Saliva is essential for the preservation, lubrication and maintenance of oral health [1]. Salivary defense rests primarily on its flow rate, pH, buffering capacity, and composition [2,3]. Reduced saliva may affect the oral health which may lead to sequel like dental caries, oral candidiasis, periodontal diseases, and various oral and pharyngeal disorders [2,4,5]. Certain systemic diseases affect secretory function of salivary glands either directly or indirectly which in turn affects the quantity and quality of saliva that is produced [6,7]. Among them, one such disease is thyroid disorder.
Although there are various types of thyroid dysfunctions, autoimmune induced hypo and hyperthyroidism is the most common which affect multiorgan systems in humans. Animal studies revealed thyroid dysfunction affects basal metabolic rate which inturn may affect the secretary unit of salivary gland [8].
Autoimmune thyroid disease is seen mostly in women between the age group of 30-50 years with a prevalence rate of 2 to 4% in women and up to 1% in men [9,10]. There are few studies suggesting significant involvement of salivary glands in cases of AITD, which indicates that there may be a common mechanism in the development of thyroid and salivary gland immune disease [11-14]. To address this need, a study to investigate the salivary gland functioning in patients with AITD was carried out.
Thus the aim of the study was to investigate the salivary glands function quantitatively by collection of unstimulated saliva for evaluating USSFR and qualitatively by estimation of pH, and buffer capacity in autoimmune thyroiditis patients and its comparison with that of the healthy controls.
Materials and Methods
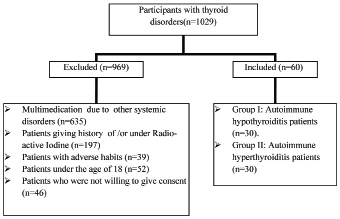
This was a descriptive cross-sectional comparative study conducted using convenience sampling method that screened for the presence of thyroid disorders [Table/Fig-1].
Selection of study participants.
The study protocol was approved by Institutional Ethical Committee and study participants were enrolled from the Government General Hospital, Bangalore, Karnataka and also from private endocrinology clinics. Hospital permission was obtained from directorate of medical education, Ministry of Health and Family Welfare, Karnataka.
All the patients were recruited from outpatient department and screened for presence of thyroid disorders from available records for a period of one year. All were examined (thyroid palpation) by two physicians and one endocrinologist. They were further screened for the presence of autoimmune thyroiditis based on below inclusion criteria for autoimmune hypo and hyperthyroiditis.
Patients with autoimmune thyroiditis (both hypo and hyper thyroiditis patients) with no other systemic illness, aged above 18 years who were willing to give consent, were included in the study. AITD patients were diagnosed based on following criteria [9]:
Autoimmune hypothyroiditis was diagnosed based upon increased serum thyroid stimulating hormone (TSH) > 5 mIU/l, low serum free tetra iodothyroxine (FT4) < 0.61 ng/dl, TPO > 34 IU/ml. Autoimmune hyperthyroiditis: Based on suppressed (TSH) < 0.3 mIU/l, TSH receptor antibody and high FT4 > 2 ng/dl [9].
Patients with any adverse habits like smoking, alcohol consumption, betel and pan chewing, hyperthyroidism undergoing radioactive iodine therapy or under any xerogenic medication that affects salivary secretion or history of any malignancy in the head and neck region etc. were excluded from the study.
Healthy volunteers within the age group of 18-45 years who were age and sex matched, willing to give consent and without any systemic illness and adverse habits were recruited from the hospitals, visiting the outpatient department. The attendees of the study participants were enrolled as control group.
The purpose of the study was explained to the participants and written informed consent was obtained. Later the patients were recalled through telephonic conversation and requested for the participation in the present study. They were scheduled for appointment from 9 to 11 AM and were further instructed to avoid food at least one hour prior to the appointment. The participants were grouped as follows:
Group I: Autoimmune hypothyroiditis (n=30)
Group II: Autoimmune hyperthyroiditis (n=30)
Group III: Healthy volunteers (Controls) (n=30)
Patients were asked to sit in upright position comfortably for five minutes and were given graduated collecting cylindrical tube with the funnel. They were instructed to drool the saliva (as done in drooling method of collection of saliva), into the tube without swallowing for 15 minutes [15]. If there was a time lapse between saliva collection and estimation, it was stored in refrigerator. Saliva was collected at the same time of the day (between 9 and 11 AM) for each patient in order to eliminate confounding, due to diurnal variation.
Collected saliva was subjected to salivary profile estimation, which included USSFR, pH and buffering capacity. USSFR was estimated by drooling method [16] and was expressed as ml/min. The pH was estimated with table top digital pH meter (SUPERFIT Auto Deluxe pH meter, Range 0-14 pH, resolution 0.01 pH, accuracy + 0.01) after standardising each time. Buffer capacity estimation was done by gold standard method according to Ericsson Y method [17], in which final pH>6 were categorised as high buffer capacity, intermediate buffer capacity when the final pH was 4.5-6.5, and low buffer capacity when pH was <4 [17].
