Aneurysmal Variant of Fibrous Histiocytoma- A Rare Entity Known for Recurrence
Aniya Antony1, Chokka Mahesh Kiran2, Manjiri Phansalkar3, Chidambara Jothi4, Jacob Jayakar5
1 Post Graduate, Department of Pathology, Pondicherry Institute of Medical Sciences, Pondicherry University, Puducherry, India.
2 Associate Professor, Department of Pathology, Pondicherry Institute of Medical Sciences, Pondicherry University, Puducherry, India.
3 Professor, Department of Pathology, Pondicherry Institute of Medical Sciences, Pondicherry University, Puducherry, India.
4 Associate Professor, Department of General Surgery, Pondicherry Institute of Medical Sciences, Pondicherry University, Puducherry, India.
5 Associate Professor, Department of General Surgery, Pondicherry Institute of Medical Sciences, Pondicherry University, Puducherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Aniya Antony, Department of Pathology Pondicherry Institute of medical sciences, Ganapathichettikulam, Kalapet, Puducherry-605014, India.
E-mail: aniya.antony@gmail.com
Aneurysmal Fibrous Histiocytoma (AFH) is a distinct and a rare clinicopathological variant of Cutaneous Fibrous Histiocytoma (CFH). It differs from the usual benign fibrous histiocytoma clinically and morphologically with high rate of recurrence. Here, we report a case of AFH with history of recurrence which presented as a polypoid swelling and showed vascular spaces with no endothelial lining which was proved negative by CD34 immunostaining. The spaces were bordered by tumour cells.
Cutaneous fibrous histiocytoma, Dermatofibroma, Soft tissue neoplasm
Case Report
A 65-year-old man had a history of slow growing nodular swelling on the medial aspect of mid one third of the right leg around 35 years back. He sustained a minor trauma to the swelling and then he got the swelling excised for which skin grafting was done. No records are available of the nature of the swelling. After five years he developed a polypoid swelling at the same site which gradually increased in size for the past 15 years to reach the present size. This swelling got ulcerated 10 days prior to surgery following which excision was done. The gross examination of the excised lesion revealed a skin covered tissue measuring 6.5 x 4.5 x 0.6 cm with a central raised nodular polypoid lesion measuring 3 x 3 x 2 cm. There was ulceration of the overlying skin. Cut section of nodular lesion was dark brown with focal areas of haemorrhage [Table/Fig-1].

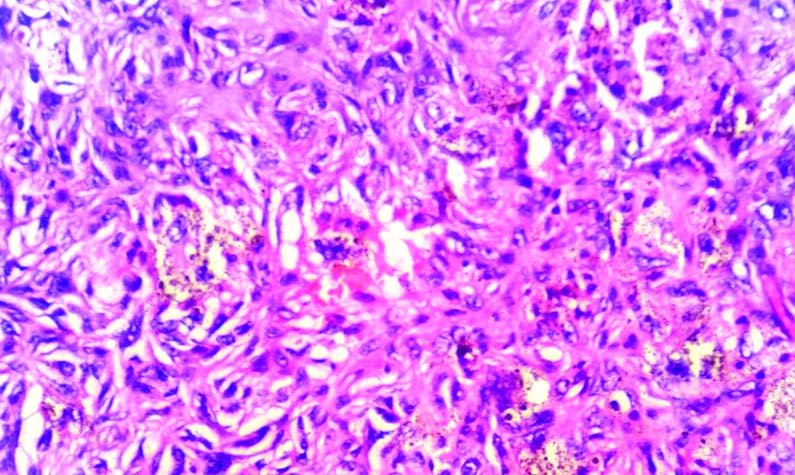
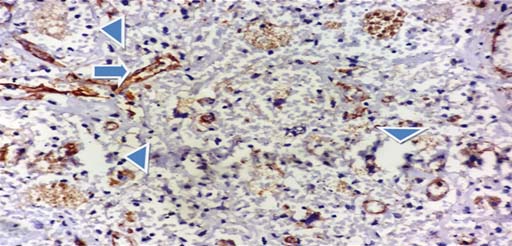
On microscopy, a circumscribed tumour was seen in the deep dermis. The central portion of the tumour showed extensive lakes of haemorrhages along with haemosiderin laden macrophages and necrotic blood vessels. Epidermis overlying haemorrhagic portion was ulcerated while surrounding epidermis showed hyperplasia. The viable tumour tissue around the haemorrhagic centre was composed of many small and cavernous pseudovascular spaces lined by spindly tumour cells in storiform pattern admixed with foamy cells, haemosiderin laden mono and multinucleated cells [Table/Fig-2,3]. The tumour cells were large with vesicular nuclei and some showed prominent nucleoli. However, mitosis was very sparse. Dense haemosiderin deposition was confirmed on Perl’s stain. Immunohistochemistry for CD34 showed negative staining for the cells surrounding the vascular spaces ruling out the possibility of endothelial cells [Table/Fig-4]. Hence a final diagnosis of AFH was given.
