Aloe vera for Dry Mouth Denture Patients – Palliative Therapy
Abdul Habeeb Bin Mohsin1, S Varalakshmi Reddy2, M Praveen Kumar3, Sarah Samee4
1 Assistant Professor, Department of Prosthodontics, Sri Sai College of Dental Surgery, Hyderabad, Telangana, India.
2 Head, Department of Prosthodontics, MNR Dental College and Hospital, Hyderabad, Telangana, India.
3 Reader, Department of Prosthodontics, MNR Dental College and Hospital, Hyderabad, Telangana, India.
4 Postgraduate Student, Department of Oral and Maxillofacial Pathology, Sri Sai College of Dental Surgery, Vikarabad, Telangana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Abdul Habeeb Bin Mohsin, 23-2-360/3 Moghal Pura, Hyderabad, Telangana, India.
E-mail: doc.habeeb@gmail.com
Introduction
Xerostomia (dry mouth) is dryness of the mouth which is due to reduced salivary flow. Lack of adequate saliva causes discomfort in denture wearing patients and decreases retention of dentures. The ability of saliva to wet the tissue surface is one of the most important properties for oral comfort and retention of complete denture in dry mouth patients.
Aim
This study was conducted to evaluate and compare the wetting ability of therapeutic Aloe vera saliva substitute and commercially available Aqwet saliva substitute on heat-polymerized acrylic resin. Contact angle of liquid saliva substitute was considered as an indicator of wettability.
Materials and Methods
Aloe vera liquid (Aloe vera – Group I) and Aqwet saliva substitute (Aqwet – Group II) were compared in terms of their wetting ability. Forty samples of heat-polymerized acrylic resin were fabricated and divided into two groups with 20 samples in each. Advancing, receding contact angles and angle of hysteresis were measured using contact angle goniometer and DSA4 software analysis. Mann-Whitney U test was applied for statistical analysis of the study.
Results
The mean advancing angle and receding angle of Group I (Aloe vera) was smaller than Group II (Aqwet). Mean angle of hysteresis of Group I (Aloe vera) was higher than Group II (Aqwet). Mann-Whitney U test revealed that there is no significant difference in contact angles between the two groups.
Conclusion
Wetting ability of Group I (Aloe vera) saliva substitute was found to be better compared to Group II (Aqwet) on heat-polymerized acrylic resin.
Denture retention, Saliva, Therapeutic, Xerostomia
Introduction
Saliva is essential to the function and protection of the oral cavity and contiguous gastrointestinal epithelium. Common functions of the fluid component of the salivary secretions include cleansing and lubrication of oral soft and hard tissues, solubilization and bolus formation of food, facilitation of taste perception, mastication and speech and retention of removable prosthesis [1]. Saliva has many mechanical and chemical functions and is a fairly sensitive parameter of certain bodily functions. The patients who wear complete denture prosthesis depend on this oral fluid to provide retention and at the same time to prevent friction between the dentures and the mucosa.
Xerostomia is dryness of the oral mucosa due to reduced salivary flow, which renders it more susceptible to irritation and epithelial atrophy. In this scenario, wearing of a dental prosthesis may cause discomfort. Overall, deficiency of the saliva causes an unhealthy and painful oral environment [2]. Denture wearing may become difficult because dry mouth can significantly add to the problem of retaining and eating with the dentures, which invariably become loose.
According to Stanitz JD, the retention force is a function of saliva surface tension, liquid film thickness, surface of contact, and liquid-denture contact angle [3]. Others have analysed the role of viscosity of saliva. Blahova Z and Neuman M reported that viscosity of saliva helps to prevent the dislodgement of denture [4]. Viscosity becomes an important factor of retention in the initial phase [5,6].
Artificial saliva substitute can be a possible treatment in relieving subjective complaints of xerostomia, for that saliva substitutes should be developed containing thickeners which increase the stability of liquid for long lasting relief and increased moistening of the oral surfaces. Ideally, saliva substitutes should be soothing, pleasantly flavoured, biocompatible and economical and must have favourable wetting ability of tissue surface of the denture. An age-old remedy to treat dry mouth is Aloe vera. It also helps to protect the sensitive tissue in the mouth and enhances the moisturizing effect [7-9].
