The development of resin-based composites is one of the most remarkable contributions to dentistry as they have the advantage of conserving sound tooth structure and simultaneously providing an aesthetic restoration [1]. Despite significant material improvements in restorative dentistry, composite resins were failing predominantly because of occlusal wear or secondary caries [2-4].
Furthermore, relatively high brittleness and low fracture strength of current composite restorative materials still control their use in large stress-bearing areas [5].
The need for long lasting and substantial restorations is one of the driving forces for the development of improved materials. Therefore, studies have been undertaken to improve the wear resistance and to reduce the polymerization shrinkage of composite restorative materials [6]. Reinforcing the resin with whiskers, ceramic fillers (dense and porous) and optimization of filler levels are among the methods that have been studied [7].
Recently, composite resins reinforced with short glass fibre fillers were introduced which are intended to be used in posterior stress bearing areas as they are showing an improved load bearing capacity, flexural strength and fracture toughness when compared to the conventional particulate filler composites [8-10].
Microleakage of composite restorations occur mainly due to stresses generated along the tooth and restoration interface from polymerization shrinkage, temperature fluctuations in the oral cavity and mechanical fatigue developed through repetitive masticatory forces [11]. Contaminated particles infiltrate through the formed gaps between tooth and restoration interface and result in the postoperative sensitivity and secondary caries which in turn necessitate the re restoration. Recent developments are also mainly focusing on the polymeric matrix of the composite materials to develop systems which reduce polymerization shrinkage stress and also to make them self-adhesive to tooth structure [12].
Resin composite formulations with greater fluidity as flowable materials, are reported to offer higher flow, better adaptation to the internal cavity wall, easier insertion and improved elasticity when compared to the traditional composites [2]. Flowable composites may offer significant advantages when used as intermediate layers, as it improves adaptation to the cavity surfaces in areas that are difficult to access and manipulate, especially when highly viscous posterior composite materials are used subsequently [13].
Hence, the primary objective of the present study was to evaluate the marginal integrity of four different composite restorative techniques such as restorations with particulate filler composites, short glass fibre reinforced composites, short glass fibre reinforced composites with particulate filler composite superficial layer, short glass fibre reinforced composites with underlying flowable composite layer.
The null hypothesis was that there would not be any significant difference in the marginal integrity of restorations with particulate filler composites, short glass fibre reinforced composites, fibre reinforced composites with particulate composite superficial layer, short glass fibre reinforced composites with underlying flowable composite layer.
Materials and Methods
The in-vitro study was conducted in Department of Pedodontics and Preventive Dentistry, GITAM Dental College and Hospital, Andhra Pradesh, India, during January and February in 2014. Twenty-eight pre-molar teeth extracted because of orthodontic reasons, free of visible caries, cracks and restorations were used in the present study. All teeth were collected from Department of Oral and Maxillofacial surgery, GITAM Dental College and Hospital, Visakhapatnam, Andhra Pradesh, India. Surface debridement of all samples were done using hand scalers and later cleaned with rubber cups and slurry of pumice. Subsequently, the samples were disinfected in 0.5% chloramine solution, and stored in distilled water at 4°C until use. A standardized Class V cavity preparation (3 x 2 x 2 mm) with occlusal margin in enamel and gingival margin extending into the cementum was done on the buccal surface of each tooth. A William’s graduated periodontal probe (Hu-friedy, Chicago, IL, USA) was used to gauge the dimensions of the cavity.
Subsequently, test samples were randomly divided into four groups, each group containing seven teeth according to the restorative material used. Group I: Particulate filler composite (Filtek Z 250 XT, 3M ESPE); Group II: Short glass fibre reinforced composite (everX Posterior, GC); Group III: Short glass fibre reinforced composite with an overlying layer (0.5-1mm) of particulate filler composite; Group IV: Short glass fibre reinforced composite with an underlying layer of flowable composite (Filtek Z 250 XT, 3M ESPE).