Cavernous vascular spaces surrounded by tumour cells (H&E; 4X) Inset: Spindle cells with storiform pattern (H&E; 10X).

Small vascular space surrounded by tumour cells (H&E; 40X).
CD34 IHC staining. Arrow - Blood vessel lined by CD34 positive cells. Arrow head – Spaces lined by tumor cells negative for CD34.(40X)
Postoperative period was uneventful and patient recovered completely. No evidence of recurrence till date, which is two years after excision.
Discussion
AFH is one of the rarest variants of cutaneous fibrous histiocytoma with reported incidence of 1.7% of all CFH [1]. Clinically, AFH presents as a solitary polypoid, blue to brown cystic lesion most commonly on the extremities of young to middle aged adults [2]. The nodule may be associated with rapid growth due to sudden haemorrhage within the lesion leading to suspicion of malignancy and may be associated with pain. High rate of recurrence also adds to the suspicion. The present case also showed rapid increase in size and a history of recurrence raising a clinical suspicion of malignancy.
Microscopically, AFH lesions are located entirely within the dermis. They are highly cellular lesions composed of fibroblastic and histiocytic cells arranged in a storiform pattern. All AFH lesions contained blood filled spaces that vary from narrow slit-like cracks to large cavernous channels [1,3,4]. These spaces are not lined by endothelial cells but are lined and surrounded by fibroblasts and histiocytes. Multinucleated giant cells, foamy cells and haemosiderin-laden macrophages are often seen at the margin of the lesion. Any atypia noted in AFH, can raise the doubt of malignancy. All these features were noted in the present case.
A brief review of literature for AFH is presented [Table/Fig-5] [1-3,5-7]. Most of the cases showed rapid increase in size or a history of recurrence, however histologically all are almost similar and characterized by vascular spaces devoid of endothelial lining.
Aneurysmal fibrous histiocytoma -A brief review of literature.
| Author, Year, Reference | Age (years) /gender | Presentation | Gross Appearance | Microscopy |
|---|
| Bal A et al., 2006 [1] | 22/Male | Nodular swelling on right thigh for six months with rapid increase in size. | Skin covered pigmented nodular growth measuring 4.5 x 2 x 1.5 cm. c/s- grey brown to tan in appearance. | Hyperplastic epidermis focally ulcerated. Tumour spindle shaped, arranged in short fascicles and storiform pattern. Cleft like and large blood filled cavernous spaces without any endothelial lining. |
| Mckenna DB et al., 1999 [2] | 91/Female | Asymptomatic nodule on dorsum of left foot. Bled spontaneously. | 8 mm, blue-black nodule with surrounding induration. | Tumour was composed of large blood filled ecstatic vascular spaces that were lined by angulated spindle cells rather than endothelium. |
| Sheehan KM et al., 2004 [3] | 48/Female | Long standing skin lesion on the calf which was progressively increasing in size and painful. | Well defined cystic tumour measuring 2.5 cm. | Spindle and histiocytic lesion with a storiform pattern containing foamy histiocytes admixed with large dilated blood vessels with no lining. |
| Kim CJ et al., 1989 [5] | 12/Female | Following a minor trauma to right parietal region, non-tender mass developed, slowly increased in size and was excised. A year later small mass recurred in the same area. | Purplish nodular mass measuring 4 x 3 x 1.3 cm with crusting and ulceration. On sectioning, revealed chocolate like gelatinous surface with cystic change. | Mass was composed of fairly cellular portions and large blood filled spaces of variable size devoid of endothelial lining. |
| Yang P et al., 1995 [6] | 41 /Male | History of rapid growth of the skin on the lower extremities. | Nodule was observed in the dermis and superficial cutis. C/S measured 3 cm in maximum dimension and appeared dark with multiple haemorrhagic cysts. | Showed a unique formation of blood filled tissue spaces and storiform proliferation of histiocyte-like and fibroblast like cells. |
