Introduction
The dimension of oral health has been expanded by adding the concept of well being after WHO broadened the definition of health by the inclusion of social well being. Since then oral health too is considered to contribute to general well being and not mere absence of disease. Daily activities like eating, talking, smiling and creative contributions to society are determinants of an individuals well being. So now it is understood that oral health is integral to general health and well being.
A paradigm shift has happened concerning the concept of health, disease causation and health care delivery in medicine and dentistry. The medical model has been replaced by the socio environmental model of health [1] which assumes the state of health as capability for optimal functioning and social and psychological well being. Consequently, Yewe–Dyer M [2] defined oral health as the state of the mouth and associated structures where disease is contained, future disease is inhibited, the occlusion is sufficient to masticate food and the teeth are of a socially acceptable appearance. Even though this definition is an attempt to incorporate the socio environmental model, a better definition given by Dolan T [3] more closely reflects the new concept. She defined oral health as a comfortable and functional dentition which allows individuals to continue in their desired social role.
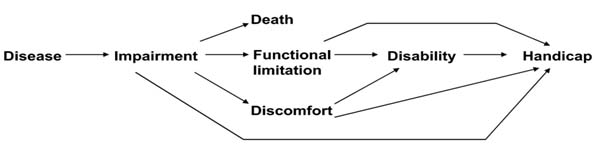
Health, health status, health related quality of life and quality of life have been used interchangeably in literature. David Locker after getting inspiration from WHO ICIDH (International Classification of Impairment, Disability and Handicap) developed a conceptual model for the first time to explain the pathways by which oral diseases and conditions affect quality of life [4] [Table/Fig-1]. According to him concepts of health and quality of life are: 1) difficult to define; 2) multidimensional and complex; 3) predominantly subjective; 4) constantly evolving; and 5) vary according to social, cultural, political and practical contexts. He also added that general health and oral health are inseparable.
Lockers adaptation of WHO ICIDH model – 1988.
It was Cohen LK and Jago JD who reported for the first time, the development of patient based measures for the psychosocial impact of oral health [5]. Development and application of patients self-assessment of oral disease outcomes has grown remarkably over the last two decades. More than 1000 articles are being published annually internationally concerning the patient reported assessment of their oral health and related quality of life. Many studies [6-8] and clinical experience suggest that patient’s perception of the effect of chronic conditions on their life quality differ between people. Some report that their quality of life is good in spite of having physical and functional limitations as a result of chronic disease. This is termed disability paradox and this suggests that health and quality of life are not only conceptually distinct but also empirically distinct [9].
Quality of life in the health scenario (Health related quality of life): The term ‘Quality of life’ (QoL) was first used by the British economist Pigou AC in 1920 [10]. Later, after World War II, this term was expanded into other areas including health. As the concept of health shifted from a biological to a biopsychosocial model [11] clinicians and researchers started recognizing the existence of the quality of life in medicine and dentistry. Now it has become more frequently used term in dental literature in the current century even though initially it was applied mainly in oncology. Quality of life is defined as an individual’s perception of the position in life in the context of culture and value systems in which they live and in relation to their personal goals, expectations, standards and concerns (WHOQoL Group 1995) [12].
The centre for health promotions of the University of Toronto defines quality of life as that concerned with the degree to which a person enjoys the important possibilities of life [13]. Health related quality of life (HRQol) is essentially the subjective perception about the ability to perform those activities important for the individual which is influenced by the current health status [14]. Therefore, assessment of HRQoL should consider the values in which each person lives, the cultural context in which he is immersed, and his expectations and achievements. Also the perception of HRQoL changes with time for the same individual.
Health related quality of life is a trade-off between how long and how well people live [15]. It is strictly a personal attribute and its dimensions change from person to person, from context to context and from culture to culture. At certain aspects, quality of life equates with health status, or in other words poor health means poor quality of life and vice versa. But now it is increasingly recognized that quality of life refers to something much broader than health. The HRQoL assessment in a patient represents the impact that a disease and its subsequent treatment have on the patient’s perception of their well being.
Theoretical basis for health related quality of life: The clinicians and basic research scientists are interested in the biological model of health which has its strong foundations on human biology, biochemistry and physiology. The biological or medical model is empirically testable by means of controlled experiments. The second half of 20th century has seen the emergence of the psycho social concept and the biopsychosocial model of health came into existence. This social science paradigm or quality of life aspect of health and disease focuses on dimensions of functioning, well being and ability of the individual to perform social roles. It cannot be tested by means of clinical experiments since these models of health are founded in psychology, sociology and economics, the methodologies of which are alien to physicians and medical researchers.
For better understanding the phenomenon behind a proposed theory it can be schematically represented by depicting inter-relationships among various concepts. Conceptual model is a schematic representation of proposed aetiological linkages believed to be related to a particular problem or disease [16]. It helps to refine the research question and operationalise the idea.
