Intraosseous Epidermal Inclusion Cyst of the Great Toe: Masquerading as Bone Tumour
Uma Kumar1, Sangeeta Lamba2
1 Specialist, Department of Pathology, ESIC Hospital, Rohini, New Delhi, India.
2 Senior Specialist and Head, Department of Pathology, ESIC Hospital, Rohini, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Uma Kumar, Specialist, Department of Pathology, Room no 128, ESI Hospital, Sector-15, Rohini, Delhi-110089, India.
E-mail: dr.uma.path@gmail.com
Cytology, Intraosseous, Nail avulsion
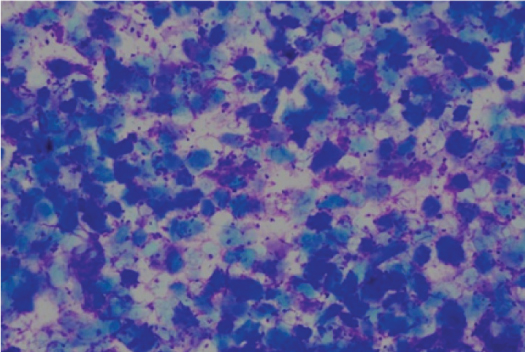
A 54-year-old male, a motor mechanic by occupation, presented to the orthopaedics clinic with two months history of painful enlargement of the left great toe [Table/Fig-1]. The swelling was slowly increasing in size. His past history revealed a road accident four years back, which caused injury to the same toe, however there was no fracture at that time. It got healed without any other consequences. After six months of this accident, an iron rod fell on the same toe which caused avulsion of his nail, for which he took treatment from a local doctor and a bandage was applied. The nail had regrown normally and he did not have any symptoms, until two months back, when he started having pain and swelling on the same toe. There was no significant medical history. On physical examination, left toe was enlarged as compared to the right toe. Overlying skin and nail were discoloured. No other swelling or lymphadenopathy was noted. Blood investigations were within normal limits. X-Ray showed a radiolucent lesion with lytic areas in distal phalanx of the left great toe [Table/Fig-2]. Clinically, a giant cell tumour of bone was suspected and Fine Needle Aspiration Cytology (FNAC) was advised to confirm the diagnosis. FNAC was performed with a 23 gauge needle attached with a 10 ml syringe which yielded 0.1 ml white pultaceous material. Smears were prepared and stained with Giemsa stain. Microscopic examination revealed numerous anucleated squames and few nucleated squamous cells in the background of granular debris [Table/Fig-3]. A diagnosis of intraosseous Epidermal Inclusion Cyst (EIC) was rendered on cytology.
Left great toe showing enlargement at the level of distal phalanx.

X-Ray film showing radiolucent lesion with lytic area (red arrow marked).

Cytology smear showing anucleated squames and few squamous cells (Giemsa 10X).
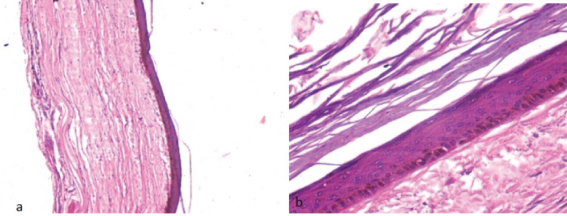
Curettage of the cyst was performed. We received multiple tissue bits measuring 1 cm3 collectively. Haematoxylin and Eosin (H&E) stained section showed a cyst wall lined by keratinised stratified squamous epithelium with prominent granular layer [Table/Fig-4a,b]. No skin appendages seen. The final diagnosis of EIC was made on histopathology. Healing was uneventful and patient was able to perform his duties after three months of surgery. The patient was kept on anti-inflammatory and antibiotic drugs till the next follow up visit.
a) Section showing cyst wall lined by keratinizing stratified squamous epithelium (H&E 10X); b) Higher magnification showing prominent granular layer (H&E 40X).
EIC are commonly seen in subcutaneous tissue, but intraosseous EIC is a rare benign lesion [1]. Skull is the most common site with predominantly parietal and temporal bone involvement. Finger phalanges are the second most common site of predilection followed by maxilla, mandible, temporomandibular joint, vertebrae, tibia and femur [2]. Toe is a rare site of involvement and to our knowledge only four cases have been documented in English literature [3]. Most common age of presentation is 25 -50 years. Men are more commonly affected than women [2,3]. In most of the cases there is a past history of trauma, similar to our case. It is hypothesized that there is a traumatic implantation of epidermal fragments into the bone or due to the migration of a fragment of nail bed into the phalangeal bone [1,4]. Iatrogenic implantation is also suggested in few studies [4,5]. Radiologically, there is a well defined, expanding radiolucent intraosseous lesion. They present as a lytic lesion and can mimic bony tumours radiologically and clinically [1,2]. Differential diagnoses of radiolucent lesion of phalanx includes chronic infections, chondroma, simple bone cyst, aneurysmal bone cyst, intraosseous ganglion, osteoid osteoma, giant cell tumour, giant cell reparative lesion and metastatic lesions [3].
Fine needle aspiration of epidermal inclusion cyst shows predominantly anucleated squames and few nucleated squamous cells. If there is superimposed infection then there is predominantly neutrophils, few macrophages, anucleated squames, nucleated squamous cells and occasional multinucleated giant cell [5]. On histopathology, the cyst is lined by keratinizing stratified squamous epithelium with presence of granular cell layer. This has to be differentiated with dermoid cyst which is also lined by keratinizing stratified squamous epithelium and contain one or more skin appendages [3,4].
Treatment of choice is bone curettage with or without bone graft. Recurrence can occur if there is incomplete excision [1-3]. To conclude, fine needle aspiration can be used for making a correct preoperative diagnosis and unnecessary surgery can be avoided. Although intraosseous EIC are extremely rare in the great toe, they should be considered in the differential diagnosis of radiolucent lesions at this site.
[1]. Ruchelsman DE, Laino DK, Chhor KS, Steiner GC, Kenan S, Digital intraosseous epidermoid inclusion cyst of the distal phalanxJ Hand Microsurg 2010 2(1):24-27. [Google Scholar]
[2]. Hamad AT, Kumar A, Kumar CA, Intraosseous epidermoid cyst of the finger phalanx: a case reportJ Orth Surg 2006 14(3):340-42. [Google Scholar]
[3]. Wang YB, Eisler J, Springfield D, Klien JM, Intraosseous epidermoid inclusion cyst in a great toe-A case report and review of literatureArch Pathol Lab Med 2003 127:e298-e300. [Google Scholar]
[4]. Ertem SY, Uckan S, Ozdemir H, An unusual presentation of an intraosseous epidermoid cyst of the anterior maxilla: a case reportJ Med Case Report 2014 8:262 [Google Scholar]
[5]. Handa U, Kumar S, Mohan H, Aspiration cytology of epidermoid cyst of terminal phalanxDiagn Cytopathol 2002 26:266-67. [Google Scholar]