Multifocal presentation of a laryngeal disorder is very rare. We report a case of a 48-year-old man, who presented to our hospital with hoarse voice for two years. Stroboscopic evaluation followed by surgery was done and the specimens were sent for histopathological examination from three different anatomical sites of larynx which were diagnosed as one-benign lesion, second-benign lesion but ability of malignant transformation and the third-a malignancy.
Coblation, Histopathology, Malignancy, Papilloma, Polyp
Case Report
A 48-year-old male patient presented to the Department of Otorhinolaryngology with the chief complaints of hoarse voice for two years. There was no associated history of cough, chest pain, dysphagia, odynophagia, hemoptysis, dyspnoea, weight loss, loss of appetite and stridor. He had been a tobacco smoker and alcoholic for 20 years and a known case of Type 2 diabetes mellitus and on regular treatment.
On general examination, the patient’s general condition was good. Clinical systemic examination did not reveal any abnormality in the cardiovascular, respiratory and gastrointestinal system. There were no palpable lymph nodes in the neck.
Indirect laryngoscopic examination revealed a sessile polypoidal mass involving the middle 1/3rd of the right vocal cord, whitish irregular papilliferous growth involving anterior 2/3rd of left vocal cord with bilateral normal vocal cord movements. On stroboscopic examination, a reddish proliferative granular lesion was seen involving the lingual surface, left lateral border and tip of the epiglottis upto the midline in the supraglottic region and a sessile pale polypoidal mass involving the middle 1/3rd of the right vocal cord and irregular chalky white papilliferous excrescences extending from anterior commissure upto the posterior 1/3rd of the left vocal cord was seen in the glottic region [Table/Fig-1].
Stroboscopic picture of multifocal presentation of larynx.
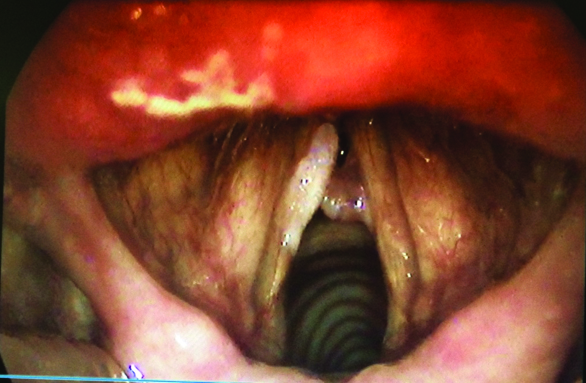
There was complete absence of mucosal wave in the left vocal cord. Right side mucosal wave were restricted at the level of vocal cord polyp with hour glass type of glottic chink and prominent open phase. The amplitude was normal with Type III muscle tension dysphonia.
Examination of the ears and nose with Paranasal Sinuses (PNS) did not reveal any abnormality. All routine blood investigations were normal. Ultrasound neck and CT scan neck were normal. Chest X-ray Posterior Anterior (PA) view showed normal lung fields. Serological test for human immunodeficiency virus and hepatitis B virus was non reactive.
Patient was posted for microlaryngeal surgery under general anaesthesia. The biopsy was taken from the epiglottic lesion and the excision of the right vocal cord polyp and left side vocal cord growth was done. All the three specimens were collected separately and sent for histopathological examination. Specimens were stained with haematoxylin and eosin stain and visualised under 10X and 40X magnification.
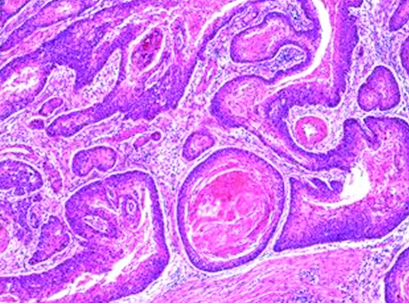
Histopathological examination of three different sites showed well differentiated invasive squamous cell carcinoma in the epiglottis, squamous papilloma in the left vocal cord and benign vocal cord polyp in the right vocal cord [Table/Fig-2,3 and 4].
