Bilateral Staghorn Calculus with Forgotten Double J Stent in Ileal Conduit Patient – A Rare Urological Challenge
Rupesh Gupta1, Ranjan Kumar Dey2, Rakesh Sharma3, Sweta Gupta4
1 Senior Resident, Department of Urology, RG Kar Medical College and Hospital, Kolkata, West Bengal, India.
2 Associate Professor, Department of Urology, RG Kar Medical College and Hospital, Kolkata, West Bengal, India.
3 Assistant Professor, Department of Urology, SMS Medical College, Jaipur, Rajasthan, India.
4 Junior Resident, Department of Obstetrics And Gynaecology, RG Kar Medical College and Hospital, Kolkata, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rupesh Gupta, 1, Khudiram Bose Sarani, Shyam Bazaar, Kolkata-700004, West Bengal, India.
E-mail: drrupesgupta@gmail.com
Forgotten DJ stent associated stone formation is not an uncommon entity. Here we are reporting the uncommon case of bilateral staghorn calculus due to forgotten DJ stent who had undergone radical cystectomy with ileal conduit diversion six years back. Management of these cases is a challenging urological situation due to inaccessible ureteric orifices. Patient was successfully treated with minimally invasive therapy in the form of combined bilateral PCNL (Percutaneous Nephrolithotomy) and ESWL (Extracorporeal Shock Wave Lithotripsy) therapy. The purpose of reporting this case is to highlight the grave consequences of a forgotten DJ stent and to discuss the difficulties encountered during the surgical steps of stone removal.
Percutaneous nephrolithotomy, Radical cystectomy, Renal calculus, Urinary diversion
Case Report
A 32-year-old male patient presented to the hospital with the complaints of intermittent dull aching left flank pain for last four months. There was history of passage of tube like structure (lower end of right DJ stent) through ileal conduit 15 days back. He had undergone radical cystectomy with ileal conduit for muscle invasive bladder tumor six years back in another hospital. Later, he did not follow up for timely removal of stents. In mean time, he was asymptomatic. His ileal conduit was draining well and there was no history of any major illness, haematuria, fever or graveluria. Clinical examination was essentially normal, showing a well-functioning ileal conduit and a healthy previous surgical scar.
Urine for routine analysis revealed alkaline pH (7.8), amorphous phosphate and triple phosphate crystals. Urine culture was positive for Escherichia coli and sensitive to amikacin, levofloxacin, cefoperazone, cefuroxime, meropenem and imipenem. His haemoglobin was 11.2 g/dl and total leucocyte count was 10800 µ/L. Serum urea and creatinine was 74 mg/dl and 2.9 mg/dl respectively.
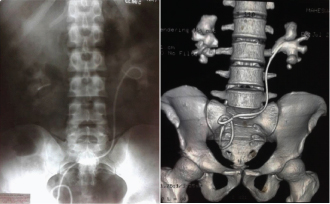
X-ray Kidney, Ureter and Bladder (KUB) revealed bilateral staghorn calculus. Additionally, a fragment of DJ stent of about 3 cm was seen in right sided kidney and complete DJ stent on left sided was seen from left kidney to ileal conduit [Table/Fig-1a]. Contrast study could not be performed due to high creatinine level, so plain CT with 3D reconstruction was advised. NCCT KUB confirmed the x-ray findings [Table/Fig-1b].
a) X-ray KUB showing bilateral staghorn calculus with a linear radio-opaque shadow at right kidney region suggestive of upper small fragment of DJ stent and complete in situ left-sided DJ stent crossing midline over sacral region toward ileal conduit; b) 3-D constructed film of plain CT showing similar findings except right DJ fragment cannot be traced in this film. (Images from left to right)
Patient was planned for bilateral PCNL first on right side than on left side in different sittings and ESWL for residual stones. IV cefoperazone was given in perioperative period. Retrograde pyelography was not possible due to inaccessible ureteral anastomotic orifices. For right sided PCNL patient was turned in prone position, care of pressure points was taken. Initial stone puncture was done with 21-gauge initial puncture needle. After confirming the tip of needle inside the system by aspirating the urine, 76% urograffin contrast was given to opacified the pelvicalyceal system. Then puncture was done in upper and lower calyces on right side and guidewire passed down in ureter, then both tracts were serially dilated to pass 30Fr amplatz sheath.
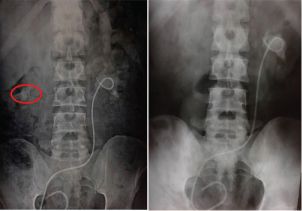
The stone was then fragmented with pneumatic lithoclast (Lithoclast Master Electro-Medical Systems, Nyon, Switzerland). DJ fragment and stone fragments were endoscopically extracted with non-traumatic grasper. About 80-90% of stone burden was removed in a single sitting. Nephrostomy tube was given though lower tract and taken out after five days [Table/Fig-2a]. Residual stone was dealt with ESWL and almost complete clearance achieved [Table/Fig-2b]. Left PCNL was done after one month in a similar manner.
