Microtia in All the Siblings of a Family: A Rare Case
Somashekar Gejje1, Brijesh Mishra2, Amrita Anandkumar Hongal3
1 Assistant Professor, Department of Plastic Surgery, BMC and RI, Bangaluru, Karnataka, India.
2 Associate Professor, Department of Plastic Surgery, KGMU, Lucknow, Uttar Pradesh, India.
3 Consultant Dermatologist, Department of Dermatology, The Bangalore Hospital, Bengaluru, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Somashekar Gejje, Assistant Professor, Department of Plastic Surgery, BMC and RI, KR Road, Fort, Near City Market, Bengaluru-560002, Karnataka, India.
E-mail: gejje.somashekar@gmail.com
Congenital, Deformity, Ear, Genetics
Microtia literally means small ear. The simplicity of the term belies the vast complexity of this entity in terms of both the variable clinical presentation and the difficulty of surgical reconstruction [1].
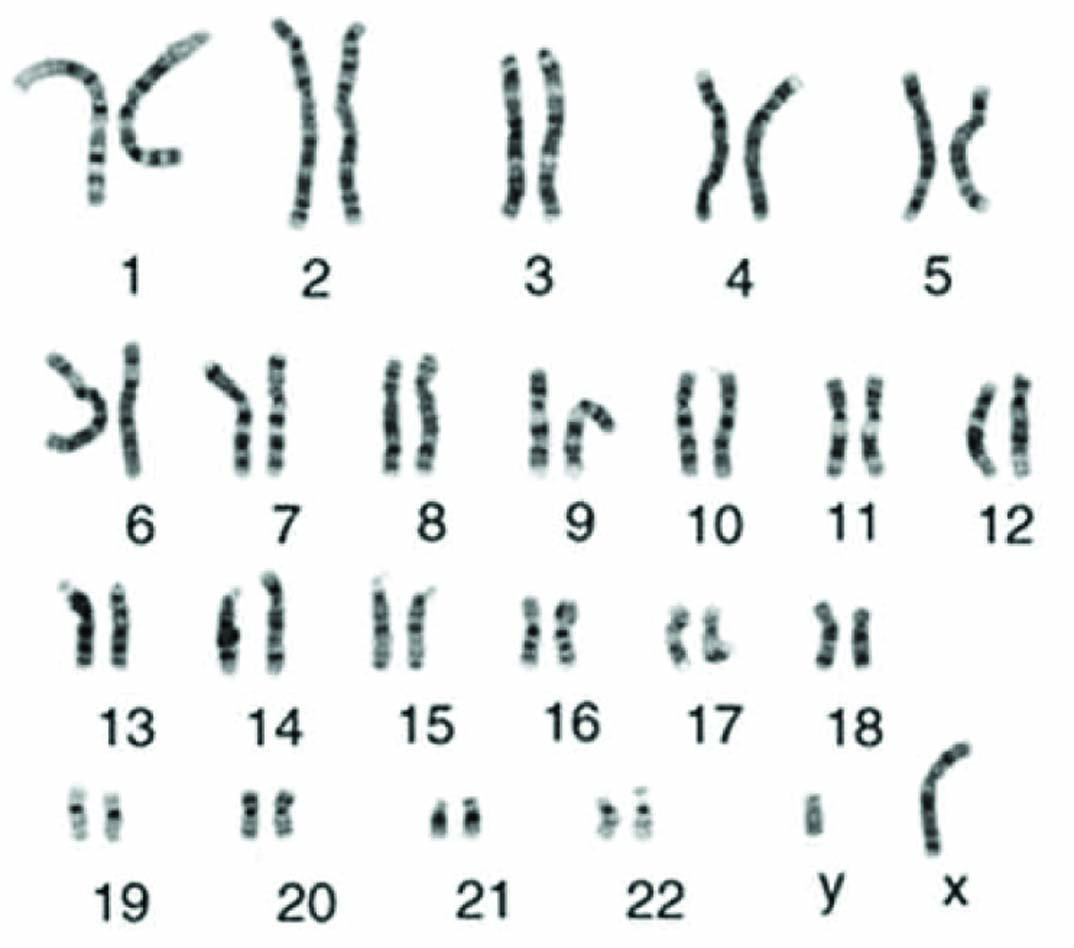
All four children of parents with second degree consanguineous marriage approached us with the chief complaints of all the children having ear deformities from birth (microtia) [Table/Fig-1]. There was no history of ingestion of teratogenic/immunosuppressive drugs during pregnancy of each kid. Eldest child was 18-year-old male and had Grade III right sided microtia, second one aged 14-year-old male had Grade II left sided microtia, another 12-year-old child had Grade II right sided microtia and the youngest girl child of 11-year-old had Grade II bilateral microtia. The parents and grandparents from both sides of four siblings had no similar deformities and were normal. Furthermore, genetics of the index case revealed normal karyotype [Table/Fig-2]. Genetics of the other siblings was not done because of financial constraints. All the kids were clinically evaluated for any other congenital abnormality and they had no problems. The external auditory canal of all the affected siblings was normal except for the pinna. The parents and the children were explained in detail about the stage autologous rib graft reconstruction of the pinna. Consent was taken for the surgeries and photographs.
All the siblings having microtia shown in a single frame.

Karyotype of the index case revealed normal findings.