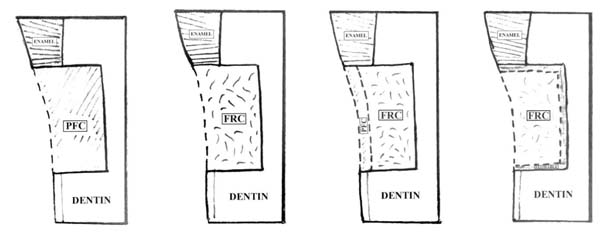
Acid etching with 37% of phosphoric acid gel (Meta Etchant, Meta Biomed Co. Ltd.), bonding agent (3M Single bond) applied and light cured (Elipar 2500 3M ESPE, Germany) for 20 seconds in all the test samples. In Group I, all samples were restored with particulate filler composite by incremental layer technique. In Group II, all samples were restored with short glass fibre reinforced composites and light cured. In Group III, samples were restored with short glass fibre reinforced composites followed by a 0.5-1 mm layer of particulate filler composite superficially and in Group IV samples were restored initially with a layer of flowable composites over the internal walls followed by fibre reinforced composites in the cavities [Table/Fig-1].
Class V restorations in the four experimental groups.
Group I: Particulate filler composite restoration (PFC); Group II: Fibre reinforced composite restoration (FRC); Group III: Fibre reinforced composite with overlying particulate filler composite; Group IV: Fibre reinforced composite with underlying flowable composite layer.
According to the type of material in each group, composite restorations were done according to the manufactures instructions and contouring of the restoration was done using mylar strip matrix band. Later, fine and superfine Sof-Lex discs (3M ESPE) were used in sequence in a slow-speed hand piece. After finishing and polishing teeth were stored in distilled water at 37°C and then subjected to thermocycling regimen of 500 cycles between 5°C and 55°C with a dwell time of one minute and three seconds of transfer time between the baths.
After thermocycling teeth apices were sealed with sticky wax. The samples were coated with two layers of nail varnish, leaving a 1 mm window around the cavity margins. Then test samples were immersed in a 2% methylene blue dye for 24 hours at 37°C, after which they were rinsed with water. Each tooth was then sectioned bucco-lingually with diamond discs. Two sections were obtained from each tooth and the section with the deepest dye penetration was selected to represent the tooth. The extent of dye penetration at the occlusal and gingival margins was determined using the stereo microscope (Olympus Optical Co, Tokyo, Japan) under 25 X magnification. The depth of dye penetration was analysed according to a 0 - 3 scale scoring system as suggested by Silveria de Araujo C [14].