Statistical analysis was performed using SPSS version 12. Data was described as mean and standard deviation for continuous variables and as actual numbers and percentages for categorical variables. Comparison of means of more than three groups was performed by ANOVA. Pairwise comparisons were drawn using Tukey post-hoc test. Statistical significance was set at p≤0.05.
Results
After thorough screening of 1029 patient records with thyroid disorder, 969 patients were excluded from the study depending on above exclusion criteria. Rest were categorised into two groups of thirty each, diagnosed as autoimmune hypothyroiditis (n=30) and hyperthyroiditis (n=30) respectively. A total of thirty healthy volunteers who were age and sex matched were included as controls [Table/Fig-1].
[Table/Fig-2]: shows the demographic details of study participants.
Demographic data of the patients
| Groups (n) | Mean age in yrs | Sex |
|---|
| Male (n) | Female (n) |
|---|
| Group I (n=30) | 30.06 | 9 | 21 |
| Group II (n=30) | 31.76 | 14 | 16 |
| Group III (n=30) | 29.7 | 11 | 19 |
Most of the study participants were females (62.22%).
[Table/Fig-3,4] shows the comparison of mean USSFR, pH and buffer capacity among the three groups and pairwise comparisons.
Salivary parameters among groups.
| Category | USSFR (ml/15 min) | pH | Buffer Capacity |
|---|
| Group I | 4.70 + 2.13 | 5.97 + 0.65 | 1.96 + 0.89 |
| Group II | 4.49 + 0.99 | 6.57 + 0.47 | 1.00 + 0.00 |
| Group III | 5.63 + 0.81 | 6.97 + 0.15 | 1.00 + 0.00 |
| p-value | 0.007* | <0.001** | <0.001** |
-Significant,
- Highly Significant, ANOVA test.
Pairwise inter group comparison of salivary parameters.
| Inter group comparison | USSFR | pH | Buffer Capacity |
|---|
| Group I vs Group III | 0.03* | <0.001** | <0.001** |
| Group II vs Group III | 0.008* | 0.005* | 1.00, NS |
| Group I vs Group II | 0.84, NS | <0.001** | <0.001** |
-Significant,
- Highly Significant, NS- Non Significant, Tukey post-hoc test.
The mean USSFR was highest in Group III (5.63+0.81) followed by Group I (4.70+2.13) and Group II (4.49+0.99). This difference was statistically significant (p=0.007). On pairwise comparisons there was no statistical significant difference between Group I and Group II (p=0.84). However, USSFR was significantly decreased in Group I (p=0.03) and Group II (p=0.008) when compared to controls.
The mean pH was highest among Group III (6.97+0.15), followed by Group II (6.57+0.47) and Group I (5.97+0.65) which showed statistically significant difference (p<0.001). However, pH was slightly reduced in Group I (p<0.001) and Group II (p=0.005) which showed statistically significant difference from that of controls.
The buffer capacity was intermediate in Group I. Group II and III showed high buffer capacity which showed no statistically significant difference using pairwise comparison (p=1).
[Table/Fig-5] depicts the distribution of study participants according to sialometric values dispersion.
Sialometric values dispersion among the groups.
| USSFR | pH | Buffer Capacity |
|---|
| Hyposalivation | Reduced Salivation | Normal | <6 | <4.5 | >6 | High | Intermediate | Low |
|---|
| Group I | 1 | 14 | 15 | 15 | 2 | 13 | 12 | 7 | 11 |
| Group II | - | 13 | 17 | 3 | - | 27 | 30 | - | - |
| Group III | | 2 | 28 | - | - | 30 | 30 | - | - |
Discussion
According to Ship JA et al., and Navazesh M et al., the normal USSFR is estimated as 0.3–0.4 ml per minute [15,16]. When USSFR is below 0.1 ml/min, it is considered as objectively hypofunctional [15,16,18], which clearly delineates subjective symptom of reduced salivation. The pH of saliva ranges from 5.3 (low flow) to 7.8 (high flow) [17] and is normally slightly acidic. Most of the salivary secretion volume and electrolyte is contributed by major salivary glands and most of the blood groups substances and lesser secretion volume is contributed by minor salivary glands [18-20].
Hormonal and metabolic changes, as well as altered general health have shown to affect the buffering capacity of saliva and in turn the pH. Thyroid dysfunction is one among the most common endocrine disorders worldwide [10], yet its association with salivary gland function has not been well illustrated in humans. Szanto A et al., have suggested, autoimmune changes that occur in endocrine glands such as thyroid, may also occur in exocrine glands such as the salivary glands, because the process of both is secretion [21].