Well differentiated invasive squamous cell carcinoma in the epiglottis (H&E stain, 10X).
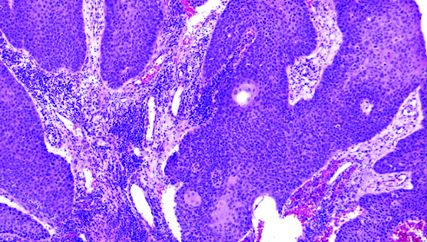
Squamous papilloma in the left vocal cord (H&E stain, 10X).
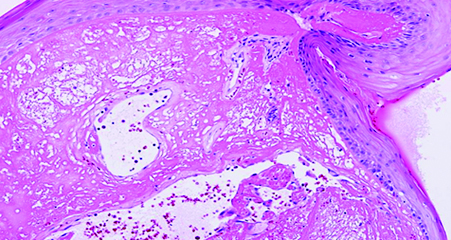
Benign vocal cord polyp in the right vocal cord (H&E stain, 40X).
All the three histopathological reports enlightened that there were three separate pathological entities. Since the malignancy was limited to the epiglottis only (T1N0M0), so the patient was posted for coblation epiglottectomy under general anaesthesia [Table/Fig-5]. Postoperative period was uneventful and the resected specimen was sent for histopathological examination for surgical margin clearance. Anterior surgical margin showed carcinoma in situ changes, while posterior margin was free of any lesion. Patient was called for regular follow up for one year and there was no evidence of any recurrence and the improvement in the hoarseness of voice was noted.
Postoperative picture of partial epiglottectomy using coblation technique.

Discussion
Many pathological lesions in the same anatomical location of the larynx is extremely a rare case and not even a single case has been reported till the recent past. So this constitutes a clinically interesting case.
The incidence of vocal cord polyp has increased in recent years due to unfavourable conditions such as increased industrialisation, smoking, air pollution and voice abuse. The pathogenesis of vocal cord polyp is excessive use of voice and faulty vocal technique, results in vasodilatation followed by stasis, increased capillary permeability and interstitial oedema. This leads to fibrosis and/or degeneration (basophil and/or hyaline) due to evolution of protein rich exudates [1].
Laryngeal papillomas are benign non invasive epithelial tumours, which includes both adult and Juvenile Onset Laryngeal Papillomatosis (JORP) [2,3]. It is commonly seen in males than females and the same was observed in our case which is similar to that reported by most of the authors in Africa Sub-Saharan region [4].
Human papilloma virus infection is the etiological agent of recurrent respiratory papillomatosis [5]. HPV 6 and HPV 11 are the most prevalent HPV types associated with laryngeal papilloma. Laryngeal papillomas shows ‘dysplastic’ features. In other words, the histopathological examination of laryngeal papilloma ranges from slightly atypical, to pre cancerous and very rarely to cancerous lesion. About 3% to 7% of the papilloma lesions undergo malignant transformation into laryngeal cancer. HPV Type 6, 11, 16 and 18 are related to malignant transformation in recurrent respiratory papillomatosis. Type 6 and 11 are considered “lower risk” for the development of cancer whereas Type 16 and 18 are considered “higher risk” [6]. The HPV typing is performed by PCR reaction using type specific primers.
Carbon dioxide laser surgery, cryotherapy, chemotherapy, coblation surgery, antiviral drugs, antiangiogenic therapy etc., are the different methods used to treat laryngeal papilloma. But, still there is a high chance of recurrence seen. The best treatment modality is to remove all visible papillomas, without injuring the normal tissues.
Nowadays, anti HPV vaccines may offer an opportunity to prevent or to treat HPV associated tumours such as cervical, oropharyngeal and possibly laryngeal cancer converting from papilloma. Vaccination induces strong cytotoxic T cell and T helper cell reponses to clear an already established infection [7].