There are numerous such conceptual models that explain the theory behind the health related quality of life concept [Table/Fig-2]. But none of these models include the entire spectrum of variables that are now regarded in HRQoL assessments and many do not specify the relations that link between biological and QoL measures.
Most popular HRQoL models with respect to oral health related quality of life.
| Year | Conceptual model | Source | Domains | Significance |
|---|
| 1980 | WHO ICIDH [18] | Integration of biomedical and social models into biopsychosocial approach | Six domains Body functions, body structures, activity, participation, environmental factors and personal factors | Basis for all conceptual frameworks of HRQoL |
| 1988 | Locker D [4] | Adapted from WHO ICIDH | Five domains impairment, functional limitation, pain/discomfort, disability, and handicap | Fundamental shift in dentistry from a medical model of care to patient centred perspective |
| 1995 | Wilson and Cleary [17] | Combined biomedical model with social science model | Five main domains biological/physiological, symptom status, functional status, general health and quality of life | Most widely cited HRQoL model |
| 2005 | Ferrans revision of Wilson and Cleary [22] | Revision of Wilson and Cleary model | Five domains of Wilson and Cleary plus further development of individual and environmental factors | Greatest potential to guide HRQoL research and practice |
| 2007 | WHO ICF –CY [24] | Based on WHO ICF model | Same as WHO ICF | Potential as a clinical tool used for measuring HRQoL, needs assessment and intervention research |
Of course many of them have not been tested empirically. A useful model should be relatively simple, intuitively reasonable to clinicians and researchers, and empirically testable [17]. The history of conceptualization of health related quality of life dates back to WHO International Classification of Impairment Disability and Handicap proposed in the year 1980 [18]. In 1988 Locker D adapted the WHO model into the oral health scenario and proposed the first conceptual model for oral health related quality of life [4]. This is regarded as the representation of a fundamental shift in dentistry from a paradigm emphasizing disease and a medical model of care to one that incorporated a patient centered perspective. Locker D in his conceptual model for oral disease has given five sequentially related abstract concepts namely impairment, functional limitation, pain/discomfort, disability and handicap. Structural Equation Modeling (SEM) is a statistical method used to test complex inter-relationships between variables in a proposed conceptual model [19]. Baker SR utilized SEM to empirically test the Locker model and concluded that it represents a generic oral health model with applicability at individual, group and population levels [20].
But the Locker model did not consider individual and environmental factors which are likely to play an integral role in oral health. The most widely used OHRQoL instrument, the Oral Health Impact Profile (OHIP) is based on the Locker’s conceptual model.
Ever since WHO ICIDH model came into being, many models have been proposed by different researchers, The Wilson and Cleary (1995) [17] model seems to be a simple yet comprehensive one. It is a merger between the prevailing biomedical concept and the emerging social concept. Wilson and Cleary model is based on five abstract concepts namely, biological/physiological, symptom status, functional status, general health and quality of life plus mentioning of individual and environmental factors [Table/Fig-3]. Locker D and Quinonez C [21] put forward several reasons to substantiate the comprehensiveness of Wilson and Cleary model, as follows: 1) it identifies the main causal pathway linking biological factors and their functional and psychological outcomes; 2) it makes explicit reference to the quality of life and the variables that have a direct or indirect influence on life quality; and 3) it indicates that quality of life is determined by both medical and nonmedical factors and suggests that personal and environmental characteristics also play a role. Wilson and Cleary model is the most widely tested and applied conceptual model in HRQoL. The other two commonly discussed HRQoL models are Ferrans FE et al., modification of Wilson and Cleary model and WHO International Classification of Functioning and Disability (WHO ICF) [22].
Wilson and Cleary model 1995 [17].
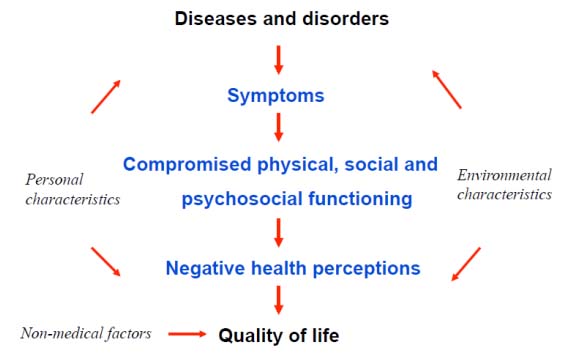
Even though the roles of individual and environmental factors are mentioned by Wilson and Cleary [17], they are not well defined and clearly stated. Ferrans FE [22] revised the model by further development of the individual and environmental factors thus further broadening the concept of Wilson and Cleary. World Health Organisation International Classification of Functioning Disability and Health: Children and Youth version (WHO-ICF-CY) [23] is an integration of medical and social models for a biopsychosocial approach. Although WHO ICF model has been considered a model of HRQoL, it is more regarded as a classification framework which can be used to explain the health of families, communities, populations and cultures rather than a guide to hypothesis generation in HRQoL research [24]. This model has evolved over time from the WHO ICIDH in 1980 and this evolution is based on systematic field trials and international consensus. The latest addition to it is the WHO ICH – CY put forward in the year 2007, which covers infants, children and adolescents.
