Record taking in orthodontics is considered immensely important as it aids in diagnosing and determining the finest possible treatment plan for each case. The emphasis has long been on X-Rays and study models while clinical photography is often considered as a luxury; an unnecessary waste of time by many clinicians [1]. Since the time cephalostat was introduced in 1931 [2] by Broadbent and Hofrath, it has become an essential diagnostic aid in orthodontic cases for treatment planning. Its major advantages include -quantification of facial and dental relationships, identification and classification of skeletal and dental anomalies, assessment of facial growth.
Cephalometry is considered a gold standard in orthodontic diagnosis. But it has many limitations of which radiation exposure is most important. Today, with rising concerns about radiation exposure, unnecessary irradiation should be avoided since there is no threshold dose below which biologic damage does not occur.
There is an increasing need of resorting to methods that can give equal if not better results [3]. Importance of clinical photography since then is gaining momentum in orthodontic practice. Photographic analyses are inexpensive, and they help in better assessment of the harmonic relationships among external craniofacial structures, which includes influence of muscles and adipose tissue [4,5]. In a developing country like India, photography plays a very important role for diagnostic and treatment planning procedures as it is of low cost, less technique sensitive and also because the expensive cephalometric apparatus is not accessible everywhere [6]. However comparisons between cephalometric and photographic measurements have infrequently been performed and conflicting results have been obtained [7,8]. The purpose of this study was to compare and correlate the measurements obtained from lateral cephalograms and analogous measurements from standardized facial profile photographs in skeletal class II cases. This possibility of predicting cephalometric values through photographs may give us a feasible, cost effective and non invasive diagnostic tool which could be used as a non radiographic alternative to lateral cephalometry. In this study, the null hypothesis is that there is no difference between the cephalometric and analogous photographic measurements.
Materials and Methods
In the present cross-sectional study, a total of 30 lateral cephalograms and profile photographs of patients exhibiting skeletal class II malocclusion, in the age group of 19-25 years of age were selected from patients reporting for orthodontic treatment to the Outpatient Department of Orthodontics and Dentofacial Orthopedics, MS Ramaiah Dental College and Hospital, Bengaluru, Karnataka, India.
Before the study, informed consent was taken from all the patients. Ethical clearance was taken from the Ethical Committee of the Institution before the commencement of the study. Selection criteria included Patients exhibiting skeletal Class II (ANB ≥ 3 °, β angle [9]< 27°) patterns, with all permanent teeth upto second molars included and no history of orthodontic treatment or orthognathic surgery. Patients with history of craniofacial trauma, congenital anomalies, neurological disturbance, pathological migration and mutilated cases were excluded from our study. The armamentarium used included Cephalostat (KODAK CARESTREAM 9300 premium), Standardized Lateral cephalograms (soft copy), Digital SLR camera (Nikon D90) mounted with the lens (AF-S VR Micro-NIKKOR 105mm f/2.8 GED), DOLPHIN software version 11.8, Standardized photographs (soft copy), Scale, protractor, mirror, adhesive tapes, thread, plaster and Fox plane.
Radiographic procedure: Digital lateral skull radiographs were taken with Cephalostat –KODAK CARESTREAM 9300 premium. This radiographic system uses a charged couple device sensor chip as an image receptor. The exposure parameters for the digital cephalographs were 78 kV, 10 mA and 0.6 seconds. Cephalometric radiographs were taken with maximum intercuspation and lips at rest. Patient was made to stand in natural head position and the red laser line of the cephalostat marking the Frankfort Horizontal (FH) plane on the patients face was made parallel to the floor.