Score 0 = No evidence of dye penetration [Table/Fig-2a];
Stereomicroscopic image of dye penetration scores (dye penetration in the occlusal/gingival margin was shown with red color indicator).
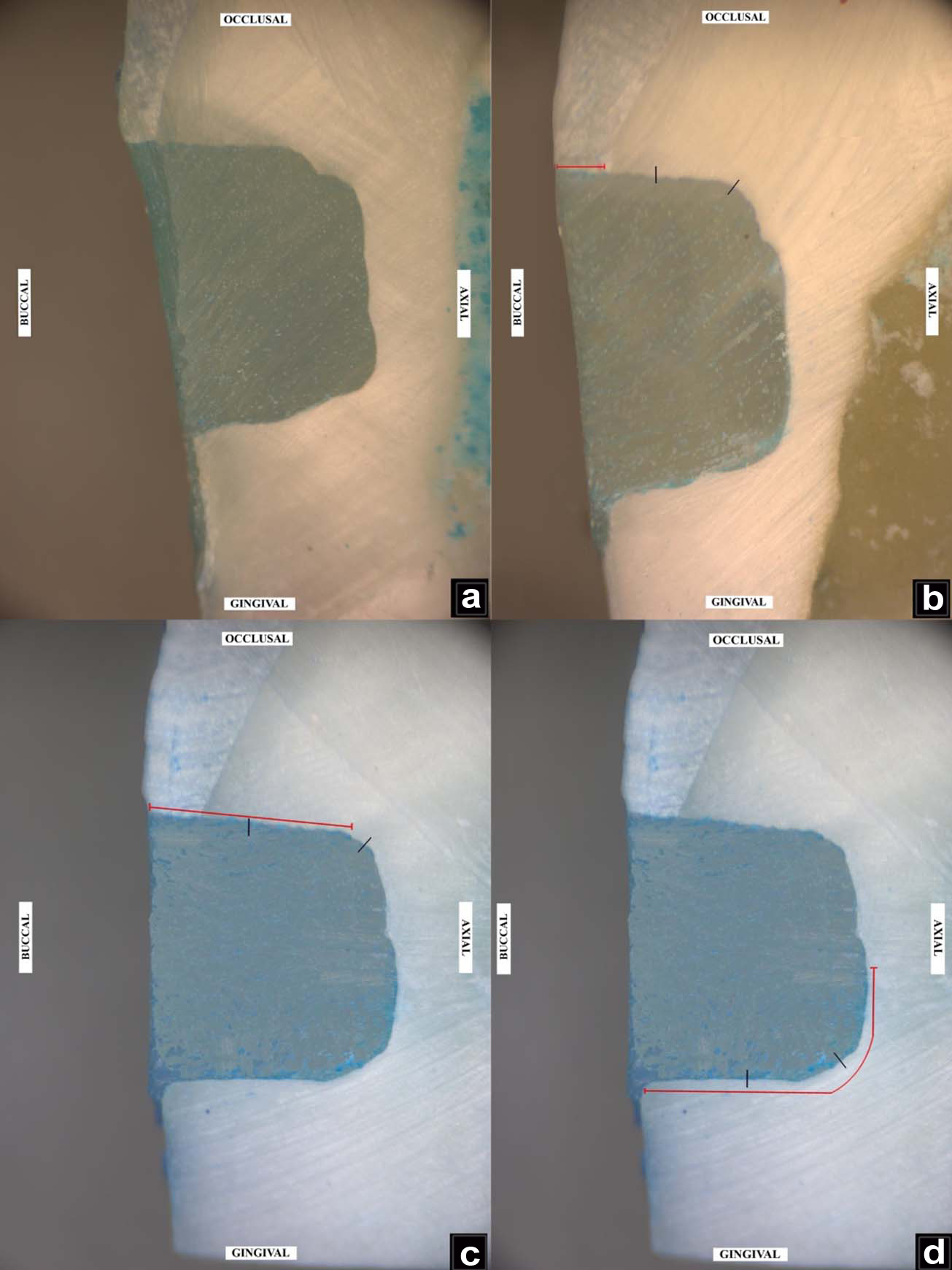
Score 1 = Dye penetration along the occlusal/gingival wall to less than half of the cavity depth [Table/Fig-2b];
Score 2 = Dye penetration along occlusal/gingival wall to more than half of the cavity depth, but not exceeding on to the axial wall [Table/Fig-2c];
Score 3 = Dye penetration along occlusal/gingival wall to full cavity depth and exceeding on to the axial wall [Table/Fig-2d];
Statistical analysis
Microleakage scoring was done separately for occlusal and gingival margins and compared using the independent sample t-test. Inter group comparison for occlusal and gingival marginal leakage scores were compared using one-way ANOVA analysis. The significant statistical difference two groups were calculated using Tukey’s post-hoc analysis. Significance was considered at the ≤ 0.05 level.
Results
Mean change in microleakage scores of occlusal and gingival margins in all the treatment groups were presented in [Table/Fig-3,4]. The comparison of occlusal and gingival microleakage scores between all the treatment groups showed a statistically significant difference (p=0.02). Mean changes in microleakage scores and statistical significant values of the occlusal and gingival margins for experimental groups were presented in the [Tables/Fig-5,6] respectively.
Mean change in microleakage scores of occlusal and gingival margins in all the treatment groups combined.
| Groups | Mean change in microleakage scores Mean±SD (n = 28) | Mean difference (95% CI) | p- value |
|---|
| Occlusal Margin | 1.3±1.09 | -0.607 (-0.082 - -1.133) | 0.024* |
| Gingival Margin | 1.93±0.86 |
Independent sample t-test was used to test the significance of microleakage scores in occlusal and gingival margins for all test samples.
- significant difference between two treatment groups (p = 0.05).
