Apple-Peel Intestinal Atresia Along with Isolated Jejunal Duplication Cyst in a Newborn – An Extremely Rare Case Report and Brief Review
Prasanta Kumar Tripathy1, Kaumudee Pattnaik2, Pradip Kumar Jena3, Hiranya Kishor Mohanty4
1 Assistant Professor, Deparment of Paediatric Surgery, SCB Medical College, Cuttack, Odisha, India.
2 Associate Professor, Deparment of Pathology, SCB Medical College, Cuttack, Odisha, India.
3 Professor, Deparment of Paediatric Surgery, SCB Medical College, Cuttack, Odisha, India.
4 Professor, Deparment of Paediatric Surgery, SCB Medical College, Cuttack, Odisha, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Prasanta Kumar Tripathy, Arunodaya Nagar, Link Road, Cuttack-753012, Odisha, India.
E-mail: drpktripathy555@gmail.com
Apple-peel type of intestinal atresia and non-communicating jejunal duplication cyst are rare congenital malformations. The coexistence is not reported in English literature. A five-day-old female neonate having intestinal obstruction and was found to have both the anomalies during laparotomy and was successfully managed. Being an extremely uncommon association between two congenital anomalies of gastrointestinal tract and surgical emergencies, it is reported with review of relevant literature.
Alimentary tract duplications, Intestinal obstruction, Jejunoileal atresia, Mesentric cyst
Case Report
A five-day-old female neonate was brought to emergency for abdominal distension, bilious vomiting and non-passage of meconium. She was born preterm (32 weeks) by spontaneous vaginal delivery at home. Antenatal ultrasonography of mother was not done. At presentation she was 1.8 kg, sick and dehydrated. Abdomen was distended with visible bowel loops, but there was no tenderness or rigidity.
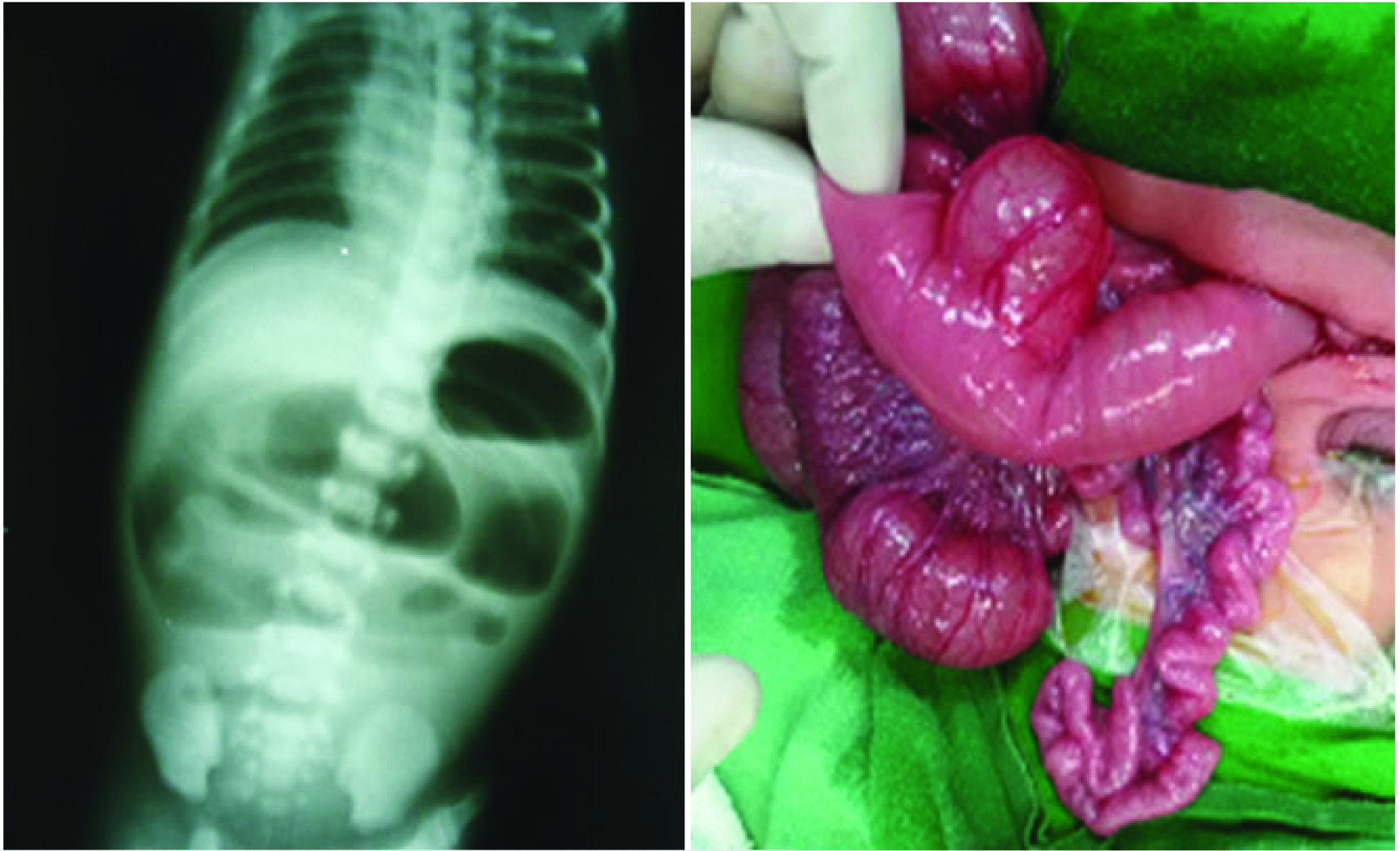