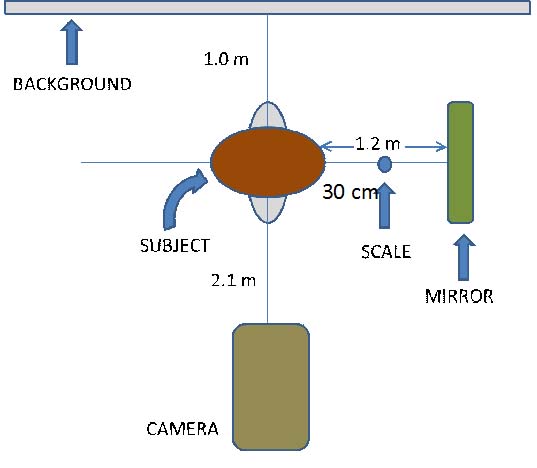
Photographic procedure: The photographic setup was standardized as shown in the [Table/Fig-1]. Adhesive dots were placed on the various anatomical landmarks that were palpable (orbitale, porion, gonion and menton). A 15 cm vertical scale was placed along the mid sagittal plane of every patient to later allow measurements at life size (1:1). A thread dipped in plaster was used to mark a line from porion to orbitale marking the FH plane. This plane was maintained parallel to the floor and at right angles to the scale on the midsagittal axis. Standardized right profile photographs were taken in the Natural Head Position (NHP) with maximum intercuspation and lips at repose [Table/Fig-2]. To obtain NHP, a mirror was placed in front of the patients, and they were instructed to tilt their head up and down with decreasing amplitude until they felt relaxed. Another photograph with the patient biting on the Fox Plane to mark the occlusal plane extraorally was also taken [Table/Fig-3]. The same digital camera (Nikon D90) with the same lens (AF-S VR Micro-NIKKOR 105 mm f/2.8 GED) mounted on a tripod was used for all the photographic records. The camera was used in its manual mode to achieve maximum image quality, given the local lighting conditions. The images obtained were transferred to the computer. Grids in Adobe Photoshop were used to confirm the parallelism of the FH plane [Table/Fig-4].
Standardized photograph with adhesive dots placed at the palpable landmarks.

Standardized photograph with patient biting on the FOX Plane.

Grids used to confirm parallelism of the FH plane (Images left to right)

The soft copies of the photos and lateral cephalograms obtained were transferred into the Dolphin software. A customized analysis was developed for the present study. The various angular and linear parameters used for this study are depicted in the [Table/Fig-5].
Various parameters used in the study.