Drinking Aloe vera juice on a regular basis or swishing the mouth with it [10], both ways could be quite effective in getting a natural treatment for dry mouth. Aloe vera is easily available Over-The-Counter (OTC) in variety of preparations; it has various other benefits for the body and the skin if taken in the juice form [11]. Tello CG et al., formulated the sticky and viscous nature of Aloe vera into a denture adhesive and evaluated for adhesive strength in both wet and dry conditions; the adhesive also was used to evaluate cytotoxicity to human gingival fibroblasts. They observed stable adhesive bond strength and minimum cytotoxicity [12]. Subramaniam T et al., in their review of beneficial properties of Aloe vera in dentistry, enlightened actions of Aloe vera such as healing properties, antibacterial activity, antifungal, anti-viral and moisturizing effects, which further enhances its use as a salivary substitute in liquid form [13].
Favourable wetting ability of the heat-polymerized acrylic resin by the saliva substitute is important for good retention of the complete dentures. The advancing and receding contact angles of the saliva substitute on the heat-polymerized acrylic resin denture base can be taken as a measure of the wettability, smaller contact angle indicates greater wettability [14].
Considering the importance of wetting of acrylic denture base by saliva substitutes in xerostomia patients, this study was carried out to evaluate and compare the wetting ability of Aloe vera and Aqwet saliva substitutes on heat-polymerized acrylic resin and to present suitable therapeutic, low cytotoxic and natural saliva substitute for best wetting in dry mouth (xerostomic) denture wearers.
Materials and Methods
This in vitro study was performed at Department of Prosthodontics, MNR Dental College and Hospital, NTR University of Health Sciences and Department of Polymers and Functional Materials, CSIR-Indian Institute of Chemical Technology, Hyderabad, India, (Study period 2014–2015).
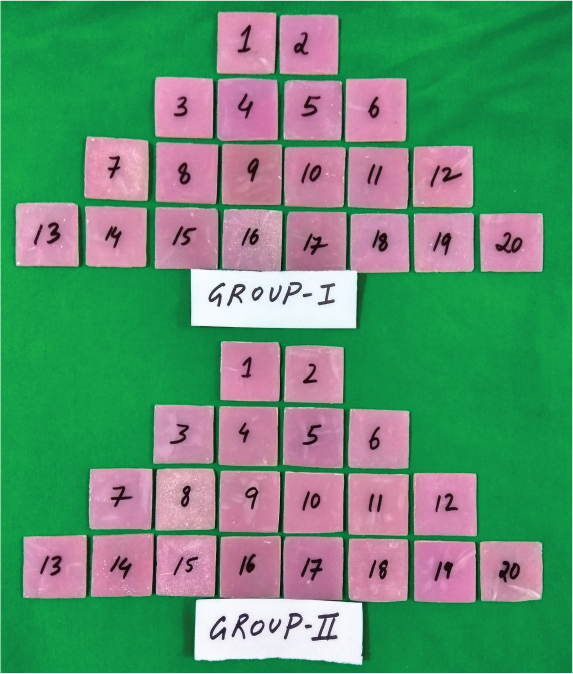
Two saliva substitutes used in this study were; Aloe vera liquid (Nature’s best) - Group I and Aqwet Saliva supplement (Cipla) - Group II [Table/Fig-1]. Forty acrylic resin samples were made using DPI (Dental Products of India) heat-polymerized acrylic resin to record contact angles of saliva substitutes on it. Forty samples were divided into two groups each containing 20 samples [Table/Fig-2].
Aloe vera liquid (Group I) and Aqwet saliva supplement (Group II).

Sample size and distribution.
