A Rare Case of Intestinal Malrotation and Volvulus of Jejunum with Coexisting Carcinoid Tumour of Appendix
Priyanka Tiwari1, Darshan Patel2, Vimal Dhaduk3, Prasanna Kumar Reddy4, Jainudeen Khalander Abdul Jameel5
1 Registrar, Department of Gastrosurgery and Minimal Access Surgery, Apollo Mains Hospital, Tamil Nadu, India.
2 Registrar, Department of Gastrosurgery and Minimal Access Surgery, Apollo Mains Hospital, India.
3 Registrar, Department of Gastrosurgery and Minimal Access Surgery, Apollo Mains Hospital, India.
4 Senior Consultant and Head, Department of Gastrosurgery and Minimal Access Surgery, Apollo Mains Hospital, Tamil Nadu, India.
5 Senior Consultant, Department of Gastrosurgery and Minimal Access Surgery, Apollo Mains Hospital, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Priyanka Tiwari, 72, Gengu Reddy Road, Egmore, Chennai Apollo Girls Hostel, Room No 2A, Chennai-600006, Tamil Nadu, India.
E-mail: dr.priyankatiwari@hotmail.com
Malrotation of the midgut is generally regarded as a paediatric pathology. It is rare in adults. Patients may present with symptoms of acute bowel obstruction or chronic abdominal pain. Barium study, Contrast Enhanced Computed Tomography (CECT), Magnetic Resonance Imaging (MRI), diagnostic laparoscopy and sometimes explorative laparotomy are used for diagnosis. Ladd’s procedure through the open approach has been the treatment of choice for complete malrotation of midgut, however there are reports on successful outcome for both complete and incomplete malrotation after laparoscopic approach as well. We report a case of a 25-year-old female who presented with a history of severe pain in abdomen for one week. CECT abdomen showed incomplete malrotation and volvulus in midgut. Laparoscopic detorsion of bowel loops, adhesiolysis, caecopexy and appendectomy was done. Patient’s symptoms subsided immediately after surgery. Histological analysis of the appendix specimen showed small appendiceal carcinoid, which was purely incidental. At three months follow up, patient was symptom free.
Chronic abdominal pain, Intestinal obstruction, Laparoscopic detorsion
Case Report
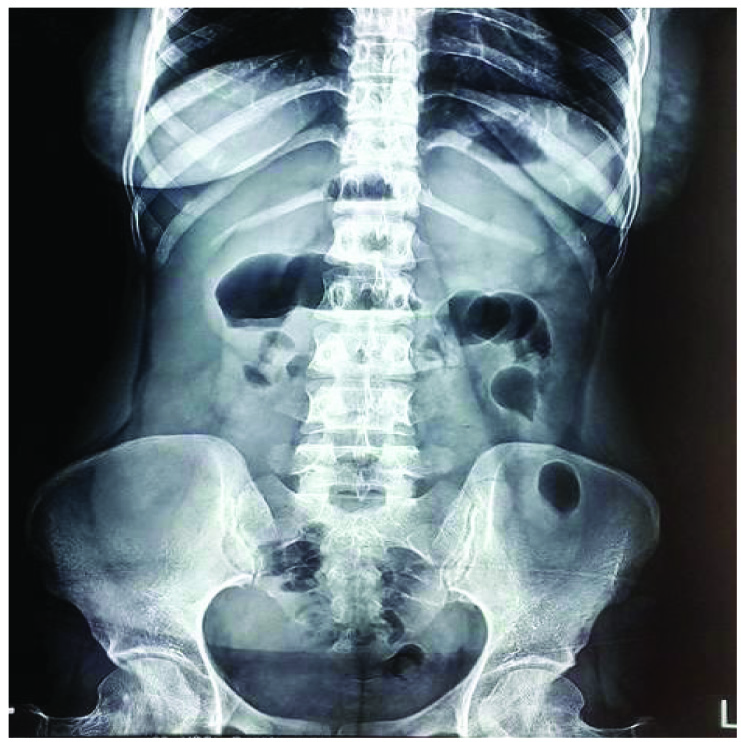
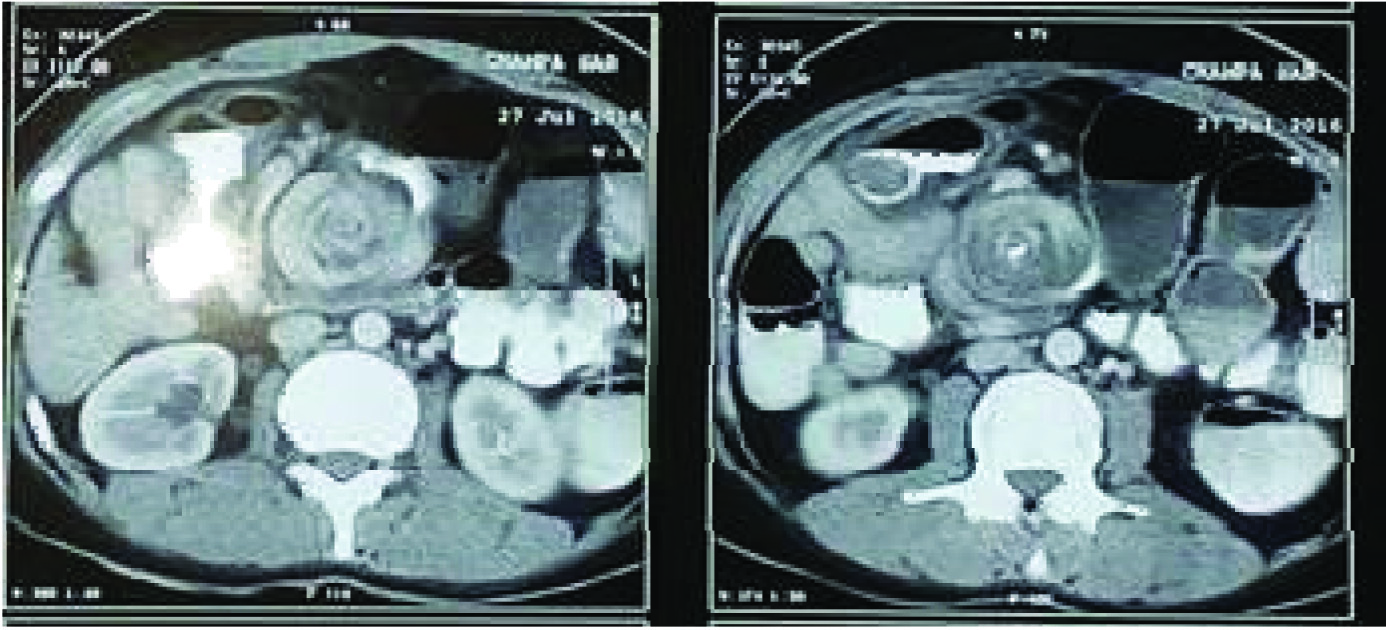