| Angular Parameters | Linear Parameters |
|---|
| FMA | AFH |
| MP-OP angle | Ramal height |
| OP angle | PFH/AFH |
| Gonial angle | Convexity(in mm) |
| ANB angle | N perp- Point A |
| Facial angle | N perp- Pog |
| Convexity | Witts |
| Mandibular body length |
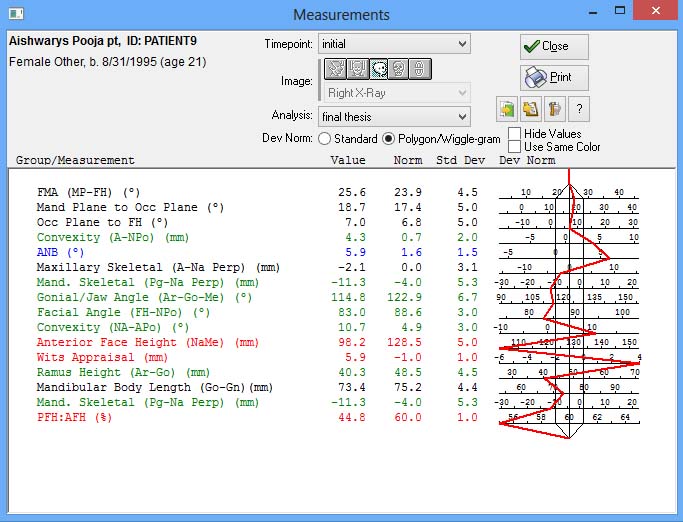
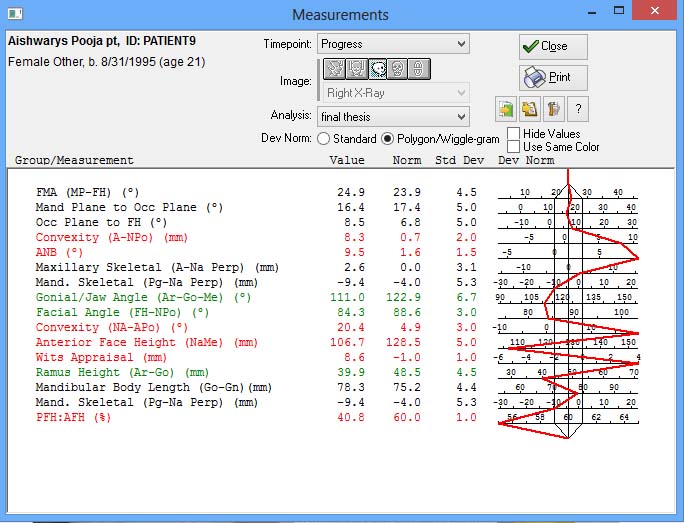
All these parameters were digitized on the photographs and lateral cephalograms using the Software. The results of the various parameters used in the study were obtained for each lateral cephalogram and photograph [Table/Fig-6,7,8 and 9]. These results were later exported and saved on MS Excel sheet.
Digitizing the lateral cephalogram using Dolphin Software.
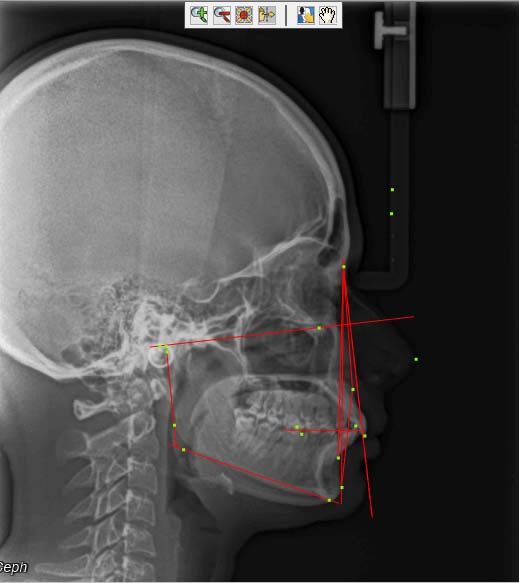
Measurements of all the parameters on the lateral cephalogram using Dolphin Software. (Images left to right)
Digitizing the photograph using Dolphin.
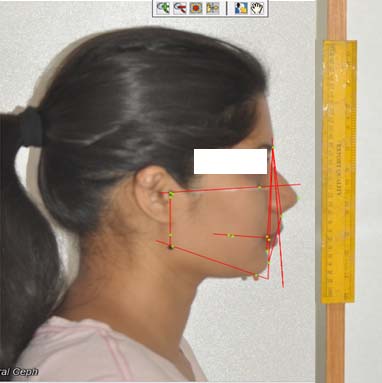
Measurements of all the parameters on the photograph using Dolphin Software. (Images left to right)
Statistical Analysis
This study was a cross-sectional study design. The data obtained was statistically analysed by using MS Excel and SPSS (Statistical Package for Social Science, Ver.16). One sample 2 tailed t-test, Pearson’s correlation coefficient and Bland-Altman test were performed to find correlation and comparison between the measurements from photographs and cephalograms in skeletal class II patients.
Results
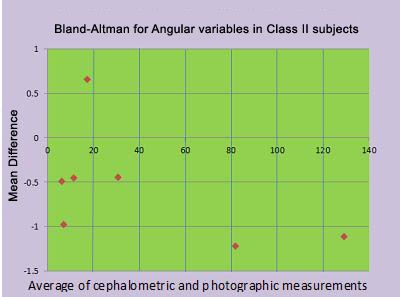
On comparing the angular cephalometric and photographic variables for the skeletal class II subjects we found all the parameters except gonial angle and facial angle to have a good relationship with the analogous photographic measurements. On comparing the linear cephalometric and photographic variables for the skeletal class II subjects we found that all the cephalometric parameters had a good relationship with the analogous photographic measurements as shown in [Table/Fig-10,11].