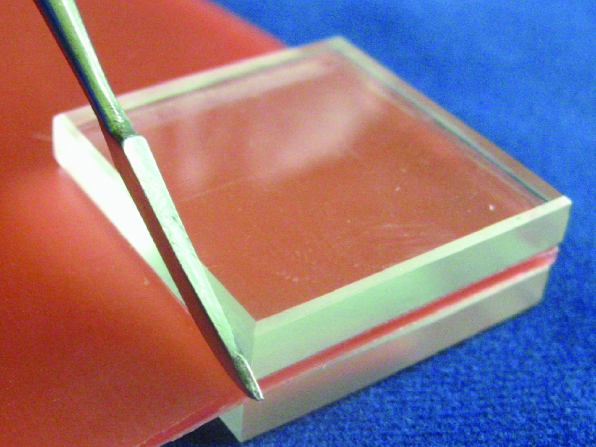
Acrylic resin samples were prepared by following method: Forty modeling wax samples of square 30x30 mm with thickness of 3 mm were obtained [Table/Fig-3]. Dental plaster was used to invest the wax samples in denture flasks. Conventional acrylization process was done according to manufacturer’s instructions to obtain 40 acrylic resin samples [Table/Fig-4]. Sample finishing was done to get an even thickness of 2 mm using acrylic trimming burs, stones and sandpaper. Tissue surface to be tested was not finished to simulate clinical practice. Other side was manually finished using sandpaper to get a uniform flat surface. The cleaning of samples was done in running water with soap and cotton, and then was cleaned with spirit, followed by ultrasonic cleaning for 15 minutes. Samples were dried and then viewed under scanning electron microscope to verify the finish.
Wax sample preparation to obtain acrylic sample.
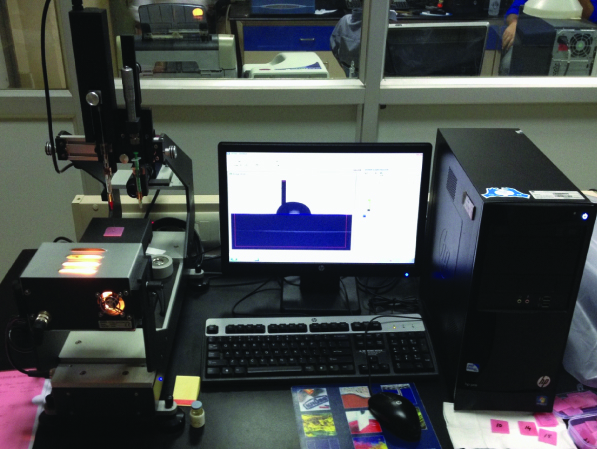
The advancing and receding contact angles of saliva substitutes were measured on acrylic samples using contact angle goniometer [14] (DSA25, KRÜSS) and software (DSA4) [Table/Fig-5] by following method: a pre-sterilized glass syringe was filled with measuring liquid (Aloe vera). Liquid drop was standardized with the help of graduated markings on the syringe. Complete care was taken not to touch the tissue surface of the sample. Tweezer was used to pick and place the acrylic sample on test table just below the needle of the syringe. Liquid drop was dispensed on acrylic plate and advancing angle was measured first, the drop was drawn backward through the needle and then receding contact angles were measured [Table/Fig-6]. After the values were obtained, the sample was removed and a new sample was placed. The procedure was repeated for remaining samples in the first group (Group I). Later, another measuring liquid (Aqwet) was filled in clean syringe and above procedure was repeated for the twenty samples in the second group (Group II), and measurements were recorded [Table/Fig-7].
Contact angle goniometer (DSA25, KRÜSS).
Measurement of contact angles using goniometer syringe.
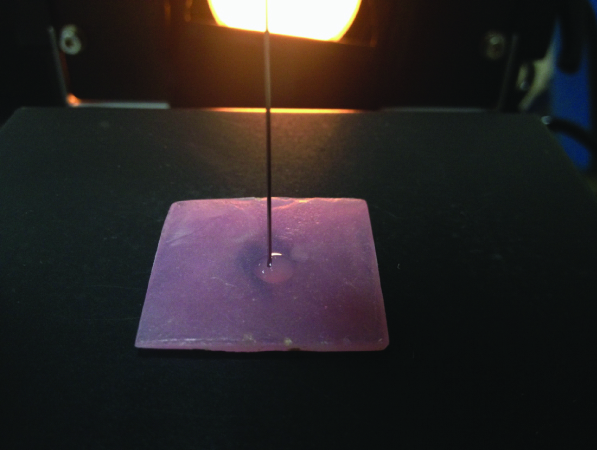
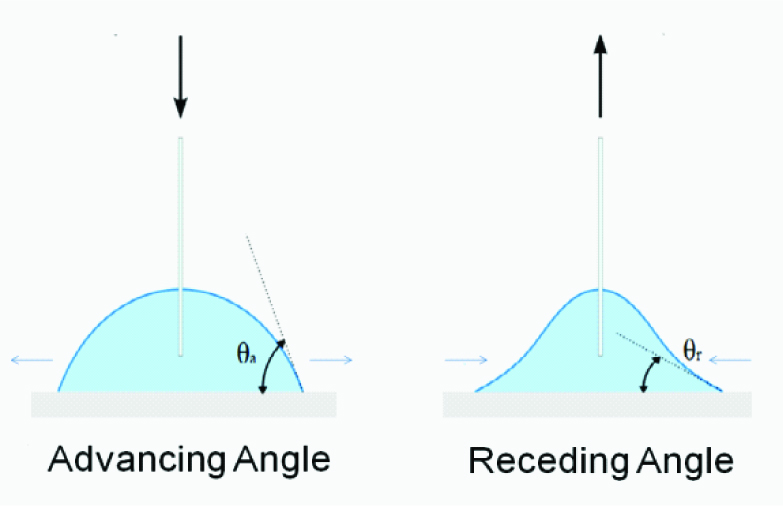
Illustration of advancing and receding contact angles.
