as chondroid syringoma, which was confirmed on histopathology. This case highlights the importance of considering chondroid syringoma in the evaluation of subcutaneous swellings of the arm and the role of Fine-Needle Aspiration Cytology (FNAC) in diagnosing this uncommon tumour.
Benign mixed tumor, Cytology, Skin
Case Report
A 37-year-old male presented to the surgical outpatient department with a gradually increasing, painless swelling on the left arm for one year. Local examination revealed a firm, mobile, non-tender, nodular swelling measuring 2.5 cm × 2 cm on the medial aspect of the left arm [Table/Fig-1]. It was not fixed to the underlying structures or to the skin. Clinical diagnosis of epidermal inclusion cyst was considered and the patient was referred for FNAC.
Clinical photograph showing nodular swelling in the left arm.

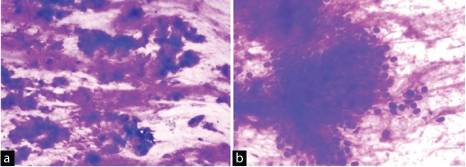
FNAC was performed with the help of 22 G needle mounted on a 10 cc syringe which yielded thick mucoid aspirate. The smears were prepared and stained with Giemsa stain. Microscopic examination showed a biphasic tumour composed of epithelial cells embedded in fibrillary chondromyxoid matrix [Table/Fig-2a, b]. These cells were monomorphic, round to oval, had centrally placed nuclei with fine chromatin and moderate amount of cytoplasm. Based on these cytological findings, a diagnosis of chondroid syringoma was rendered and histopathological confirmation was advised.
(a) Cytological smear showing the chondromyxoid ground substance (Giemsa, 4×); (b) Round-to-oval epithelial cells embedded in the fibrillary matrix (Giemsa, 40×).
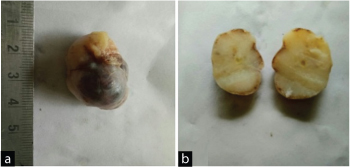
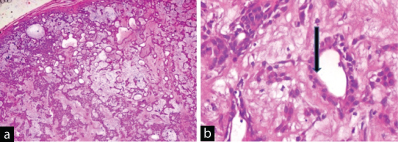
Grossly, the tumour was well encapsulated, firm and nodular measuring 3 cm × 2 cm × 2 cm. Cut section was grayish-white, solid with myxoid areas [Table/Fig-3a, b]. Microscopic examination showed an encapsulated tumour consisting of prominent chondromyxoid stroma enveloping benign bland appearing epithelial cells arranged in tubules, nests, sheets and cords [Table/Fig-4a]. These tubules were lined by outer flattened cells and inner cuboidal cells to polygonal cells, showing apical snouts at places and had round monomorphic nuclei, fine chromatin and inconspicuous nucleoli [Table/Fig-4b]. No necrosis, atypia, or mitotic activity was noted. The histological features were consistent with apocrine variant of chondroid syringoma. On 6-month follow-up, the patient was well with no recurrence.
(a) Gross photograph showing well-encapsulated nodular tumour; (b) cut section is grayish-white solid with myxoid areas.
(a) Section showing encapsulated tumor with cells arranged in sheets, nest and cords and chondromyxoid stroma (H and E, 4×); (b) High-power view showing tubules lined by two types of cells. Luminal cells showing apical snouts (black arrow marked) (H and E, 40×).
Discussion
Chondroid syringoma is a rare benign adnexal tumour, typically located in the head and neck region [1]. It is also known as mixed tumour of the skin and composed of both epithelial and mesenchymal components [2]. It constitutes <0.01% of all primary skin tumours [3].
Hirsch Pand Helwig EB et al. coined the term chondroid syringoma for the tumours with sweat gland-like epithelial components and cartilaginous-like stroma [4]. Chondroid syringoma is thought to originate from both secretory and ductal segments of sweat glands. It usually affects middle-aged or older male patients, clinically presenting as a slow-growing, painless, firm subcutaneous nodule measuring 0.5 cm-3 cm in size [5]. Tumours more than 3 cm in size are described as giant chondroid syringoma [2,3]. Clinically, they can mimic dermoid cyst, sebaceous cyst, neurofibroma, dermatofibroma, pilomatricoma, histiocytoma and nodular fasciitis [4,5]. They are mostly located in the head and neck region, followed by the hand, foot, axillary region, abdomen, penis, vulva and scrotum [6]. A few reported cases of malignant chondroid syringoma are seen to occur on the extremities or trunk with a 2:1 female-to-male ratio [7].
The cytological differential diagnosis includes soft tissue tumours with myxoid background including nodular fasciitis, neurilemmoma, neurofibroma, intramuscular myxoma and low-grade fibromyxoid sarcoma. Other differentials are myoepitheliomas and carcinomas with mucinous stroma [1,5].