Comparison of cephalometric and photographic methods in assessments of angular and linear variables in skeletal class II subjects using paired t test (p< 0.05-significant), Bland-Altman test (Mean difference between -1 to +1 - significant).
| Sl no | Parameter | Ceph | Photo | Mean | Std Dv. | overall Std Dv. | Mean diff | Paired t test | p-value |
|---|
| M | F | M | F | Ceph | Photo | Ceph | Photo |
|---|
| Mean | Mean | Mean | Mean |
|---|
| Angular Parameters in Class II |
| 1 | FMA | 30.61 | 30.03 | 30.96 | 30.57 | 30.32 | 30.76 | 4.38 | 4.67 | 30.54 | -0.44 | -2.01 | 0.0543 |
| 2 | Mandibular plane-occlusal plane | 17.64 | 17.85 | 17.50 | 16.73 | 17.74 | 17.12 | 3.91 | 3.64 | 17.43 | 0.65 | 0.71 | 0.4845 |
| 3 | Occlusal plane angle | 6.95 | 6.00 | 7.61 | 7.28 | 6.48 | 7.45 | 4.40 | 4.14 | 6.97 | -0.97 | -1.46 | 0.1557 |
| 4 | Gonial angle | 129.5 | 127.4 | 130.1 | 129.0 | 128.49 | 129.5 | 5.32 | 4.59 | 129.04 | -1.11 | -1.81 | 0.0811 |
| 5 | ANB | 5.97 | 5.81 | 6.47 | 6.28 | 5.89 | 6.38 | 1.45 | 1.53 | 6.14 | -0.49 | -4.26 | 0.0002 |
| 6 | Facial angle | 80.39 | 82.09 | 81.95 | 82.97 | 81.24 | 82.26 | 3.66 | 3.37 | 81.75 | -1.22 | -4.49 | 0.0001 |
| 7 | Convexity | 12.56 | 9.87 | 13.08 | 10.24 | 11.21 | 11.66 | 3.37 | 3.20 | 11.44 | -0.45 | -1.57 | 0.1273 |
| Linear Parameters in Class II |
| 1 | Anterior facial height | 126.56 | 131.94 | 126.95 | 132.79 | 129.25 | 129.87 | 8.32 | 8.66 | 129.56 | -0.62 | -1.43 | 0.1637 |
| 2 | Ramal height | 49.88 | 49.46 | 49.57 | 50.45 | 49.67 | 50.01 | 5.78 | 5.86 | 49.84 | -0.35 | -0.60 | 0.5511 |
| 3 | PFH/AFH | 57.28 | 56.12 | 57.45 | 56.34 | 56.7 | 56.89 | 4.50 | 5.06 | 56.79 | -0.19 | -0.41 | 0.6840 |
| 4 | Convexity | 2.28 | 3.03 | 2.67 | 3.47 | 2.65 | 3.07 | 1.97 | 1.97 | 2.86 | -0.42 | -5.29 | 0.0001 |
| 5 | N perp –Point A | 0.92 | 1.37 | 1.52 | 1.71 | 1.14 | 1.62 | 2.26 | 2.15 | 1.38 | -0.47 | -1.13 | 0.2658 |
| 6 | N perp –Pog | -7.53 | -7.2 | -7.57 | -7.37 | -7.36 | -7.47 | 3.99 | 4.09 | -7.415 | 0.10 | 0.76 | 0.4559 |
| 7 | Witts | 3.80 | 3.27 | 4.16 | 3.26 | 3.54 | 3.71 | 1.71 | 1.50 | 3.625 | -0.18 | -2.25 | 0.0319 |
| 8 | Mandibular body length | 67.97 | 68.10 | 67.25 | 67.40 | 68.04 | 67.33 | 4.74 | 4.85 | 67.68 | 0.71 | -5.98 | 0.0001 |
Correlation coefficients between cephalometric and photographic measurements in the class II subjects using Pearson correlation coefficient (r > 0.5 is significant and p-value< 0.05 is significant).