Urgent resuscitation was started with intravenous fluids, oxygen and Nasogastric (NG) tube. NG tube was draining bilious fluids. Erect abdominal x-ray revealed multiple dilated intestinal loops and air-fluid levels [Table/Fig-1a]. After initial stabilization emergency laparotomy was performed. Proximal jejunum was dilated and ending blindly. There was a mesenteric defect followed by type III b (apple-peel) atresia with single arterial supply and significant loss of intestinal length. A fluid-filled cystic lesion measuring 4 cm in diameter was found in the mesentry of proximal jejunum. The lesion was intimately adherent to jejunal wall and sharing common blood supply [Table/Fig-1b]. The duplication appeared to be having all the layers of intestinal wall. Proximal dilated jejunum along with the duplication cyst was excised. The distal atretic small bowel was opened at its proximal end and flushed with warm normal saline to confirm the patency. End-to-back anastomosis was done between proximal jejunum and distal atretic segment of bowel using 5-0 polyglactin sutures in single layer.
(a) Straight x-ray abdomen showing multiple dilated intestinal loops and air-fluid levels; (b) Intraoperative photograph showing apple peel type of intestinal atresia and isolated jejunal duplication cyst.
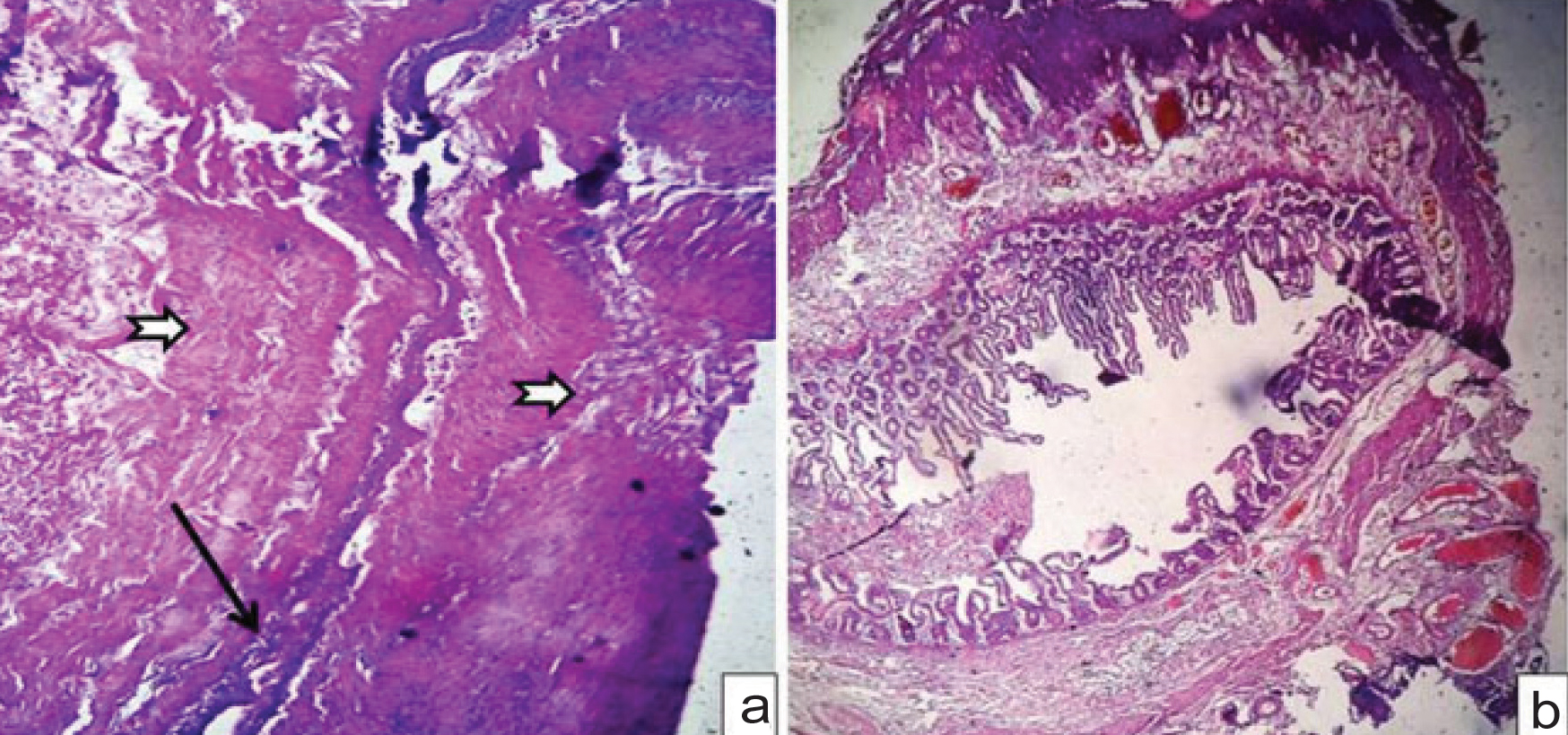
Gross pathology suggested collapsed unilocular cystic structure measuring 4 cm attached to serosal aspect of intestinal wall. The cyst contained mucoid materials and sections were taken from the cyst wall. Microsection revealed normal small intestinal mucosa with flattened villi and the wall showed organized inner circular and outer longitudinal smooth muscle bundles [Table/Fig-2a]. Microsection from distal atretic small intestine