According to Slade GD et al., the impact on the quality of life in patients with common oral or dental diseases varies from others with similar extent and severity of the clinical condition [25]. According to Wilson and Cleary this difference in quality of life affection within people with comparable clinical disease is due to the mechanisms of adaptation and coping. The personal and environmental variables also play a mediating or moderating role.
Definition of Oral Health Related Quality of Life (OHRQoL): The concept of the broader perspective of health was appreciated by researchers in Medicine as early as 1960s. But the need and scope of the wider horizon of the concept of health and well being with respect to oral conditions was recognized almost a decade later by dental clinicians and researchers. This is partly because dental diseases were not thought to satisfy the classical sick role theory [26] which formed the basis for the development of WHO ICIDH model of health and quality of life.
Although oral health problems are rarely life threatening they remain a major public health problem because of their burden due to high prevalence and it is now widely recognized that oral health can contribute to social, economic and psychological consequences. In other words, oral health can impact an individual’s quality of life. Oral health and the ensuing life quality of the individual is an essential component of general health and well being and hence recognized by the WHO as an important segment of its Global Oral Health Program [27].
The concept of oral health related quality of life is vague. The many definitions of oral health related quality of life proposed by various researchers and groups are proof of this fact [Table/Fig-4] for different definitions of OHRQoL [28-32].
Various definitions of OHRQoL.
| Gift HC and Atchison KA [32] |
| “Self-report specifically pertaining to oral health capturing both the functional, social and psychological impacts of oral disease” |
| Locker D et al., [28] |
| “The extent to which oral disorders affect functioning and psychosocial well being.” |
| NIDCR US Surgeon Generals Report [29] |
| “OHRQoL is a multidimensional construct that reflects (among other things) people’s comfort when eating, sleeping, and engaging in social interaction; their self esteem; and their satisfaction with respect to their oral health.” |
| Locker D et al., [30] |
| “Symptoms and functional and psychosocial impacts that emanate from oral diseases and disorders” |
| Inglehart MR [31] |
| “An individual’s assessment of how the following affect his or her well being: functional factors, psychological factors, social factors and experience of pain/discomfort in relation to orofacial concerns” |
In simpler terms OHRQoL is the impact of oral conditions on daily functioning. But it is too simple an explanation. These definitions suggest that OHRQoL equates with health but at the same time it encompasses dimensions which are broader than health.
Significance of oral health related quality of life: Gift HC and Atchison KA have identified three areas of dental health in which oral health related quality of life has got significance, namely-clinical practice of dentistry, dental research and dental education [32].
OHRQoL is being increasingly recognized in clinical dentistry owing to the understanding that it is the patients who are being treated and not merely their dental or oral condition. This is founded on the recently recognized patient centred biopsychosocial approach to oral health care. Sischo L and Broder HL suggest the following reasons for the growing importance of QoL in clinical dental practice [33]:
1) The patient’s more active role as a member of the treatment team;
2) The need for evidence based approaches in health practices; and
3) The fact that many treatments for chronic diseases fail to cure the health condition.
OHRQoL has demonstrated tremendous potential at all levels of dental research including basic research, clinical trials and in epidemiological survey research. Evidences suggest that periodontal disease can have profound oral health impact and is associated with low OHRQoL [34-37]. Shamrany A reported that since the magnitude of the dental condition can be better expressed in terms of its quality of life impact on the sufferers than by means of normative clinical indices, it is easy to communicate the gravity of the problem to politicians and policy makers [38]. This in turn helps to strategize dental health care programs, institutional priorities, policies, and funding decisions. Oral health related quality of life has been included as an integral aspect of dental health and overall health in many policy documents in the United states like healthy people 2010, US Surgeon General’s report on oral health 2003, CDC burden of oral disease tool for creating state documents 2005, NIDCR strategic plan 2007 etc., [39].
Patient Reported Outcome Measures (PROMs): The US FDA defined PROM as any aspect of a patient’s health status that comes directly from the patient (i.e., without the interpretation of the patient’s responses by a physician or anyone else) and may include reports of disease symptoms, treatment adverse effects, functional status, or overall well being [40]. These self reported health outcomes are being used in intervention clinical trials. HRQoL has to be distinguished from PROM. HRQoL measures are not only patient reported, but also involve the patients subjective assessment or evaluation of important aspects of his or her well being [40]. In other words all HRQoL measures can be called as PROMs but all PROMs are not HRQoLs, especially those with little or no evaluation component.
Oral health related quality of life measures: Now, it is widely recognized that quality of life measures are not a substitute of assessing disease or treatment outcomes but are vital adjuncts to it. In dental literature tools that measure patient’s perspective were originally referred to as socio-dental indicators or measures of oral health status or social impacts of oral diseases [4]. In the late 1990s these terms were replaced by the term OHRQoL. The following words are used to denote quality of life measures interchangeably - scale, profile, tool, inventory and questionnaire.