| Angular Parameters | r-value | p-value |
|---|
| FMA | 0.9668 | 0.0001* |
| Mandibular plane-occlusal plane | 0.1779 | 0.3470 |
| Occlusal plane angle | 0.6373 | 0.0002* |
| Gonial angle | 0.7809 | 0.0001* |
| ANB | 0.9130 | 0.0001* |
| Facial angle | 0.9141 | 0.0001* |
| Convexity (degree) | 0.8890 | 0.0001* |
| Linear Parameters | r-value | p-value |
| Anterior facial height | 0.9620 | 0.0001* |
| Ramal height | 0.8621 | 0.0001* |
| PFA/AFH | 0.8610 | 0.0001* |
| Convexity (mm) | 0.9661 | 0.0001* |
| N perp- Point A | 0.9243 | 0.0001* |
| N perp- Pog | 0.9755 | 0.0001* |
| Witts | 0.8992 | 0.0001* |
| Mandibular body length | 0.9120 | 0.0001* |
indicates significant p-value
Discussion
Cephalometry has been established to be the contemporary gold standard for diagnosis of skeletal craniofacial morphology in orthodontic clinical practice. But because of its low cost, and no harmful radiation exposure, the photographic assessment is a pronounced diagnostic tool for epidemiologic studies. The standardized photographic technique has numerous advantages [5,10] as the subject does not move, there are no skin pressure– related errors, also it is easier to take measurements, the time needed with the patient is also lesser, also it is easier for the clinician to explain the photographs to the patient rather than a cephalogram. Additionally, measurements can be made repeatedly as well as the data can be stored permanently, making longitudinal follow up studies possible. There are some disadvantages of the photographic technique as well distortion of the image due to the presence of some distance between the subject and the lens as it causes objects farther to the camera appear smaller than those closer to it [10,11]. But this factor is only critical when we are making an attempt to equate structures located in the various planes of space. Most landmarks obtained from the cephalograms and photographs in the current study are at the midline, so this should not affect our measurements too much [11]. Furthermore, angular variables were used more often, which partially incapacitates the difficulty of magnification.
Another potential source of error is the head posture; it should be ensured that the head posture is same during the radiographic and photographic recording procedure [8]. NHP is a consistent and reproducible position of the head when the individual is in an upright posture with the eyes focused at a point in the distance at eye level, assuming that the visual axis is horizontal [12]. Even a slight deviation of the NHP can significantly affect landmark locations and alter measurement results. A standardized photography protocol also comprises of accurate establishment of landmarks. Since most photographic measurements were conducted depending upon the anatomic landmarks identified by palpation, only one operator performed palpation, computerized analysis as well as image taking.
Since the establishment of our specialty more than 100 years ago, orthodontic practice revolves around the angle paradigm [13]. Perfect occlusion was given maximum emphasis during orthodontic treatment and facial beauty was thought to follow. However, concepts changed with time. Now, it is the soft tissue proportions that receive maximum attention, and not the skeletal proportions. Proffit [13], paved the way towards this paradigm shift. Clinicians started placing maximum emphasis on the clinical evaluation of the patients and assessment of the soft tissue changes that occurred with each dentoskeletal change and with age, thus helping in better orthodontic treatment planning.