Mean microleakage scores in occlusal and gingival surfaces of all I experimental groups.
| Parameters | Group I | Group II | Group III | Group IV |
|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD |
|---|
| Occlusal | 2.14 | 1.06 | 0.42 | 0.53 | 1.14 | 2.14 | 1.14 | 1.71 |
| Gingival | 2.57 | 0.97 | 1.42 | 0.53 | 0.89 | 0.69 | 1.06 | 1.11 |
Mean change in microleakage scores of the occlusal margins between particulate filler composite (PFC), fibre reinforced composite (FRC), FRC + PFC and flowable composite with FRC.
| Treatment groups | Mean changes in microleakage scores Mean±SD (n =7) | Between groups p-value |
|---|
| Group I | 2.1±1.07 | 0.011*, 0.218†, 0.670‡ |
| Group II | 0.4±0.54 | 0.497§, 0.131‖ |
| Group III | 1.1±0.90 | 0.828** |
| Group IV | 1.6±1.13 | |
-Group I vs Group II,
- Group I vs Group III,
- Group I vs Group IV
- Group II vs Group III,
- Group II vs Group IV,
- Group III vs Group IV
Mean change in microleakage scores of the Gingival margins between particulate filler composite (PFC), fibre reinforced composite (FRC), FRC + PFC and flowable composite with FRC.
| treatment groups | Mean change in microleakage scores Mean±SD (n=7) | between groups p-value |
|---|
| Group I | 2.4±0.79 | 0.123*, 0.911†, 0.370‡ |
| Group II | 1.43±0.53 | 0.370§, 0.911‖ |
| Group III | 2.14±0.7 | 0.756** |
| Group IV | 1.71±1.11 | |
-Group I vs Group II,
- Group I vs Group III,
- Group I vs Group IV,
- Group II vs Group III,
- Group II vs Group IV,
- Group III vs Group IV
Tukey’s Post-hoc one-way ANOVA analysis showed a significant difference in the dye penetration between all the experimental groups in occlusal margin (p-value of 0.02). Group II restorations showed a less microleakage score when compared to Group I restorations with a significant difference (p=0.01). However, the Group II restorations showed no significant difference with the other two experimental groups. Microleakage score in the gingival margin showed no significant difference between the different experimental groups.
Discussion
Though improved mechanical properties of the fibre reinforced composites were evident, marginal adaptability of fibre reinforced composites are yet to be proved. Hence, in the present study short glass fibre reinforced composites (everX Posterior) were used as the experimental material to test marginal integrity in cervical restorations.
In the present study, short glass fibre reinforced composites (everX Posterior) was showing the least microleakage compared to other experimental groups (p=0.01), thus rejecting the null hypothesis for the primary objective. The results are in accordance with Tezvergil A et al., where they compared the polymerization shrinkage strain of glass fibre reinforced composites and particulate filler composites and concluded that fibre reinforced composites showed a reduced microleakage scores when compared to the particulate filler composites [15].
According to Garoushi S et al., polymerization shrinkage varies in anisotropic materials (fiber reinforced composites) where fibres are oriented in different planes and the shrinkage is not equal to all directions. They also inferred that polymerization shrinkage is controlled in direction of fibres significantly. Thus, during polymerization of fibre reinforced composites the material will not be able to shrink along the length of the fibres which support the reduced microleakage scores in the fibre reinforced composites [16].
A laboratory study reported by El Mowafy O, showed that experimental group with glass and polyethylene fibres at the gingival margins showed reduced microleakage than control group (particulate filler composites) [17]. It can be explained as the fibers replace part of the composite increment at this location, resulting in a decrease in the overall volumetric polymerization contraction of the composite. A similar in vitro study by RS Basavanna et al., reported that irrespective of the presence of flowable composites the fibre inserts reduced the microleakage in the gingival margins [18].
In the present study, samples in all groups showed relatively greater microleakage at the gingival/cemental margins rather than the occlusal/enamel margins. The results are in accordance with Garoushi S et al., where the class II cavities restored with fibre reinforced composites showed that gingival margins had higher marginal microleakage than the occlusal margins [9]. The most likely cause for this phenomenon is polymerization contraction characteristics of composites which include that polymerization shrinkage occurs towards the center of the restoration, the stronger enamel composite joint and the light source [19]. Accordingly, Yap AU mentioned that the magnitude of polymerization shrinkage is so great that even water sorption and stress relaxation cannot compensate for it [20].