These measures vary widely in terms of: 1) the format of the items, whether question or statement; 2) format of response, VAS score or likert type; 3) number of items; 4) context of its use; and 5) the population in which it is applied.
Oral health related quality of life tools may be:
1) Socio dental indicators;
2) Global self ratings of oral health;
3) Multiple item questionnaires.
Social indicators assess the effect of oral conditions at the community level. The Social Impacts of Dental Diseases (SIDD) developed by Sheiham A et al., was one of the first socio dental indicators [41]. This type of assessment generally involves carrying out of extensive population surveys to find out the burden of oral conditions on the whole population in terms of certain social indicators such as days of leave from work or job, absence from school, loss of working days due to oral diseases. They are important for planners and policy makers with respect to social or economic perspective.
Global self-ratings are a single item measure which asks a general question regarding the individual’s perception of their overall health status or quality of life at that particular period. The responses will be in a categorical manner ranging from excellent to poor.
Multiple item questionnaires are the more widely used measure of HRQoL. These measures are classified into generic measures and specific measures. Generic measures assess the overall oral health for example, OHIP or OIDP. Specific measures assess specific populations like edentulous or preschool children etc., or specific conditions like dental caries or malocclusion. [Table/Fig-5] shows various OHRQoL measures [42,43]. Ideal qualities of a quality of life [44,45] measure are given in [Table/Fig-6].
Various oral health outcome measures (adapted and modified from Locker and Allen 2007[42] and Hernández J et al., 2015 [43]).
| I.Pre-1997 |
| Social Impacts of Dental Disease (Cushing et al., 1986) |
| General (Geriatric) Oral Health Assessment Index(GOHAI) (Atchison and Dolan 1990) |
| Dental Impact Profile (DIP) (Strauss and Hunt 1993) |
| Oral Health Impact Profile (OHIP) (Slade and Spencer 1994) |
| Oral Impacts on Daily Performances (OIDP) (Adulyanon and Sheiham 1997) |
| Subjective Oral Health Status Indicators (SOHSI) (Locker and Miller 1994) |
| Oral Health-Related Quality of Life Measure (Kressin NR 1997) |
| Dental Impact on Daily Living (DIDLS) (Leao and Sheiham 1997) |
| Oral Health Quality of Life Inventory (John E Cornell et al., 1997) |
| Rand Dental Questions (Dolan T A et al., 1997) |
| OHIP 14 (Slade 1997) |
| II.Post-1997 |
| OHRQoL for Dental Hygiene (Gadbdury- Amyot et al., 1999) |
| Orthognathic QoL Questionnaire (Cunningham et al., 2000) |
| OHIP 14 (Locker and Allen 2002) |
| OHIP Aesthetic (Wong 2007) |
| OHQoL-UK (Mc Grath and Bedi 2001) |
| Child Oral Health Quality of Life Questionnaire (COHQoL) (Jokovic et al., 2002) |
| Parent perception questionnaire |
| Family impact Scale |
| Child perception questionnaire (CPQ 8-10) |
| Child perception questionnaire (CPQ 11-14) |
| Child perception questionnaire (CPQ 11-14) short form |
| Child OIDP (Gherunpong S et al., 2004) |
| Psychosocial Impact of Dental Aesthetic Questionnaire (PIDAQ) (Klages et al., 2006) |
| Child OHIP (Broder 2007) |
| Early Childhood Oral Health Impact Scale (ECOHIS) (Pahel 2007) |
| Surgical Orthodontic Outcome Questionnaire (SOOQ)(Locker D et al., 2007) |
| Prosthetic Quality of life questionnaire (Montero 2011) |
| Scale of Oral Health Outcomes (SOHO) (Tsakos 2012) |
| Quality of life with implant prosthesis (Preciado 2013) |
Ideal qualities of a quality of life measure [46,47].
| Ideal qualities of an OHRQoL Tool |
| 1. Reliability |
| 2. Validity |
| 3. Responsiveness |
| 4. Interpretability |
Criteria for evaluating health related quality of life measures: There are a number of OHRQoL scales now available in the literature, but only a few of them explicitly measures quality of life of the target population. So, it is important to critically analyse these tools regarding their validity and usefulness in assessing the intended measure and to judge the relevance of the evidence it generates.
Any HRQoL measure should be centered on two things: a) it should be patient centered or person centered; and b) it should address aspects of daily life that are important to them which may be affected by the disorder or the condition in question.
There are two different sets of guidelines for evaluating HRQol tools. The Gill TM and Feinstein AR [46] criteria are very stringent and few published and widely accepted tools conform to it. Another guideline which is less demanding is given by Guyatt CD and Cook DJ [47].
