Ichthyosis Uteri Associated with Endometrial Adenocarcinoma: A Case Report
Nishu Bhardwaj1, Preeti Diwaker2, Priyanka Gogoi3, Neelam Wadhwa4, Kiran Mishra5
1 Junior Resident, Department of Pathology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi, India.
2 Assistant Professor, Department of Pathology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi, India.
3 Associate Professor, Department of Pathology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi, India.
4 Professor, Department of Pathology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi, India.
5 Ex-Director Professor, Department of Pathology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Preeti Diwaker, 4th Floor, Department of Pathology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Dilshad Garden, Delhi-95, India.
E-mail: diwaker_preeti@yahoo.in
The replacement of the entire or extensive parts of endometrial lining by stratified squamous epithelium is a rare entity known as ichthyosis uteri. It is considered to be a benign condition but may be associated with dysplastic changes and primary squamous cell carcinoma of the endometrium. Its association with endometrial adenocarcinoma is very rare. The aetiology of this condition is not clearly understood till date. We report a case of ichthyosis uteri associated with endometrial adenocarcinoma in a 70-year-old female who presented with complaint of per-vaginal bleeding for six months and underwent hysterectomy after being diagnosed with endometrial carcinoma. Microscopic examination of sections revealed endometrioid adenocarcinoma International Federation of Gynaecology and Obstetrics (FIGO) Grade 3 along with extensive replacement of the endometrial lining by stratified squamous epithelium, consistent with ichthyosis uteri. Although ichthyosis uteri is considered benign and its malignant potential is yet to be established, its association with endometrial malignancies, both squamous and adenocarcinoma, necessitates extensive sampling of the uterus if any focus of squamous metaplasia is identified in a hysterectomy specimen, to rule out a co-existing carcinoma.
Carcinoma, Hysterectomy, Malignant
Case Report
A 70-year-old postmenopausal female, para 5, live 4, presented with complaint of per-vaginal bleeding for six months. Per-vaginal examination revealed an enlarged uterus of 12 weeks gestational size. Ultrasonography showed a heterogenously hyperechoic mass about 6 x 5.2 x 4 cm in size, distending the uterine cavity.
A clinico-radiological diagnosis of endometrial carcinoma was made and endometrial curettage was done for confirmation. Biopsy revealed endometrial adenocarcinoma and the patient underwent a total abdominal hysterectomy with bilateral salpingo-oophorectomy, pelvic and para-aortic lymph node sampling as well as omentectomy. Peroperatively, the uterus was about 12 weeks in size and bilateral ovaries and parametrium appeared normal.
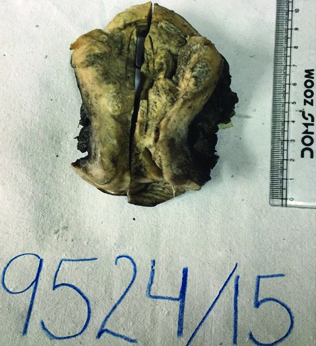
The panhysterectomy specimen sent for histopathological examination measured 10.6 x 7 x 6.5 cm. Cut section revealed a polypoidal friable growth measuring 7 x 6.6 x 4 cm in the uterine cavity arising from the anterior wall of the uterus. Grossly tumour appeared to be invading more than 50% of the myometrium [Table/Fig-1]. The uninvolved endometrial lining appeared atrophic. The cervix as well as bilateral fallopian tubes and ovaries were unremarkable. The 12 sampled regional lymph nodes and omentum were also grossly uninvolved.
Uterus with cervix showing growth present in uterine cavity and invading into myometrium.