FNAC of nodular fasciitis shows single and binucleated cells resembling ganglion cells with marked anisocytosis and anisokaryosis [8]. Cytosmears in neurilemmoma show cells having nuclei with pointed ends and have a buckled or twisted appearance. Intramuscular myxoma on cytology shows an abundant myxoid background with scant cellularity and cells having long cytoplasmic processes, elongated nuclei with occasional muscle giant cells [9]. Aspirates in low-grade fibromyxoid sarcoma show small clusters of spindle cells with mild-to-moderate atypia [10]. Myoepitheliomas of soft tissue are very rare and are indistinguishable from chondroid syringoma on cytology. They are usually located in the deep soft tissues of the extremities [11]. Carcinomas with myxoid stroma can be easily distinguished due to obvious malignant features in epithelial cells and rarely pose a diagnostic difficulty [9,10].
FNAC can suggest a diagnosis of chondroid syringoma on the basis of thick mucoid aspirate. The hallmark of these tumours on cytology is the presence of chondromyxoid matrix with biphasic population of epithelial and myoepithelial cells [12]. It may be misdiagnosed on cytology if the typical biphasic pattern is not seen in smears. Khan K reported a case with extensive cystic change with the presence of epithelial clusters, admixed smaller myoepithelial cells, cystic macrophages and scant chondromyxoid stromal elements [13]. In these cases, histopathology is most reliable in establishing a definitive diagnosis.
Histologically, the tumours contain varying amounts of nests of cuboidal/polygonal cells, tubuloalveolar structures, ductal structures, keratinous cysts and chondromyxoid matrix [3,6]. Headington JT classified these lesions into two types: Apocrine and eccrine. The apocrine type shows irregular branching tubules lined by double-layer epithelium, as seen in this case [6], while eccrine chondroid syringoma is characterized by uniform, small, round tubules lined by single layer of epithelium, which are evenly spaced within a myxoid-chondroid matrix [5,6]. On immunohistochemistry, inner cell layer expresses cytokeratin, carcinoembryonic antigen and epithelial membrane antigen; whereas, the outer cell layer is positive for vimentin, S-100 protein, neuron-specific enolase and occasionally glial fibrillary acidic protein [4,12].
Treatment includes complete excision with wide margins. Incomplete removal and satellite lesions are hypothesized to cause local recurrence. Thus, a regular follow-up is required to monitor for recurrence and malignancy [3,4].
Conclusion
Although the arm is a rare site of involvement, chondroid syringoma should be included in the differential diagnosis of subcutaneous swellings in the arm. Fine-needle aspiration is a simple, easy and cost-effective tool which can be used to diagnose chondroid syringoma and differentiate it from other subcutaneous nodules.
[1]. Dubb M, Michelow P, Cytologic features of chondroid syringoma in fine needle aspiration biopsies: a report of 3 casesActa Cytol 2010 54(2):183-86. [Google Scholar]
[2]. Tokyol C, Aktepe F, Yavas BD, Yildiz H, Aycicek A, Chondroid syringoma: a case reportActa Cytol 2010 54(5 Suppl):973-76. [Google Scholar]
[3]. Kumar B, Chondroid syringoma diagnosed by fine needle aspiration cytologyDiagn Cytopathol 2010 38(1):38-40. [Google Scholar]
[4]. Hirsch P, Helwig EB, Chondroid syringoma: Mixed tumour of skin, salivary gland typeArch Dermatol 1961 84(5):835-47. [Google Scholar]
[5]. Yavuzer R, Basterzi Y, Sari A, Bir F, Sezer C, Chondroid syringoma: a diagnosis more frequent than expectedDermatol Surg 2003 29(2):179-81. [Google Scholar]
[6]. Headington JT, Mixed tumours of skin: eccrine and apocrine typesArch Dermatol 1961 84:989-96. [Google Scholar]
[7]. Malik R, Saxena A, Kamath N, A rare case of malignant chondroid syringoma of scalpIndian Dermatol Online J 2013 4(3):236-38. [Google Scholar]
[8]. Silvanto AM, Melly L, Hannan SA, Kocjan G, FNAC of nodular fasciitis mimicking a pleomorphic adenoma: another diagnostic pitfallCytopathology 2010 21(4):276-77. [Google Scholar]
[9]. Iyer VK, Cytology of soft tissue tumours: benign soft tissue tumours including reactive, nonneoplastic lesionsJ Cytol 2008 25:81-86. [Google Scholar]
[10]. Domanski HA, Mertens F, Panagopoulos I, Akerman M, Low grade fibromyxoid sarcoma is difficult to diagnose by fine needle aspiration cytology: A cytomorphological study of eight casesCytopathology 2009 20(5):304-14. [Google Scholar]
[11]. Moon A, Chin S, Kim HK, Kwak JJ, Myoepithelioma of soft tissue in the knee: A case report of an unusual locationIndian J Pathol Microbiol 2016 59(2):254-56. [Google Scholar]
[12]. Pal S, Sengupta S, Jana S, Bose K, Fine-needle aspiration cytology of chondroid syringoma of fore arm: Report of a rare caseJ Cytol 2014 31(3):171-73. [Google Scholar]
[13]. Khan K, Chondroid syringoma: a case with unusual cytological findingsIndian J Dermatol 2013 58(2):157 [Google Scholar]