Guyatt and Cook (1994) guidelines for evaluating HRQoL measures:
Do the authors show that aspects of patients’ lives they have measured are important to the patients? If not, have previous studies demonstrated their importance?
Do the investigators examine aspects of patients’ lives that clinical experience indicates patient’s value?
Are there aspects of HRQoL that are important to patients that have been omitted?
Were individual patients asked to directly place a value on their lives?
Based on the Guyatt and Cook criteria, Locker and Allen proposed a seven point criteria to evaluate OHRQoL tools [42]. They are;
1) Is the stated aim to measure HRQoL or QoL and is it explicit?
2) If not, is an alternative construct measured by the instrument specified and defined and its consistent domains identified?
3) Was it developed to be used with groups (surveys or trials) or individuals (clinical practice)?
4) Were the items derived from qualitative interviews with those who will be respondents?
5) Is there evidence that the aspects of life the items address are important to the respondents?
6) Does the questionnaire contain global ratings of HRQoL?
7) How was the measure validated? Was it tested against oral health indicators or with indicators that may capture aspects of quality of life?
Oral health related quality of life research in India: Social well being is an integral part of OHRQoL. The social environment of the patients or population studied therefore needs to be considered in defining the content of the quality of life assessment tool. This is particularly significant for a country like India where there is so much of diversity in social, cultural, ethnic, economic and linguistic aspects between various regions. The customs, religious practices and health beliefs vary so are literacy and health awareness. Thus, the tools developed for Western populations or elsewhere could not be utilized to study the quality of life by mere translation into any of the Indian languages. Relevant modifications have to be made in the content and construct of the tool according to the demography in order to assess the subjective perception. As with health science research in general, the importance of OHRQoL is recognized late in India. Published articles on Indian population are comparatively fewer. Hindi is the fourth largest spoken language in the world OHIP has been translated to many Indian languages including Hindi [48,49]. A tool that is found to be reliable and valid in the Hindi speaking population may not be valid in South India. Batra M et al., [49], utilized a translated and validated Hindi version of OHIP 14 in Moradabad adult population (n= 186) in the state of Uttar Pradesh, India. The instrument was found to be reliable and valid with a Cronbach’s alpha of 0-8. Deshpande et al., [48] on the other hand applied the translated Hindi version of OHIP-14 and the original English version simultaneously to 102 participants and assessed the correlation of the responses. But the translational validation process lacks specificity and is not explicitly mentioned. GOHAI has been translated to Hindi [50] and Tamil [51] Bhat SG and Sivaram R developed the Malayalam version of ECOHIS [52]. Kumar S tested the psychometric properties of Telugu versions of CPQ (11-14) [53] and Parental/Caregiver Perception Questionnaire (P CPQ) and Family Impact Scale (FIS) [54]. Mathur VP et al., developed a new tool, Oral Health related Early Childhood Quality of Life (OH – ECQoL) in Hindi to be applied in North Indian pre-school children which was reported to be reliable and valid in that population [55]. [Table/Fig-7] is cited for details regarding studies from India [56-60].
Some OHRQoL studies from India.
| Authors | Instrument | Objective | Population and Sample | Remarks |
|---|
| Kumar S et al., [56] | OHRQoL - Jokovic | Comparison of caries status and OHRQoL between school children living with parents and orphan children | 12-15 years old school children in UdaipurN= 536279 living with parents and 257 orphans | Significant difference with regard to QoL between the groups.Relatively higher caries scores and poor QoL in orphans. |
| Fotedar S et al., [57] | OHIP 14Both English and a Hindi version used in personal interview | To describe the OHRQoL in adults and to assess its relationship with DMFT and CPI indices | Adults attending OPD in a Shimla Dental CollegeN= 351 | OHRQoL is positively correlated with DMFT and CPI scores.Translational validity not done. |
| Ingle NA et al., [58] | OHIP 14Tamil version | To describe OHRQoL of adults and to assess its relationship with DMFT and OHIS | Adults attending OPD in a Chennai Dental CollegeN= 307 | OHIP scores significantly correlated with the clinical indices.Translational validity not done. |