The reinforcing effects of particulate filler composites with fiber reinforced composites were evaluated by Garoushi S et al., where they evaluated the effectiveness of fiber reinforced composites substructure with overlying particulate filler composites by static load-bearing capacity test. Analysing the in vitro study results, they concluded that load bearing capacity of the particulate filler composites with underlying short random fibre reinforced composites was increased significantly [21].
As the combination of particulate filler composites over fiber reinforced composites is showing a significant increase in the load bearing capacity, microleakage in this combination was tested in this study [21,22]. Thus, a superficial layer of particulate filler composites was placed over short fiber reinforced composites which was also recommended by the manufacturer’s instructions for everX Posterior [23].
In the present study, restorations with the short glass fibre reinforced composites under particulate filler composites showed more mean microleakage scores when compared to the restorations with short glass fibre reinforced composites. Though the particulate filler composites and fiber reinforced composites combination is showing improved mechanical properties, no statistical significant difference was found between the two groups (p=0.49). This might be because of the increased polymerization shrinkage in particulate filler composites overlying the short fiber reinforced composites.
Application of flowable composites as a thin layer beneath the packable composites is a common clinical technique as they show an improved clinical bonding with dentin and also they relieve contraction stresses developed during the polymerization [24-26]. Peutzfeldt A et al., suggested that these favorable effects are due to the improved cavity adaptation and stress-absorbing ability of flowable composites [27]. Hence, a combination of flowable composite as an underlying layer for short glass fiber reinforced composites was tested in the present study.
According to Ferracane JL., the properties of resin composites depend primarily on the material composition. They proposed that a correlation exists between filler content and mechanical properties, particularly for modulus of elasticity, the higher the filler content, the higher the modulus and the greater the resistance to deformation [28]. Similarly, Bayne SC et al., mentioned that lower the filler content greater the polymerization shrinkage and lower the ability to resist deformation [29].
As in accordance with Ferracane JL., in the present study, combination of flowable composites beneath the short fibre reinforced composites showed more mean microleakage scores than the restorations with fibre reinforced composites alone. However, the results of microleakage score were not statistically significant (p=0.13). This might be explained by the effects of the higher-than expected polymerization shrinkage of the flowable composite materials which has a lower filler loading and lower modulus of elasticity [28].
The present study results were in accordance with Jain P et al., where they tested the microleakage of class II resin based composite restorations with four different flowable composites and they concluded that flowable composites did not influence the microleakage significantly [30]. However, the present study results were contradictory to the Estafan AM et al., where they evaluated microleakage scores in four different low viscous composites systems and they concluded that flowable composites resist microleakage in enamel and cementum/dentin margins [31].
Limitation
Though every effort was taken to mimic the clinical condition in the present study, number of teeth per group can be improved for reliable results. In addition, use of microtome rather than diamond discs for sectioning the tooth, could have improved the stereo microscopic examination. However, for accurate assessment of the marginal integrity in experimental groups additional testing procedures such as nano leakage tests using silver nitrate are recommended.
Conclusion
The study revealed that short glass fibre reinforced composites shows the improved marginal integrity than traditional particulate filler composites. However, superficial layer of particulate filler composites and underlying flowable composites couldn’t improve the marginal integrity of short glass fibre reinforced composites in the present study. Thus, it can be inferred that short glass fibre reinforced composites are indicated in high stress bearing areas which warrant the improved marginal integrity.
Independent sample t-test was used to test the significance of microleakage scores in occlusal and gingival margins for all test samples.
*- significant difference between two treatment groups (p = 0.05).
*-Group I vs Group II,
†- Group I vs Group III,
‡- Group I vs Group IV
§- Group II vs Group III,
‖- Group II vs Group IV,
**- Group III vs Group IV
*-Group I vs Group II,
†- Group I vs Group III,
‡- Group I vs Group IV,
§- Group II vs Group III,
‖- Group II vs Group IV,
**- Group III vs Group IV