showed narrowed lumen with normal villus structure. Submucosa was having loose fibrous tissue with thrombosed and congested blood vessels [Table/Fig-2b]. The newborn had an uneventful postoperative recovery [Table/Fig-3]. Nasogastric tube was removed after the output decreased and became non-bilious. She was discharged on ninth postoperative day with breast feeds. The baby is under intense follow up since last three months with nutritional advice. She is tolerating breast feeds and gaining weight.
Microsection of collapsed duplication cyst shows normal small intestinal mucosa with compressed denuded surface epithelial lining (long black arrow) and the wall shows organized smooth muscle bundles, the muscularis propria (notched white arrows). (H&E, 400X). b) Microsection from distal atretic small intestine showing narrowed lumen with normal villus structure and congested blood vessels (H&E, 100X).
Postoperative image of the neonate.

Discussion
Intestinal obstruction is a common cause of neonatal morbidity and mortality. About one third of these cases are due to intestinal atresia [1]. But, apple-peel or type IIIb Jejuno Ileal Atresia (JIA) is an uncommon variant in Grosfeld classification system [2]. It is also called Christmas-tree or Maypole deformity. There is proximal jejunal atresia followed by large mesenteric defect with significant loss of bowel length. The distal atretic small intestine has a helical appearance around one perfusing vessel in a retrograde fashion. It is associated with a familial pattern and other congenital malformations [3]. This variety of atresia have highest mortality rate (71%) among all types of JIA [4]. Prognosis in JIA has improved in last two decades, but management of apple-peel type is a challenge due to short bowel syndrome.