| Sudeep CB et al., [59] | Child –OIDP TsakosAssisted interview | To assess OHRQoL of 12-15 years old residing in orphanages | Children residing in orphanages in Calicut, KeralaN= 252 | Positive correlation between OIDP scores and oral health status. No mentioning about translation of OIDP instrument. |
| Mathur VP etal., [55] | OH ECQoL (Hindi)Newly developed Questionnaire administered to parents | To develop a reliable instrument to measure the OHRQoL of pre school children in North India.To compare between caries and caries free children | North Indian preschool children between 24- 71 monthsN= 300 | Reliable and valid tool for the population.(Cronbachs Alpha 0.86, ICC 0.94)Early childhood caries has significant impact on QoL. |
| Sirisha N R et al., [60] | OHIP 14Telugu version | To assess the impact of socioeconomic status on QoL in a special community | Yenadi tribe of Andhra.N= 156 | High level of oral disease but poor impact on the QoL. Telugu instrument is reliable and valid(Cronbachs Alpha 0.8). |
| Bhat SG and Sivaram R [52] | ECOHIS(The Early Childhood Oral Health Impact Scale) Malayalam version | To develop and validate Malayalam version of ECOHIS | Parents of Malayalam speaking pre school childrenN= 300 | M-ECOHIS can be used to assess OHRQoL of Malayalam speaking school children(Cronbachs Alpha 0.87, ICC 0.94). |
| AppukuttanDP et al., [51] | GOHAI(General Oral Health Assessment Index) Tamil version | To assess the psychometric properties of translated Tamil version of GOHAI | South Indian Tamil speaking adult population between 20-70 attending OPD of a Chennai Dental College N=265 | Tamil version shows acceptable psychometric properties.(Cronbachs Alpha 0.8)PCA analysis extracted four domains with 66.4% variance. |
| Jain R [50] | GOHAIHindi version Self administered | To assess the reliability and validity of the Hindi version | Patients above 55 years attending a Navi Mumbai Dental CollegeN= 420 | Satisfactory psychometric properties(Cronbachs Alpha 0.77). |
| DeshpandeNC et al., [48] | OHIPHindi version. English version also given to the same subjects simultaneously | To validate the Hindi version of OHIP 14 | Patients above 18 years attending a Vadodara Dental CollegeN= 102 | 96.3% correlation between the original English and Translated Hindi versions(Pearsons Correlation Coefficient 0.963) Reliability and validity testing not done. |
| Batra M et al., [49] | OHIP 14Hindi version | To validate the Hindi versionTo assess its psychometric properties in Indian population | Moradabad city population who attended dental screening campsN= 186 | The instrument is reliable and valid with good internal consistency(Cronbachs Alpha 0.8)High correlation between OHIP and OHI-S. |
| Kumar S et al., [53] | CPQ 11-14Telugu version | To assess the reliability and validity of the instrument | Telugu speaking school childrenN= 1342 | The Telugu instrument showed good psychometric properties(Cronbachs Alpha 0.925, ICC 0.923). |
| Kumar S etal., [54] | 1. Family Impact Scale (FIS)2. Parental– Caregiver Perception Questionnaire (P-CPQ) Telugu version | To assess the reliability and validity of FIS and 8 and 16 item P-CPQ | 11-13 years old school children and their parents of TelanganaN= 1342 | Internal consistency and reliability of all the three scales are good.Construct validity of FIS was questionable.Cronbach’s alphaFIS - 0.78, P-CPQ 16-items - 0.83 P-CPQ 8 items - 0.71 |
Conclusion
It is now widely recognized that oral diseases can have varying impacts on people and their well being and life quality. Dental diseases cause pain, discomfort, and affect proper physical functions like chewing, talking and smiling and can influence the individual’s social roles. Results from various clinical and interventional research show that dental treatments and public health interventions can improve OHRQoL. The medical community has recognized the growing importance of the patient reported outcome assessments in clinical practice, public health and research. But much less is being reported in dental literature regarding patient reported outcome assessment. So there is potential in this aspect and in future dental health services research will be focusing on the self reported quality of life as a secondary or even a primary outcome measure in evaluating interventions or community health programmes.
[1]. Nettleton S, The Sociology of health and illness 1995 Cambridgepolity press [Google Scholar]
[2]. Yewe-Dyer M, The definition of oral healthBr Dent J 1993 174:224-25. [Google Scholar]
[3]. Dolan T, Identification of appropriate outcomes for an aging populationSpecial Care in Dentistry 1993 13:35-39. [Google Scholar]
[4]. Locker D, Measuring oral health: A conceptual frame workCommunity Dent Health 1988 5:3-18. [Google Scholar]
[5]. Cohen LK, Jago JD, Towards the formulation of socio dental indicatorsInt J Health Serv 1976 6:681-98. [Google Scholar]