Statistical Analysis
The statistical analysis was performed using the SPSS 18.0 software package. Mann-Whitney U two-tailed comparison statistical test was employed in the present study. Means of contact angle values were determined. The difference between the advancing and receding contact angle values was calculated as Angle of Hysteresis [15].
Results
The mean advancing angle of Group I (Aloe vera) was 75.14° and Group II (Aqwet) was 76.02°. In two-tailed comparison for advancing angle there was no significant difference between groups (p-value=0.85). Only 85% of homogeneity in Group I and Group II was seen in advancing angle [Table/Fig-8]. The mean receding angle of Group I (Aloe vera) was 69.74° and Group II (Aqwet) was 71.02°. In two-tailed comparison for receding angle there was no significant difference between groups (p-value=0.695). Only 69.5% of homogeneity in Group I and Group II was seen in receding angle. The mean angle of hysteresis of Group I (Aloe vera) was 5.40° and Group II (Aqwet) was 4.95°. In two-tailed comparison for angle of hysteresis there was no significant difference between Groups (p-value=0.223). Only 22.3% of homogeneity in Group I and Group II was seen in angle of hysteresis. Results from this study showed that mean advancing and receding contact angles values of Aloevera were less than the Aqwet and mean angle of hysteresis of Aloe vera was higher than Aqwet.
Tabular presentation of contact angles mean values and test statistics.
| Descriptive Statistics | Mann-Whitney u Test |
|---|
| Group | N | Minimum (Contact Angle) | Maximum (Contact Angle) | Mean | Std. Deviation | Statistics | Z-Value | p-Value |
| Advancing Angle | Group I | 20 | 61.8° | 87.3° | 75.14° | 7.17 | 193.0 | -0.19 | 0.850 |
| Group II | 20 | 63.5° | 87.1° | 76.02° | 6.82 |
| Receding Angle | Group I | 20 | 53.7° | 84.3° | 69.74° | 7.30 | 185.5 | -0.39 | 0.695 |
| Group II | 20 | 62.6° | 82.5° | 71.02° | 4.84 |
| Angle of Hysteresis | Group I | 20 | 0.4° | 11.4° | 5.40° | 3.11 | 155.0 | -1.22 | 0.223 |
| Group II | 20 | 0.3° | 16.2° | 4.95° | 4.96 |
Discussion
Saliva plays an important role in the retention of complete dentures and in protection of oral health. A denture causes discomfort in xerostomic patients. Artificial saliva products are useful agents for the palliative treatment of xerostomia. Saliva substitutes are divided into two groups: artificial and mucin-based saliva substitutes [16]. Mucin based saliva substitutes are not used because they are derived from porcine derivatives therefore are likely to be objectionable to the Indian population. Therefore, saliva substitutes used in the study was artificial saliva substitute which contained synthetic and natural substance, which impart lubrication and viscosity [2,17].
In study, done by Aydin AK et al., both types of artificial salivas (mucin-based and carboxymethylcellulose-based substitutes) had better wetting properties on denture base resin than the natural saliva. This further increased the scope of analysing contact angles of artificial saliva [2]. Oh DJ et al., reported that artificial saliva has significantly better effects in patients with very severe dry mouth whose functional salivary gland capacity was severely compromised. Artificial saliva decreased the patients’ discomfort during the night as well as during the day. Their quality of life may also increase following the use of artificial saliva [18]. Moisturizing effects of Aloevera enhances its use as a salivary substitute in liquid form. An age-old remedy to treat dry mouth is Aloe vera; suggested natural treatment for dry mouth is swishing the mouth with it as required [13].