Alimentary tract duplications are rare congenital malformations that can arise anywhere in gastrointestinal tract, the most common location being ileum [5,6]. They are epithelial-lined structures attached to intestinal wall and supplied by mesenteric vessels [7]. When they do not communicate with intestinal lumen, they are called non-communicating or isolated duplication cyst [5]. Duplication cysts will lead to intestinal obstruction, perforation and there is potentiality for malignant degeneration [6]. Most of them are located on the mesentry of intestine as opposed to Meckel diverticulum, which occur on antimesentric side of bowel. Mesentric cyst is another common differential diagnosis. Histopathologically mesenteric cysts have flattened to cuboidal epithelium without organized muscle coat and absence of nerve plexus, whereas duplication cysts as in our case shows organized muscle coat along with nerve plexus. Excision of duplication cyst along with the native bowel is the standard operative management due to their common blood supply [7].
Half a century back, Favara et al., suggested antenatal vascular accident as aetiological factor for both intestinal atresia and duplication cysts [8]. However, the coexistence is rarely documented [8,9]. Duplication cysts leading to mesenteric volvulus followed by vascular compromise had been proposed in the pathogenesis of intestinal atresia [9]. Apple-peel type of atresia represents a severe form of antenatal vascular accident. The finding of these two rare congenital anomalies of gastrointestinal tract in a newborn with intestinal obstruction prompted us to carry out an extensive search of literature. The association between intestinal atresia and duplication cyst is occasionally reported. However, the association between apple-peel type of atresia and isolated jejunal duplication cyst is not reported in English literature. We suspect intrauterine ischemic insult as aetiological factor for the dual occurrence of congenital malformations in our case.
Conclusion
Apple-peel type of intestinal atresia may coexist with duplication cyst. Non-communicating duplication cysts should be differentiated from mesenteric cysts. Precise surgical technique and postoperative care are essential for salvage of these neonates.
[1]. Subbarayan D, Singh M, Khurana N, Sathish A, Histomorphological Features of Intestinal Atresia and its Clinical CorrelationJ Clin Diagn Res 2015 9(11):EC26-EC29. [Google Scholar]
[2]. Grosfeld JL, Ballantine TVN, Shoemaker R, Operative management of intestinal atresia and stenosis based on pathological findingsJ Pediatr Surg 1979 14:368 [Google Scholar]
[3]. Frischer JS, Azizkhan G, Coran AG, Adzick NS, Krummel TM, Laberge J, Shamberger RC, Caldmone AA, Jejunoileal Atresia and StenosisPediatric Surgery 2012 7th edElsevier Saunders:1059-71. [Google Scholar]
[4]. Prasad TR, Bajpai M, Intestinal atresiaIndian J Pediatr 2000 67:671-78. [Google Scholar]
[5]. Virich G, Grvan D, Merrit N, Giant ileal duplication cyst presenting as malrotationJ Pediatr Surg Case Reports 2013 1:39-41. [Google Scholar]
[6]. Schwartzberg D, Burjonrappa SC, Pseudo Double Bubble:Jejunal duplication mimicking duodenal atresia on prenatal ultrasoundJ Neonat Surg 2013 2(4):42 [Google Scholar]
[7]. Tripathy PK, Jena PK, Mohanty HK, Isolated jejunal duplication cyst associated with intestinal malrotation in a newbornJ Neonat Surg 2016 5:63 [Google Scholar]
[8]. Favara BE, Franciosi RA, Akers DR, Enteric duplications. Thirty seven cases:a vascular theory of pathogenesisAm J Dis Child 1971 122:501-06. [Google Scholar]
[9]. Sinha S, Gangopadhyay AN, Harshwardhan Gopal SC, Ileal atresia with enteric duplicationIndian Pediatr 1992 29:1573-74. [Google Scholar]