a) X-ray KUB after right PCNL showing residual stone (mark by red circle) in right kidney and left side staghorn calculus with DJ in situ; b) X-ray KUB after right sided ESWL showing complete clearance of right side stone and left side as before. (Images from left to right)
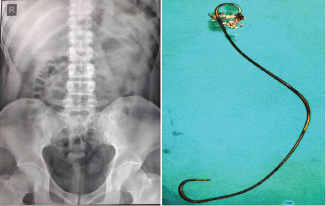
Two tracts dilatation was required in upper and middle calyces. Near complete clearance of stone was done along with the removal of intact DJ stent. Nephrostomy tube was placed in middle calyx tract. Few residual fragments were cleared by ESWL [Table/Fig-3a,b]. Struvite stone was found on analysis. The patient is doing well on follow-up. The creatinine level after one week of complete stone clearance was 1.7 mg/dl.
a) X-ray KUB after bilateral PCNL and ESWL showing complete clearance of stones and DJ stent; b) Intact removed left DJ stent specimen and retrieved stone fragments. (Images from left to right)
Discussion
After removal of bladder in radical cystectomy, urinary diversion is routinely required. Ileal conduit is easy to perform and provide low pressure diversion and have lesser complications than continent types [1]. It also has some long term complications like urolithiasis. Stone can be formed in 4.9-15.3% of patients with urinary diversion [2]. Paitent with stone in upper urinary tract usually have symptoms like pain, haematuria, UTI and graveluria. But it may remain asymptomatic for long time, so require close long term surveillance [2]. Patel and Bellman suggested routine annual x-ray KUB and flexible ureteroscopy for the patients undergone urinary diversion surgeries [3].
Ureterointestinal anastomosis is usually done over ureteric stent to provide support and drainage of urine from ipsilateral kidney. Long term indwelling stent is associated with encrustation or stone formation [2]. Proposed mechanisms for encrustation is deposition of stone components like calcium, magnesium, ammonium and phosphorus due to change in local milieu by bacterial infection induced altered pH, formation of biological biofilm and hydrophilic property of stent [4]. Silicon stent have less chance of encrustation compare to polyurethane stents but in long term, no stent is protected from encrustation [5]. Chances of stone formation are related to the indwelling duration of a stent [4,5]. So, ureteric stent should be removed or changed after appropriate duration when they are no longer required to prevent these complications. Chances of urolithiasis due to forgotten DJ stent is very less now a days because use of infant feeding tube or J stent in which one end remain outside of conduit and strict follow up protocol is used now a days.
Puri A et al., have reported a case of forgotten DJ stent with large calculus at its distal end after ileal conduit diversion and is managed by open surgery [6]. The indexed patient had bilateral staghorn calculus with forgotten in situ left sided DJ stent and upper remnant part of DJ stent in right kidney who had undergone radical cystectomy six years back. This is an uncommon presentation of forgotten DJ stent. Only a few similar cases have been reported in the literature [7,8]. Management of such cases is challenging and ideal by minimally invasive approach, open surgery should be done when other methods are not safe [9]. We have treated this patient with bilateral PCNL plus ESWL and we have achieved almost complete clearance.
Conclusion
Bilateral staghorn with forgotten DJ stent in an ileal conduit patient is a rare but challenging urological condition. We used minimal invasive therapy in terms of combined therapy (PCNL+ ESWL) and successfully patient was made stone free. This type of situation should be prevented by data registry.
[1]. Madersbacher S, Schmidt J, Eberle JM, Thoeny HC, Burkhard F, Hochreiter W, Long-term outcome of ileal conduit diversionJournal of Urology 2003 169(3):985-90. [Google Scholar]
[2]. Rajaian S, Kekre NS, Large bifid ureteric calculus in a patient with an ileal conduitUrology Annals 2012 4(3):178-80. [Google Scholar]
[3]. Patel H, Bellman GC, Special considerations in the endourologic management of stones in continent urinary reservoirsJournal of Endourology 1995 9(3):249-54. [Google Scholar]
[4]. Murthy KVR, Reddy SJ, Prasad DV, Endourological management of forgotten encrusted ureteral stentsInternational Braz J Urol 2010 36(4):420-29. [Google Scholar]
[5]. Lai CJ, Wong WJ, Tsai PK, Wu HC, Chen J, Management of a retained double-J catheter with severe encrustations:a case reportJTUA 2009 20:187-89. [Google Scholar]
[6]. Puri A, Priyadarshi V, Raizada N, Pal DK, Forgotten DJ stent with a large calculus at its distal end in an ileal conduit diversionCase Reports in Urology 2014 2014:684651 [Google Scholar]
[7]. Karbhari SS, Kriplani A, Dhaded RB, DJ stent:forgotten for fourteen yearsJournal of Evolution of Medical and Dental Sciences 2015 4(26):4527-30. [Google Scholar]
[8]. Sharma A, Andankar M, Pathak H, Two cases of retained ureteral stents presenting with breakage and encrustationsInternational Journal of Medical Research & Health Sciences 2016 5(10):208-12. [Google Scholar]
[9]. Muntaner LP, Pacios JCL, Vega AV, Rodricuez FO, Sanchez MJM, Madrid GJF, Urinary stone in a Bricker’s ileal conduitArchivos Españoles de Urología 2004 57(8):851-53. [Google Scholar]