| Das A et al., 2015 [7] | 30/Female | Tender swelling on the medial aspect of right thigh for four months with sudden increase in size. | A Pedunculated tumour of 6 cm. O/S- had a bluish tinge. On opening, 10 ml of brown coloured fluid came out. | Tumoural mass in the deep dermis showed spindle cells in a storiform pattern and blood filled spaces lacked an endothelial lining. |
| Present Case. 2015 | 65/Male | Slow growing polypoidal lesion with h/o recurrence on the medial aspect of mid one third of right leg. Ulceration present was following a minor trauma. | Skin covered tissue measuring 6.5 x 4.5 x 0.6 cm. Skin covered surface shows ulceration with grey brown areas. c/s-lesion dark brown with focal areas of haemorrhage. | Showed a viable tumour composed of many small and cavernous pseudovascular spaces lined by spindly tumour cells in storiform pattern. |
Aneurysmal variant mimics many other benign, malignant, vascular tumours and has to be differentiated from them [2-4]. Angiomatoid Malignant Fibrous Histiocytoma (AMFH) has to be differentiated from AFH. Clinically AMFH is seen to occur in children and young individuals associated with systemic manifestations. Tumour is found to be located in the subcutaneous tissue and lower dermis. Grossly, they are firm red-brown circumscribed lesion. Microscopically, they show solid fibro-histiocytic areas, pseudoangiomatous spaces filled with blood, thick fibrous pseudocapsule with prominent haemosiderin deposition and pericapsular cuffing of lymphoplasmacytic cells with occasional germinal centre. A prominent inflammatory infiltrate and location of the tumour in the subcutaneous tissues is noted in AMFH. AFH is entirely located in the dermis as seen in the present lesion [2-5,8,9].
Besides AMFH, the major differential diagnosis for AFH is Kaposi Sarcoma (KS). KS is clinically found to occur in elderly men and affects the lower extremities. It presents as flat, pink patches which latter acquires blue-violet papular appearance. Microscopically, the vascular spaces are lined by endothelial cells positive for CD34, a major point that differentiates KS from AFH [2-5,8].
Cutaneous angiosarcoma occurs on the face and scalp of elderly patients and long duration lesions are elevated, nodular and ulcerated, thus they mimic AFH. Histologically, they show vascular spaces lined by atypical, mitotically active endothelial cells, positive for CD34 immunostaining [2,3,5,8].
The present case showed CD34 negativity of cells lining the vascular spaces ruling out the possibility of Kaposi’s sarcoma and cutaneous angiosarcoma.
Conclusion
Rarity of aneurysmal variants of fibrous histiocytoma along with their similarity with malignant vascular tumours and clinically high recurrence rate poses a big diagnostic challenge.
[1]. Bal A, Punia RPS, Harsh Mohan, Aneurysmal benign fibrous histiocytoma of the skinIJD 2006 51(3):207-08. [Google Scholar]
[2]. McKenna DB, Kavanagh GM, McLaren KM, Tidman MJ, Aneurysmal fibrous histiocytoma:An unusual variant of cutaneous fibrous histiocytomaJ Eur Acad Dermatol Venereol 1999 12:238-40. [Google Scholar]
[3]. Sheehan KM, Leader MB, Sexton S, Cunningham F, Leen E, Recurrent aneurysmal fibrous histiocytomaJ Clin Pathol 2004 54:312-13. [Google Scholar]
[4]. Santa Cruz DJ, Kyriakos M, Aneursymal fibrous histiocytoma of the skinCancer 1981 47:2053-61. [Google Scholar]
[5]. Kim CJ, Cho JH, Chi JG, Aneurysmal (“Angiomatoid”) fibrous histiocytoma in a childJ Korean Med Sci 1989 4(4):159-62. [Google Scholar]
[6]. Yang P, Hirose T, Hasegawa T, Seki K, Hizawa K, Aneursymal fibrous histiocytoma of the skin. A histological, immunohistochemical and ultrastructural studyAm J Dermatopath 1995 17(2):179-84. [Google Scholar]
[7]. Das A, Bandyopadhyay D, Mishra V, Saha A, Aneurysmal benign fibrous histiocytoma presenting as a giant acrochordon on thighIndian Dermatol Online J 2015 6:436-38. [Google Scholar]
[8]. Dal PC, Fletcher CDM, Unni KK, Mertens F, Angiomatoid fibrous histiocytoma In Chap 9Tumours of uncertain differentiation: Pathology and Genetics of tumours of Soft tissue and Bone 2002 First editionFranceIARC Press:194-95. [Google Scholar]
[9]. Thway K, Fisher C, Angiomatoid fibrous histiocytoma:the current status of pathology and geneticsArchives of Pathology and Laboratory Medicine 2015 139(5):674-82. [Google Scholar]