[6]. Nguyen HA, Anderson CA, Miracle CM, Rifkin DE, The association between depression, perceived health status, and quality of life among individuals with chronic kidney disease: an analysis of the national health and nutrition examination survey 2011-2012Nephron 2017 [Google Scholar]
[7]. Pinheiro LC, Tan X, Olshan AF, Wheeler SB, Reeder-Hayes KE, Samuel CA, Examining health-related quality of life patterns in women with breast cancerQual Life Res 2017 :1533-35. [Google Scholar]
[8]. Garvey G, Cunningham J, He VY, Janda M, Baade P, Sabesan S, Health-related quality of life among Indigenous Australians diagnosed with cancerQual Life Res 2016 8:1999-08. [Google Scholar]
[9]. Carr AJ, Higginson IJ, Are quality of life measurespatient centered?Brit Med J 2001 322:1357-60. [Google Scholar]
[10]. Pigou AC, The economics of welfare 1920 LondonMacmillan & Co, Limited [Google Scholar]
[11]. Engel GL, The clinical application of the biopsychosocial modelAm J Psychiatry 1980 137:535-44. [Google Scholar]
[12]. WHOQoL GroupThe World Health Organization quality of life assessment (WHOQoL): Position paper from the World Health OrganizationSoc Sci Med 1995 41:1403-09. [Google Scholar]
[13]. Raphael D, Brown I, Renwick R, Rootman I, Quality of life theory and assessment: what are the implications for health promotionIssues in Health Promotion Series. University of Toronto, Centre for Health Promotion 1994 [Google Scholar]
[14]. Schwartzmann L, Quality Of Life Related To Health: Conceptual AspectsScience. Sick [on-line] 2003 2:9-21. [Google Scholar]
[15]. Gift HC, Atchinson KA, Oral health, health and health related quality of lifeMedical care 1995 33:557-77. [Google Scholar]
[16]. Earp JA, Ennett ST, Conceptual models for health education research and practiceHealth Education Research: Theory and Practice 1991 6:163-71. [Google Scholar]
[17]. Wilson I, Cleary PD, Linking clinical variables with health related quality of life;a conceptual model of patient outcomesJAMA 1995 273:59-65. [Google Scholar]
[18]. WHO International Classification of Impairments Disabilities and HandicapsA manual of classification related to the consequence of disease 1980 GenevaWHO [Google Scholar]
[19]. Kline RB, Principles and practice of structural equation modeling 2005 2nd edNew YorkThe Guildford press [Google Scholar]
[20]. Baker SR, Testing a conceptual model of oral health: a structural equation modeling approachJournal of Dental Research 2007 86:708-12. [Google Scholar]
[21]. Locker D, Quinonez C, To what extend do oral disorders compromise the quality of life?Community Dent Oral Epidemiol 2011 39:3-11. [Google Scholar]
[22]. Ferrans CE, Zerwic JJ, Wilbur JE, Larson JL, Conceptual model of health related quality of lifeJ Nurs Scholarsh 2005 37:336-34. [Google Scholar]
[23]. International Classification of FunctioningDisability and Health: Children and Youth version 2007 GenevaWHO [Google Scholar]
[24]. Bakas T, McLennon SM, Carpenter JS, Buelow JM, Otte JL, Hanna KM, Systematic review of health related quality of life modelsHealth and Quality of life Outcomes 2012 10:134 [Google Scholar]
[25]. Slade GD, Nuttall N, Saunders AR, Steele JG, Allen PF, Lahti S, Impacts of oral disorders in the United Kingdom and AustraliaBrit Dent J 2005 198:489-93. [Google Scholar]
[26]. Varul MZ, Talcott Parsons, the sick role and chronic illnessBody & Society 2010 16:72-94. [Google Scholar]
[27]. The World Oral Health Report 2003Continuous improvement of oral health in the 21st Century: the approach of the WHO Global Oral Health Programme 2003 Geneva, SwitzerlandWHO [Google Scholar]
[28]. Locker D, Clarke M, Payne B, Self-perceived oral health status, psychological well-being and life satisfaction in an older adult populationJ Dent Res 2000 79:970-75. [Google Scholar]
[29]. Oral health in AmericasReport of the US Surgeon general. National Institute of Dental and Craniofacial Research 2000 National Institute of Health [Google Scholar]
[30]. Locker D, Matear D, Stephens M, Jokovic A, Oral health-related quality of life of a population of medically compromised elderly peopleCommunity Dent Health 2002 19:90-97. [Google Scholar]
[31]. Inglehart MR, Bagramian RA, Oral health related quality of life: an introduction 2011 ChicagoQuintessence Publishing:1-6. [Google Scholar]
[32]. Gift HC, Atchison KA, Dayton CM, Conceptualizing oral health and oral health related quality of healthSocial Science & Medicine 1997 44(5):601-08. [Google Scholar]
[33]. Sischo L, Broder HL, Oral health related quality of life: what, why, how, and the future implicationsJ Dent Res 2011 90:1264-70. [Google Scholar]
[34]. Ng SKS, Leung WK, Oral health related quality of life and periodontal statusCommunity Dentistry and Oral epidemiol 2006 34:114-22. [Google Scholar]
[35]. Needleman I, Mcgrath C, Floyd P, Biddle A, Impact of oral health on the life quality of periodontal patientsJ Clin Periodontol 2004 31:454-57. [Google Scholar]