To produce adequate adhesion of a denture to the supporting tissues, saliva must flow easily over the entire surface to ensure wetting of the adherend surface [5]. The contact angle hysteresis and denture geometry at the meniscus contact lines are determinant factors of denture retention [6]. Contamination of the studied surfaces may produce a change in the water surface tension that, in turn, would induce an error in the measured contact angle values. Hence, extremely careful rinsing procedure such as washing with soap water, wiping with spirit and ultrasonic cleaning of acrylic samples made it highly improbable that either chemical or microbial contamination occurred.
Advancing contact angle is defined as the angle that a liquid drop forms on a dry solid surface. Receding angle is formed when the liquid recedes on the previously wet solid surface. The difference between the advancing angle and the receding angle is called angle of hysteresis [15]. Angle of hysteresis is potential for greater wetting as the value increases. As the difference of advancing and receding angle increases angle of hysteresis increases this is proportional to both the values. The difference window of advancing and receding angle values determines angle of hysteresis so that the potential for wetting of the heat cure acrylic resin can be evaluated based on it. Contact angle hysteresis is influenced by surface heterogeneity, surface roughness, surface deformation and chemical contamination of water [15]. Equilibrium contact angle has been regarded as related to denture comfort, and denture retention is more related to contact angle hysteresis [5].
The quality of life for xerostomia patients may be improved by the use of a suitable saliva substitute. O’brien WJ and Ryge G reported that the wettability was excellent in a denture treated with silica in comparison with an untreated denture. With treated denture best wettability was found on the tissue side of the dentures which is the critical area for retention, hence it is indicated that thin film of a viscous Aloe vera will improve retention of denture [19]. According to wettability studies of contact angles, primarily wetting occurs when a solid and liquid come into contact. Contact angles less than 90 degrees (small contact angles) indicate high wettability, while contact angles more than 90 degrees (large contact angles) indicate low wettability. More specifically, a contact angle less than 90 degrees indicates that wetting of the surface is favourable, and the fluid will spread over a large area on the surface, it is considered as hydrophilic; while contact angles greater than 90 degrees generally means that wetting of the surface is unfavourable so the fluid will minimize its contact with the surface and form a compact liquid droplet, it is considered as hydrophobic. For example, complete wetting occurs when the contact angle is 0 degree, as the droplet turns into a flat puddle [20].
There are few studies reported which involved contact angles of saliva on polymer surface. Most authors confirm our research on denture base materials which reported distilled water contact angles between 58°-81° on acrylic resin [21]. Similarly, Farcasiu AT and Pauma M reported higher contact angles for natural saliva (70°-81°) and lower contact angles for artificial saliva (41°-51°) [21]. Our present study reported similar values (53.7°-87.3°). To notice the characteristics of saliva our values represent a rheological process, where saliva wets gradually. There is limited scientific studies using Aloe vera and saliva substitutes on denture base materials but we can compare to the results of Vissink A et al., [16], they investigated contact angles of water, human whole saliva and different artificial salivas on polished human enamel and on human mucosa. They found that saliva substitutes exhibit contact angles between 56.7°-61.2°.
Valid and accurate comparison of results for saliva substitutes in the present study could not be done with other scientific studies, as no previous research work has been conducted to assess the wettability of Aloe vera on denture base materials.
Future prospects may include evaluation of more naturally occurring therapeutic saliva substitutes when combined with Aloe vera to form more efficient replacement of saliva which could be more stable in terms of substantivity. Further clinical trials with larger samples needed to get the feedback from patients to determine its efficacy.
Clinical implications of this study adds to the use of best available natural and therapeutic saliva substitute for the cancer patients and geriatric patients. Antibacterial property of Aloe vera eliminates the chances of abnormal bacterial growth.
Limitation
Due to lack of available data on Aloe vera from the previous studies, proper sample size could not be determined. There are some of the limitations of contact angle measurement which is due to its system that depends on many factors including selected liquid and surface roughness of substrate.