A 25-year-old female presented with history of severe colicky abdominal pain for seven days. She also had postprandial vomiting for 10 days. She had multiple similar episodes since childhood which had settled with conservative management. Abdominal examination was unremarkable. Abdominal X-ray revealed a few distended centrally located small bowel loops [Table/Fig-1]. Blood tests revealed Hb – 9.9 gm/dl, White cell count -10,400/mm3, ESR -34, Platelet count -2.28 lakh/mm3, Na -141 mmol/, K-3.61 mmol/l, Urea -26 mg/dl, Creatinine -0.83 mg/dl, Amylase -75U/l, Lipase -200U/l. CRP– 20.4. CECT showed multiple dilated small bowel loops with a “whirlpool sign” and loss of normal SMA/SMV relationship in keeping with midgut malrotation [Table/Fig-2].
X- ray showing distended small bowel loops
CECT abdomen showing dilated small bowel loops with “whirlpool” sign.
Patient was taken up for a laparoscopy. Patient was placed in supine position with split leg position. Camera port was introduced through open technique and pneumoperitoneum created. Two 5 mm working ports were introduced to the right and left of the rectus muscle. Caecum was floppy and excessively mobile, appendix was subhepatic in position and small bowel loops were dilated and twisted around mesentery in two whirls and anatomic relation of SMV and SMA was altered [Table/Fig-3]. Duodeno-jejunal (DJ) flexure was identified. Dense adhesions were present around the DJ flexure and around the jejunal mesentery. These adhesions were released [Table/Fig-4]. Two small bowel loops distal to DJ flexure were found to be twisted clockwise. Adhesiolysis was performed to separate the small bowel loops and de-twisting was done. Caecum was placed in right lower quadrant and fixed to right lateral wall of abdomen with 2-0 prolene [Table/Fig-5]. Appendectomy was done as a routine procedure. Patient was allowed clear liquids orally on the first postoperative day and slowly progressed to soft diet. Her postoperative course was entirely uneventful. Histopathology of appendix showed a 1 cm benign carcinoid tumour in the base of appendix, the resection margin of which was clear of tumour.
Appendix subhepatic in position.


Discussion
Intestinal malrotation represents one of the most common congenital anomalies of gastrointestinal tract. Although, most of the cases manifest during the first year of life, complications from malrotation including midgut volvulus and obstruction may present at any age [1]. Nonspecific recurrent abdominal complaints in adults of any age should raise suspicion of the possibility of midgut malrotation with or without concomitant volvulus [2].