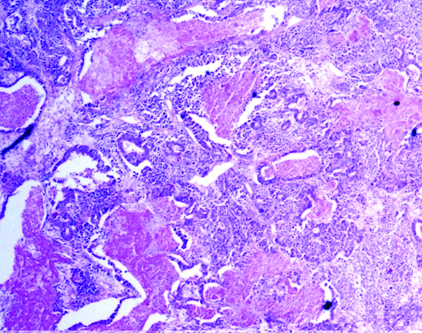
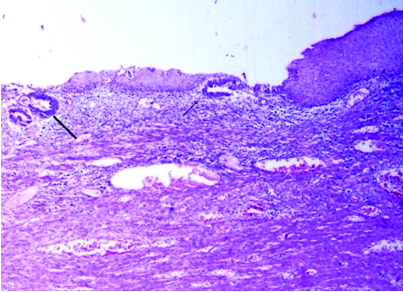
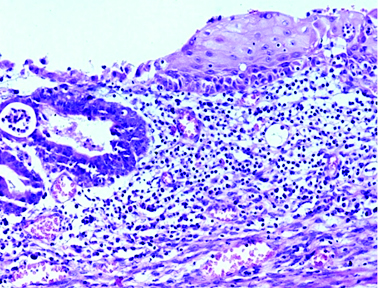
Microscopy of sections from tumour revealed endometrioid adenocarcinoma with confluent areas of necrosis FIGO grade 3 invading more than 50% of the myometrial thickness, with no intermixed areas of squamous differentiation [Table/Fig-2]. Multiple sections from the atrophic endometrium showed stratified squamous epithelium with prominent intercellular bridges and no dysplastic changes. A dense lymphoplasmacytic inflammatory infiltrate was seen in the underlying stroma along with few dysplastic endometrial glands [Table/Fig-3,4]. Few sections from tumour also revealed overlying benign stratified squamous epithelium being destroyed by the endometrioid adenocarcinoma [Table/Fig-5]. The cervical stromal connective tissue was found to be involved. Bilateral ovaries, fallopian tubes and the omentum were free from tumour. No lymphovascular invasion or regional lymph node metastasis was identified. Based on the above findings, a final diagnosis of endometrioid adenocarcinoma (FIGO grade 3), pT2 pN0 pMx with icthyosis uteri was offered. Patient received adjuvant pelvic irradiation after surgery and was followed up for a period of six months which was uneventful.
High grade endometrioid adenocarcinoma with confluent areas of necrosis (H&E 4X).
Extensive replacement of endometrial lining by stratified squamous epithelium (H&E 4X).
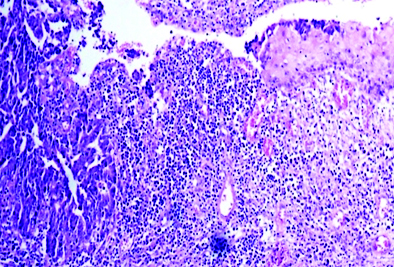
Stratified squamous epithelium replacing endometrial lining with sub-epithelial lymphoplasmacytic inflammatory infiltrate and dysplastic endometrial glands (H&E 20X).
Endometrioid adenocarcinoma destroying the overlying stratified squamous epithelium (H&E 10X).
Discussion
Squamous metaplasia of the endometrium is of two types, typical squamous metaplasia characterized by sheets of cells with obvious squamous differentiation in the form of intercellular bridges and/or keratinisation, and morular squamous metaplasia in which rounded mulberry-like aggregates or syncytial sheets of cells lacking typical features of squamous differentiation are seen occupying glandular lumina [1]. Foci of typical and morular squamous metaplasia are seen in endometrial hyperplasia, endometrial adenocarcinoma and less commonly, in endometritis and endometrial polyps. However, the replacement of extensive parts of endometrial lining by stratified squamous epithelium is a rare entity known as ichthyosis uteri [2]. The term ichthyosis uteri was originally coined by Zeller in 1885, and was used to describe extensive replacement of the endometrial lining by stratified squamous epithelium as a result of iatrogenic introduction of caustic substances such as hot formalin and iodine [3]. Since then, similar changes have been described in response to long-standing inflammatory conditions of the endometrium, such as, tubercular endometritis, hyperplasias and pyometra secondary to malignancies [4]. The aetiology of this rare condition is not clearly understood till date. Various causes like chronic infections, trauma, foreign bodies, estrogen therapy, vitamin A deficiency etc., have been suggested [5]. In the present case, the presence of a dense lymphoplasmacytic infiltrate below the stratified squamous lining suggests the role of chronic inflammation as an aetiological factor for ichthyosis uteri.