[36]. Cunha-Cruz J, Hujoel PP, Kressin NR, Oral health related quality of life of periodontal patientsJ Periodont Res 2007 42:169-76. [Google Scholar]
[37]. Jansson H, Wahlin A, Johansson V, Akerman S, Lundegren N, Isberg PJ, Impact of periodontal disease experience on oral health relatedquality of lifeJ Periodontol 2014 85:438-45. [Google Scholar]
[38]. Shamrany A, Oral health related Quality of life: a broader perspectiveEastern Mediterranean Health Journal 2006 12:894-901. [Google Scholar]
[39]. Rozier RG, Pahel BT, Patient and population reported outcomes in public health dentistry: Oral health related quality of lifeDent Clin N Am 2008 52:345-65. [Google Scholar]
[40]. Lipscomb J, Gotay CC, Snyder C, Lipscomb J, Gotay CC, Snyder C, Introduction to outcomes assessment in cancerOutcomes assessment in cancer;measures, methods, and applications 2005 CambridgeUniversity Press:1-lp14. [Google Scholar]
[41]. Sheiham A, Maizals J, Maizels A, New composite indicators of dental healthCommunity Dental Health 1987 4:407-14. [Google Scholar]
[42]. Locker D, Allen F, What do measures of ‘oral health-related quality of life’ measure?Community Dent Oral Epidemiol 2007 35:401-11. [Google Scholar]
[43]. Hernández J, Díaz FC, Vilchis MC, Mandeep Singh Virdi, Oral health related quality of lifeEmerging trends in Oral health sciences and Dentitsry 2015 Intech Publishers:691-715. [Google Scholar]
[44]. Streiner DL, Norman GR, Cairney J, Health measurement scales: a practical guide to their development and use 2015 5th edOxford University press [Google Scholar]
[45]. Guyatt GH, Feeny DH, Patrick DL, Measuring health related quality of lifeAnn Intern Med 1993 118:622-29. [Google Scholar]
[46]. Gill TM, Feinstein AR, A critical appraisal of the appraisal of the quality of quality of life measurementsJAMA 1994 272:619-26. [Google Scholar]
[47]. Guyatt GD, Cook DJ, Health status, quality of life and the individualJAMA 1994 272:630-31. [Google Scholar]
[48]. Deshpande NC, Nawathe AA, Translation and validation of Hindi version of Oral Health Impact Profile 14J Indian Soc Periodontol 2015 19:208-10. [Google Scholar]
[49]. Batra M, Aggarwal VP, Shah AF, Gupta M, Validation of Hindi version of Oral Health Impact Proflie 14 for adultsJ Indian Assoc Public Health Dent 2015 13:469-74. [Google Scholar]
[50]. Jain R, Dupare R, Chitguppi R, Basavaraj P, Assessment of validity and reliability of Hindi version of Geriatric Oral Health Assessment Index (GOHAI) in Indian populationIndian J Public Health 2015 59:272-78. [Google Scholar]
[51]. Appukuttan DP, Vinayagavel M, Balasundaram A, Damodaran LK, Shivaraman P, Gunasshegaran K, Linguistic adaptation and psychometric properties of tamil version of general oral health assessment index-TmlAnn Med Health Sci Res 2015 5:413-22. [Google Scholar]
[52]. Bhat SG, Sivaram R, Psychometric properties of the Malayalam version of ECOHISJ Indian Soc Pedod Prev Dent 2015 33:234-38. [Google Scholar]
[53]. Kumar S, Kroon J, Lalloo R, Johnson NW, Psychometric properties of translation of the child perception questionnaire (CPQ11-14) in Telugu speaking Indian childrenPLos One 2016 11:3 [Google Scholar]
[54]. Kumar S, Kroon J, Lalloo R, Johnson NW, Validity and reliability of short forms of parental-caregiver perception and family impact scale in a Telugu speaking population of IndiaHealth Qual Life Outcomes 2016 14:34 [Google Scholar]
[55]. Mathur VP, Dhillon JK, Logani A, Agarwal R, Development and validation of oral health-related early childhood quality of life tool for North Indian preschool childrenIndian J Dent Res 2014 25:559-66. [Google Scholar]
[56]. Kumar S, Goyal A, Tadakamadla J, Tibdewal H, Duraiswamy P, Kulkarni S, Oral health related quality of life among children with parentsand those with no parentsCommunity Dental Health 2011 28:227-31. [Google Scholar]
[57]. Fotedar S, Sharma KR, Fotedar V, Bhardwaj V, Chauhan A, Manchanda K, Relationship between oral health status and oral health related quality of life in adults attending HP Government Dental College, Shimla, Himachal Pradesh-IndiaOHDM 2014 13:661-65. [Google Scholar]
[58]. Ingle NA, Chaly PE, Zohara CK, Oral health related quality of life in adult population attending the outpatient department of a hospital in Chennai, IndiaJ Int Oral Health 2010 2:45-56. [Google Scholar]
[59]. Sudeep CB, Sequeira PS, Jain J, Oral health related quality of life among12-15-year-old children residing at orphanages in south India- a descriptive studyBritish Journal of Research 2014 2:53-62. [Google Scholar]
[60]. Sirisha NR, Srinivas P, Suresh S, Devaki T, Srinivas R, Simha BV, Oral health related quality of life among special community adult population with low socioeconomic status residing in Guntur city, Andhra Pradesh: A cross-sectional studyJ Indian Assoc Public Health Dent 2014 12:302-05. [Google Scholar]