Embryologic steps of intestinal rotation have been well described by Mall FP in his paper published over a century ago [3]. In the fifth week of embryologic development, there is rapid elongation of the intestinal segment and the primary gut loop extends ventrally into the umbilical cord. By the 10th week, the abdomen has enlarged sufficiently to accommodate the growing intestinal tract and as it returns to the abdomen, there is a 270° counter clockwise rotation of the tube around the axis of the superior mesenteric artery, followed by fixation. Malrotation refers to interruption, reversal or arrest of this complex process and ranges from non-rotation to incomplete rotation or lack of fixation. This may result in axial rotation of the midgut causing midgut volvulus, although even complete malrotation may be asymptomatic.
Malrotation with volvulus in newborn usually presented with bilious vomiting in 40% to 60%. Few cases present with abdominal distension, hematemesis, hematochezia, peritonitis and shock. Adults present with intermittent episodes of pain in abdomen. As malrotation is rare in adults, there is often delay in diagnosis and treatment. A high index of suspicion is therefore required [4]. There are no plain abdominal x-ray findings that are pathognomic of intestinal malrotation with volvulus. CECT findings of twisting of mesenteric vessels, bowel obstruction and malposition of caecum may suggest malrotation. CECT is also a good tool to detect the “whirlpool” sign of volvulus secondary to malrotation, however in most cases the diagnosis is made only at laparoscopy [5].
Although, malrotations in children and adults have been treated historically by the open approach, with advancements in laparoscopic expertise worldwide, there are many reports of successful outcome after laparoscopic approach for both incomplete and complete midgut malrotation [6]. Laparoscopy is now regarded as a safe and effective method in the diagnosis and treatment of intestinal malrotation both in infants and young children [7].
Presence of an appendiceal carcinoid in a patient undergoing appendicectomy during surgery for malrotation is extremely rare. To our knowledge, only one case has been previously reported [8]. Our patient’s histology suggested a benign carcinoid tumour. In general, it is recommended to do a right hemicolectomy subsequently if the carcinoid tumour of the appendix is more than 2 cm or if it is less than 2 cm with positive lymph nodes. As this was only a 1 cm tumour with a clear resection margin and there was no local lymphadenopathy on preoperative CT scan, appendicectomy that we had performed was deemed sufficient [9].
Conclusion
Laparoscopic detorsion of incomplete midgut malrotation associated with jejunal volvulus is a safe and effective procedure. Finding of a carcinoid tumour in the appendix during a routine appendicectomy for such a procedure is rare.
[1]. Sartorelli K, Schneider JG, Surgical conditions of the small intestine in Infants and childrenShackelford’s Surgery of the Alimentary Tract1Chapter 83:1046-1049. [Google Scholar]
[2]. Haak BW, Bodewitz ST, Kuijper CF, de Widt-Levert LM, Intestinal malrotation and volvulus in adult lifeInternational Journal of Surgery Case Reports 2014 5(5):259-61. [Google Scholar]
[3]. Mall FP, Development of the human intestine and its position in the adultBull Johns Hopkins hosp9(197):1898 [Google Scholar]
[4]. Okiemute FE, Abraham AA, Tony WD, Midgut malrotation first presenting as acute bowel obstruction in adulthood: A case report and literature reviewWorld Journal of Emergency Surgery 2011 6:22 [Google Scholar]
[5]. Bozlar U, Ugurel MS, Ustunsoz B, Coskun U, CT angiographic demonstration of a mesenteric vessel “whirlpool” in intestinal malrotation and midgut volvulus: a case reportKorean Journal of Radiology 2008 9(5):466-69. [Google Scholar]
[6]. Seymour NE, Andersen DK, Laparoscopic treatment of intestinal malrotation in adultsJSLS: Journal of the Society of Laparoendoscopic Surgeons 2005 9(3):298-301. [Google Scholar]
[7]. El Basatiny YM, Abdella MR, Outcome of laparoscopic diagnosis and treatment of intestinal malrotation in infants and young childrenEgypt J Surg 2015 34:22-77. [Google Scholar]
[8]. Cusimano A, Abdelghany AM, Donadini A, Chronic intermittent abdominal pain in young woman with intestinal malrotation, Fitz-Hugh-Curtis syndrome and appendiceal neuroendocrine tumor: a rare case report and literature reviewMC Womens Health 2016 16:16-3. [Google Scholar]
[9]. Roggo A, Wood WC, Ottinger LW, Carcinoid tumors of the appendixAnnals of Surgery 1993 217(4):385-90. [Google Scholar]