On comparing the angular cephalometric and photographic variables for the skeletal class II subjects we found the cephalometric parameters like FMA, MP-OP angle, OP angle, ANB, convexity (in degrees) to have a good relationship with the analogous photographic measurements (p>0.05) except gonial angle and facial angle (p<0.05). The angular variables including FMA, MP-OP angle, OP angle, ANB, convexity (in degrees) showed a significant mean difference (-1<Mean<1). The gonial angle and facial angle showed a mean difference -1.11 and -1.22 respectively which lies outside significant mean difference range whereas the r-values of gonial angle and facial angle showed positive correlation of 0.78 and 0.91 respectively [Table/Fig-10,11 and 12]. This could be attributed to the variability in the soft tissue chin as shown in a study by Bittner C and Pancherz H [14]. The comparison of these angular cephalometric and photographic parameters was in conjunction with with Gomes LDCR et al., [3], and Patel DP et al., [6]. Hence the photographic parameters including FMA, MP-OP angle, OP angle, gonial angle, convexity (in degree) could be used as a substitute to the analogous cephalometric parameter in class II subjects.
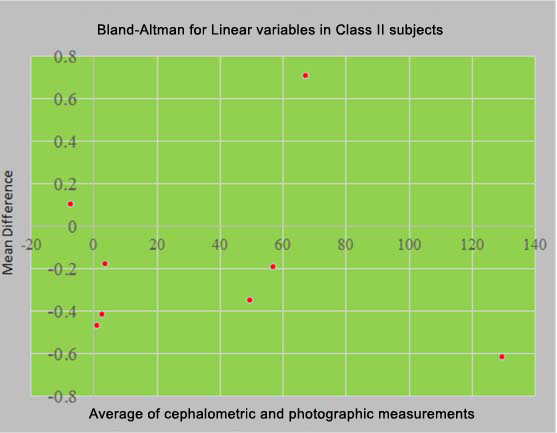
Comparison of cephalometric and photographic methods in assessments of linear variables in skeletal class II subjects (all the points between -1 and +1 meant that the cephalometric and photographic values were similar).
On comparing the linear cephalometric and photographic variables for the skeletal class II subjects we found that the cephalometric parameters like AFH, Ramal height, PFH/AFH, N-perp-Point A, and N-perp-Pog have a good relationship with the analogous photographic measurements (p>0.05). The parameters used including AFH, Ramal height, PFH/AFH, convexity (in mm), N perp-Point A, N perp-Pog, Witts and Mandibular body length showed a significant mean difference (-1<Mean<1) [Table/Fig-10,13]. The r-values also showed high positive correlation [Table/Fig-11].
Comparison of cephalometric and photographic methods in assessments of linear variables in skeletal class II subjects (all the points between -1 and +1 meant that the cephalometric and photographic values were similar). In this case all the points are within the range, which means that all the linear variables in cephalograms and photographs were similar.
All the previous studies in literature focused on all three malocclusions together, i.e., the sample included Class I, II and III together and did not show results for the individual classes separately. Since a few similar studies had been carried out in the past but most of them either carried out the study on class I patients or all three populations, no study till now focused on class II cases separately. Hence, we could not find literature to support our results. Though, cephalograms provide us with accurate measurements, their major disadvantage is the exposure of patients to radiation. With our results we can conclude that photographs can be used as an alternative to cephalograms. The advantages of photographs are that they are safe and free from radiation, easy, less time consuming, do they do not require any special equipment. However, there are a few disadvantages which include the magnification error in photographs, and difficulty in palpation of some points.
Limitation
This study was carried out on a small sample size of 30 subjects. It focused Class II subjects only. As there were no studies in literature based on class II subjects other than ours, further research in this field is needed to prove the importance of photographs.
Conclusion
On comparing the angular cephalometric and photographic variables for the skeletal class II subjects we found the parameters like ANB, facial plane angle had a significant p-value indicating that the difference between these photographic and cephalometric parameters was significant and hence these photographic parameters could not be used instead of the cephalometric values. All the other angular photographic variables can be used as a substitute to the analogous cephalometric parameters in class II subjects.
On comparing the linear cephalometric and photographic variables for the skeletal class II subjects we found the cephalometric parameters convexity (in mm), Witts, mandibular body length had significant p-value indicating that the difference between these photographic and cephalometric parameters was significant and hence the photographic parameters could not be used as an alternative. All the other linear photographic parameters could be used alternatively for the analogous cephalometric parameters
*indicates significant p-value