Early studies in humans assessed the relationship between hypothyroid and salivary gland function using salivary gland scintigraphy [12] and parotid gland flow rates [11,22-24]. In the available literature, assessing salivary gland function using USSFR has not been evaluated in conjunction with AITD and this being the gold standard method to diagnose any systemic disorder affecting salivary gland functioning, it was used in the present study [16,20,25].
Our findings revealed AITD was more common among females which is in accordance with published literature [9,10,23], hence the present study included more of the female participants in the control group.
Dixit PS et al., in their study using both cross-sectional and longitudinal data which showed that hypothyroidism and its treatment did not cause significant decrease in stimulated parotid flow rates [24]. However, their study measured only parotid salivary flow rates instead of USSFR, which perhaps may be more sensitive to hypothyroidism and its treatment. As published literature is not available on the prevalence of hyposalivation among patients with thyroid dysfunction further comparisons were not made. In contrary, our study revealed significant reduction in USSFR among patients with AITD when compared to controls which is in accordance with the study done by Agha-Hosseini F [26]. However, hyposalivation in AITD patients was lower than that of another common endocrine disorder i.e., diabetes [27,28].
Earlier reports using radionuclide scintigraphy have similarly shown that hypothyroidism resulted in poorer salivary gland function [12], which supports our study as there was hyposalivation in patients suffering with hypothyroidism. In our study, a lower USSFR (<0.3 ml/min), salivary pH and lower buffer capacity among hypothyroid subjects was observed, which is in accordance to the study done by Chang CP et al., Muralidharan D et al., [29,30]. In the case report by Markitziu A et al., the lower salivary gland function (0.25 ml/min) among hypothyroid subjects was attributed to parotid gland sialosis induced by chronic hypothyroidism [22]. These all consequences are due to the lower basal metabolic rate, which might be the possible postulated hypothesis from the in vitro study bases [8].
In a new animal study, tyrosylprotein sulfotransferase-2 (Tpst2-/-) knockout mice have salivary hypofunction and smaller salivary gland size due to primary hypothyroidism. After thyroid hormone supplementation, all signs of hypothyroidism (serum T4 and body weight) and salivary gland hypofunction (histological changes and pilocarpine induced salivary flow) were restored to normal or near normal. Their findings indicated that salivary gland hypofunction and low body weight in Tpst2-/- mice was entirely because of primary hypothyroidism [31].
Alterations in the buffering capacity of saliva is one of the most important factors that make the tooth structure prone to caries. Hence, it is essential to maintain the ability of saliva to buffer acids in order to preserve the pH above critical limits to prevent demineralisation of tooth [25,32-34]. Our study revealed only two patients having pH below critical level, who also exhibited poor buffer capacity which is in accordance to the published literature [30].
This suggests the importance of estimation of all the salivary parameters which are critical to maintain the oral health, to be estimated routinely in suspected systemic diseases. As such these patients are under multimedication apart from thyroid, which significantly reduces the salivary flow rate but when all the causes are excluded, the autoimmune thyroiditis itself may pose problem for salivary reduction which may compromise the oral health. A variety of drugs more than 1800 belonging to greater than 80 classes, that have wide range of therapeutic activities have been reported to cause xerostomia, as a side effect [35,36].
To the best of our knowledge only three studies have estimated sialometric analysis in AITD in conjunction with Hashimotos thyroiditis [23,26,29]. Our study is a preliminary one which included both autoimmune hypothyroiditis and hyperthyroidits.
Poor buffering capacity tips the balance toward demineralisation thereby potentially compromising tooth integrity [37]. The present study excluded subjects with history of systemic illnesses, head and neck irradiation or on medication, all of which are known to affect salivary function and could confound the results. However, there is a possibility of presence of undiagnosed systemic illness which may have influenced salivary parameters. Also, being a hospital based study, it is likely that the more severe forms of thyroid dysfunction and also who were under treatment were included and hence the salivary characteristics of subjects with subclinical thyroid dysfunction may not have been considered.
In our study, assessment of saliva was done on patients who were already under treatment, and hence there was only hyposalivation but not to the extent of causing severe xerostomia. However, further studies with large number of autoimmune thyroiditis patients are necessary to confirm our findings.
This study infers the importance of salivary estimation of all the parameters which are critical to maintain the oral health to be estimated routinely in hypothyroid patients.
Conclusion
This study revealed that autoimmune thyroiditis patients have altered metabolism which affects the functioning of the salivary glands resulting hyposalivation especially in autoimmune hypothyroiditis patients. So long follow up of patient may ensure to check any changes occurring, concurrent to the disorder that may cause hyposalivation.
We recommend all AITD patients to use fluoride dentrifrices and for periodic follow up. Future studies should be done to find the exact hypothesis of how thyroid dysfunction can affect salivary gland functioning prior to the treatment and followed by treatment.
*-Significant,
**- Highly Significant, ANOVA test.
*-Significant,
**- Highly Significant, NS- Non Significant, Tukey post-hoc test.