The majority of microtia cases are combined with atresia or stenosis of the auditory canal, and there is a high correlation between the degree of microtia and the frequency of external and middle ear abnormalities. Incidence has been reported as sporadic instances instead of as familial cases. The prevalence of microtia has been reported to vary from 0.83% to 17.4% per 10,000 population [2].
Microtia can be a feature in a wide variety of chromosomal abnormalities, including the most common trisomy aneuploidies of chromosomes 13, 18, and 2 and genetic factors are likely to affect the occurrence in at least some patients with microtia [3].
Many genes like goosecoid gene, TCOF 1 gene (Treacher Collins Syndrome), HOXA1 and HOXA2 gene, TBX1, Fibroblast Growth Factor 3 (FGF 3), 4p24 and 18q deletions have been reported to influence microtia [4].
According to the Marx Classification, [5] in Grade 1, all the structures of a normal auricle are preserved but the pinna is smaller, in Grade 2, some anatomical structures can be still recognised, in Grade 3 type (most common and also called the peanut type), only a rudiment of soft tissue is present and Grade 4 is the extreme type where there is absent external ear and auditory canal.
Reconstructive options for microtia are autogenous type (using the popular Nagata and the Brent technique), composite type using autogenous tissues and alloplastic implants and last the prosthetic type [6].
Conclusion
To conclude, most of the cases of microtia occur in isolated fashion. Only rarely does microtia appear to run in families.
[1]. Charles H Thorne, Ear ReconstructionGrabb and Smith Plastic SurgerySeventh editionWolters Kluver, Lippincott Williams and Wilkins:285 [Google Scholar]
[2]. Suutarla S, Rautio J, Ritvanen A, Jero J, Klockars T, Microtia in Finland: Comparison of characteristics in different populationsInt J Pediatr Otorhinolaryngol 2007 71:1211-17. [Google Scholar]
[3]. Forrester MB, Merz RD, Trisomies 13 and 18: Prenatal diagnosis and epidemiologic studies in Hawaii 1986-1997Genet Test 1999 3:335-40. [Google Scholar]
[4]. Perez-Aytes A, Ledo A, Boso V, Saenz P, Roma E, Poveda JL, In utero exposure to mycophenolate mofetil: A characteristic phenotype?Am J Med Genet A 2008 146A:1-7. [Google Scholar]
[5]. Marx H, Denker Kahler O, Handbook of the diseases of the neck, nose and throat including border regions vol. VI 1926 BerlinSpringer-Verlag:131 [Google Scholar]
[6]. Charles H Thorne, Ear ReconstructionGrabb and Smith Plastic Surgery7th editionWolters Kluver, Lippincott Williams and Wilkins:287 [Google Scholar]