Cases with ichthyosis uteri associated with benign pathologies like uterine squamous papilloma and prolapse have been reported, thus suggesting that it is mostly an incidental finding [6,7]. Even though it is a benign condition by itself, ichthyosis of the uterus has been found to be associated with various malignant conditions [8-11]. Bagga PK et al., and Murhekar K et al., reported cases of primary squamous cell carcinoma of the endometrium arising in a background of dysplastic ichthyosis uteri, thus suggesting that this condition may have malignant potential [8,9].
The occurrence of icthyosis uteri with endometrial adenocarcinoma, though rarer, has been reported in literature [5,10]. In the present case, a large part of the endometrium showed involvement by an endometrioid adenocarcinoma with evidence of gland formation, high grade nuclei and large areas of necrosis. The endometrial lining overlying the tumour as well as the adjacent uninvolved endometrium demonstrated extensive replacement by of the surface lining by stratified squamous epithelium. These co-existing findings suggest that the patient had pre-existing ichthyosis uteri, the underlying cause of which might be chronic inflammation, followed by the development of an adenocarcinoma in the underlying endometrial glands. In a case similar to ours, Bewtra C et al., found extensive squamous metaplasia of the endometrial lining with an underlying low-grade adenocarcinoma [10].
Ichthyosis uteri can only be diagnosed incidentally after hysterectomy as there are no presenting complaints generally. Due to the rarity of the condition, its clinical significance is not completely understood so far. Apart from individual case reports, there is insufficient evidence to suggest that ichthyosis uteri alone have intrinsic neoplastic potential [10].
Conclusion
Even though the malignant potential of ichthyosis uteri is yet to be established, its association with several malignancies necessitates extensive sampling of the uterus if a focus of squamous metaplasia is identified in a hysterectomy specimen in order to rule out a co-existing carcinoma.
Conflict of Interest: The authors declare that there is no conflict of interest.
[1]. Kurman RJ, Kurman RJ, TeLinde RW, Ellenson LH, Endometrial carcinomaBlaustein’s Pathology of Female Genital Tract 2002 5th edNew YorkSpringer:542-543. [Google Scholar]
[2]. Patton Wt, Squires GV, Ichthyosis uteri: a case reportAm J Obstet Gynaecol 1962 84:858-60. [Google Scholar]
[3]. Thumma RR, Krishna R, Pidakala P, Dysplastic ichthyosis uteri of endometrium associated with squamous cell carcinoma insitu of cervix- does it have a malignant potentialIOSR-JDMS 2014 13:64-67. [Google Scholar]
[4]. Hendrickson MR, Kempson RL, Surgical pathology of uterine corpusMajor Problems in Pathology 1980 Philadelphia, PaWB Saunders:170-171. [Google Scholar]
[5]. Shi H, Chen X, Zhang S, Zhou C, Ichthyosis uteri complicated by poorly differentiated endometrial adenocarcinoma with squamous differentiationPrzeglad Menopauzalny 2013 6:449-52. [Google Scholar]
[6]. Kükükali T, Ertoy D, Ayhan A, Ichthyosis uteri associated with a uterine squamous papillomaEur J Gynaecol Oncol 1996 17:37-41. [Google Scholar]
[7]. Wahal SP, Mardi K, Ichthyosis uteri: an incidental finding with review of literatureMuller Journal of Medical Science and Research 2014 5:89-90. [Google Scholar]
[8]. Bagga PK, Jaswal TS, Dutta U, Mahajan NC, Primary endometrial squamous cell carcinoma with extensive squamous metaplasia and dysplasiaIndian J Pathol Microbiol 2008 51:267-68. [Google Scholar]
[9]. Murhekar K, Majhi U, Sridevi V, Rajkumar T, Do ichthyosis uteri have malignant potential? A case report of squamous cell carcinoma of endometrium associated with extensive ichthyosis uteriDiagn Pathol 2008 3:4 [Google Scholar]
[10]. Bewtra C, Xie QM, Hunter WJ, Jungensen W, Ichthyosis uteri: a case report and review of literatureArch Pathol Lab Med 2005 129:124-25. [Google Scholar]
[11]. Fadare O, Dysplastic ichthyosis uteri-like changes of the entire endometrium associated with squamous cell carcinoma of the uterine cervixDiagn Pathol 2006 1:8 [Google Scholar]