Smoking is the most important risk factor for laryngeal cancer. Death from laryngeal cancer is 20 times more likely for heaviest smokers than for non smokers [8]. Heavy chronic consumption of alcohol is also significant. When combined, these two factors appear to have a synergistic effect.
Laryngeal cancer has characteristic patterns of spread depending on the site of origin. The treatment plan depends on the site, stage (tumour size, nodal spread, distant metastasis) and histological type. The overall health and comorbidities of the patient must also be taken into account.
In our case, patient was a known smoker and alcoholic since 20 years as well as coolie by occupation. Chronic smoking for a long time followed by faulty technique of voice usage may be the possible mechanism that lead to the formation of three pathological lesions in same anatomical location.
The early laryngeal tumours are treated by coblation technique. Coblation is non thermal volumetric tissue removal through molecular dissociation. Coblation devices use a lower voltage Radio Frequency signal (100-350 Volts at 100-500kHz) which is applied through an electrically conductive medium. In the ionised state, vapour layer is formed around the electrode. The low temperature (40° to 90°C) plasma contains radicals which are chemically very active. These radicals chemically disintegrate tissue. This activity is a chemical process with some heat dissipated as a controlled by product allowing control of haemostasis, as opposed to conventional electrocautery, which is a purely thermally driven process [9].
The advantages of coblation are minimal damage to underlying tissue, bloodless field and significantly less risk of airway fire. In our case, since it was an early tumour confined only to the epiglottis, we have done coblation epiglottectomy.
Conclusion
The otorhinolaryngologists should keep in mind that both benign and malignant lesions can coexist in the same individual. So, finest modality technique like stroboscopy has to be included in the routine examination of voice disorder and biopsies from suspicious sites should be taken to confirm the diagnosis and to plan the management.
[1]. Kambic V, Rasdel Z, Zargi M, Acko M, Vocal cord polyps: Incidence, histology and pathogenesisJournal of Laryngology and Otology 1981 95(6):609-18. [Google Scholar]
[2]. Zhou C, Sun B, Wang F, Dai Z, Han Z, Han J, Coblation plus photodynamic therapy for the treatment of juvenile onset laryngeal papillomatosis: Case reportWorld Journal of Surgical oncology 2014 12:275 [Google Scholar]
[3]. Derkay CS, Wiatrak B, Recurrent respiratory papillomatosis: A reviewLaryngoscope 2008 118(7):1236-47. [Google Scholar]
[4]. Timbo SK, Konipo Togola F, Mohamed AA, Keita MA, Sacko HB, Traore L, Laryngeal Papillomatosis in Mali. Apropos of 19 cases collected at the Gabriel TouréHospital of BamakoBull Soc Pathol Exot 2002 95(1):31-33. [Google Scholar]
[5]. Moore CE, Wiatrak BJ, Clatchey KD, Koopmann CF, Thomas GR, Bradford GR, High risk human papillomavirus types and squamous cell carcinoma in patients with respiratory papillomasOtolaryngol Head Neck Surg 1999 120:698-705. [Google Scholar]
[6]. Hobbs CG, Birchall MA, Human papillomavirus infection in the etiology of laryngeal carcinomaCurr Opin Otolaryngol Head Neck Surg 2004 12:88-92. [Google Scholar]
[7]. Brinkman JA, Caffrey AS, Muderspach LI, Roman LD, Kast WM, The impact of anti HPV vaccination on cervical cancer incidence and HPV induced cervical lesions: Consequences for clinical managementEur J Gynaecol Oncol 2005 26:129-42. [Google Scholar]
[8]. Pazdur R, Wagman LD, Camphausen KA, Hoskins WJ, Cancer management: A multidisciplinary approachOncology 2007 11:34-46. [Google Scholar]
[9]. Thiagarajan B, Coblation an overviewOtolaryngology online journal 2014 4:1 [Google Scholar]