Conclusion
Present study concluded that Group I (Aloe vera) has the smaller advancing and receding contact angle values and the higher angle of hysteresis when compared to Group II (Aqwet) on heat-polymerized acrylic resin. Based on contact angle values, Group I (Aloe vera) has the better wetting ability on heat-polymerized acrylic resin.
[1]. Napeñas JJ, Brennan MT, Fox PC, Diagnosis and treatment of xerostomia (dry mouth)Odontology 2009 97:76-83. [Google Scholar]
[2]. Aydin AK, Terzioglu H, Ulubayram K, Hasirci N, Wetting properties of saliva substitutes on acrylic resinInt J Prosthodont 1997 10:473-77. [Google Scholar]
[3]. Stanitz JD, An analysis of the part played by the fluid film in denture retentionJ Am Dent Assoc 1948 37:168-72. [Google Scholar]
[4]. Blahova Z, Neuman M, Physical factors in retention of complete denturesJ Prosthet Dent 1971 25(3):230-35. [Google Scholar]
[5]. Monsénégo P, Proust J, Complete denture retention. Part I: Physical analysis of the mechanism. Hysteresis of the solid-liquid contact angleJ Prosthet Dent 1989 62:189-96. [Google Scholar]
[6]. Monsenego PH, Baszkin A, Complete denture retention. Part II: Wettability studies on various acrylic resin denture base materialsJ Prosthet Dent 1989 62:308-12. [Google Scholar]
[7]. Dweck AC, Herbal medicine for the skin –their chemistry and effects on skin and mucous membranesPers Care Mag 2002 3:19-21. [Google Scholar]
[8]. Barcroft A, Myskja A, Aloe vera: Nature’s silent healer 2003 LondonBAAM Publishing Ltd [Google Scholar]
[9]. Surjushe A, Vasani R, Saple D, Aloe vera: a short reviewIndian J Dermatol 2008 53(4):163-66. [Google Scholar]
[10]. Bhat G, Kudva P, Dodwad V, Aloe vera: Nature’s soothing healer to periodontal diseaseJ Indian Soc Periodontol 2011 15:205-09. [Google Scholar]
[11]. Sudworth R, The use of Aloe vera in dentistry 2002 PhiladelphiaPositive Health Publications Ltd [Google Scholar]
[12]. Tello CG, Ford P, Iacopino AM, In vitro evaluation of complex carbohydrate denture adhesive formulationsQuintessence Int 1998 29:585-93. [Google Scholar]
[13]. Subramaniam T, Subramaniam A, Chowdhery A, Das S, Gil M, Versatility of Aloe vera in dentistryJ Dent Med Sci 2014 13(10):98-102. [Google Scholar]
[14]. Yuan Y, Lee TR, Contact angle and wetting properties. Surface science techniques 2013 Springer-Verlag, Berlin Heidelberg [Google Scholar]
[15]. Eral HB, ’t Mannetje DJCM, Oh JM, Contact angle hysteresis: a review of fundamentals and applicationsColloid Polym Sci 2013 291(2):247-60. [Google Scholar]
[16]. Vissink A, DE Jong HP, Busscher HJ, Arends J, S-Gravenmade EJ, Wetting properties of human saliva and saliva substitutesJ Dent Res 1986 65(9):1121-24. [Google Scholar]
[17]. Weerkamp AH, Wagner K, Vissink A, Gravenmade EJ, Effect of the application of a mucin-based saliva substitute on the oral microflora of xerostomic patientsJ Oral Pathol Med 1987 16:474-76. [Google Scholar]
[18]. Oh DJ, Lee JY, Kim YK, Kho HS, Effects of carboxymethylcellulose (cmc)- based artificial saliva in patients with xerostomiaInt J Oral Maxillofac Surg 2008 37:1027-31. [Google Scholar]
[19]. O’brien WJ, Ryge G, Wettability of poly-(methyl methacrylate) treated with silicon tetrachlorideJ Prosthet Dent 1965 15:304-08. [Google Scholar]
[20]. Yuan Y, Lee TR, Contact angle and wetting propertiesSurface science techniques 2013 [Google Scholar]
[21]. Farcasiu AT, Pauma M, Denture base materials wettability with natural and artificial salivaRomanian Journal of Oral Rehabilitation 2011 3(3):95-99. [Google Scholar]