The liver is wedge shaped, largest gland of the body. It is situated under the right dome of diaphragm and mainly occupies the right hypochondrium and epigastric region. It is divided into anatomical right and left lobe by the attachment of falciform ligament, fissure for ligamentum venosum and fissure for ligamentum teres. The caudate and quadrate lobes are parts of the right lobe of liver. The gall bladder fossa is situated on the inferior surface of right lobe and fundus of the gall bladder is situated beyond the inferior border of the liver [1].
It has caudate and quadrate lobes as the parts of the right anatomical lobe. The fossa for the gall bladder is situated on the inferior surface of right lobe of the liver and gall bladder is situated in it. The fundus of the gall bladder usually projects beyond the inferior border of the liver [1].
The liver has four lobes or eight segments depending on whether it is defined by its gross anatomical appearance or by its internal architecture. Knowledge of variation in liver anatomy is required for good surgical outcome, diagnostic imaging and minimally invasive surgical procedures. Morphological variations of the liver are common like one or more accessory lobe, liver cyst, atrophy of liver and absence of one of the lobes [2].
A sound knowledge of the normal and variant liver anatomy is a prerequisite to having a favourable surgical outcome and commonly occurring variations assume even more significance in the era of diagnostic imaging and minimally invasive surgical approaches. Morphological variations of the liver are irregularities in the form, occurrence of one or more accessory lobes or presence of cyst; less common abnormalities are, atrophy or complete absence of one of the lobes [2].
Accessory lobes can occur in numerous places. The exact reason for the origin of accessory lobe of liver in man is still unknown. In most cases, the accessory lobe is found in the infra-hepatic position. Riedel’s lobe is the best known example of a sessile accessory lobe. Accessory lobes may also trigger tumour [2]. Aim of this study was to find out morphological variations of liver. Now-a-days the knowledge of this kind of variations are important for surgeons and gastroenterologists in planning and performing the surgical procedures, for the radiologists to prevent a possible misdiagnosis and for the anatomists to find out new variants.
Materials and Methods
This present observational study was conducted on 80 human livers from embalmed cadavers in the Department of Anatomy, Medical College, Vadodara from December 2012 to December 2016 The liver specimens were removed from adult human cadavers during routine dissection for medical undergraduate students of batch over a period of four years and then preserved in 10% of formalin. The lobes of the liver, right lobe, left lobe, caudate lobe and quadrate lobe were studied in detail for their morphological features and classified according to Netter’s classification [Table/Fig-1] [3]. The specimens were photographed. All intact cadaveric livers with no obvious deformity were studied. Liver with features of cirrhosis or any damage was excluded.
Showing different morphological variations of liver.
| Morphological features | Number of specimens (%) |
|---|
| Normal | 14 (17.5 %) |
| Accessory fissures | 10 (12.5 %) |
| Accessory fissures on caudate lobe | 3 (3.7%) |
| Superior and Inferior quadrate lobe | 6 (7.5%) |
| Pons hepatis connecting left lobe with quadrate lobe | 1 (1.25%) |
| Absence of fissure for ligamentumteres | 9 (11.2%) |
| Riedel’s lobe present | 1 (1.25%) |
| Elongated left lobe present | 10 (12.5%) |
| Mini accessory lobe present | 3 (3.7%) |
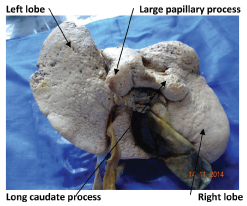
| Large papillary process and long caudate process | 1 (1.25%) |
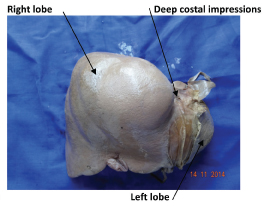
| Netter Type 1 (Very small left lobe, deep costal impressions) | 14 (17.5 %) |
| Netter Type 2 (Complete atrophy of left lobe) | - |
| Netter Type 3 (Transverse saddle like liver, relatively large left lobe) | - |
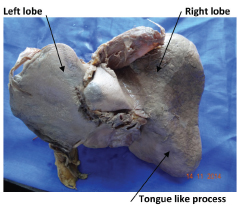
| Netter Type 4 (Tongue like process of right lobe) | 1 (1.25 %) |
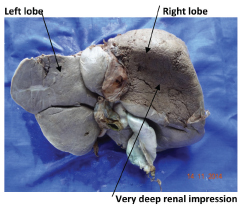
| Netter Type 5 (Very deep renal impression and corset constriction) | 1 (1.25 %) |
| Netter Type 6 (Diaphragmatic grooves) | 6 (7.5 %) |
| Total | 80 (100%) |
Results
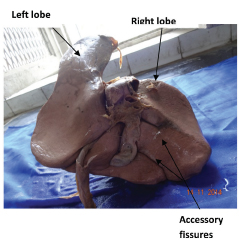
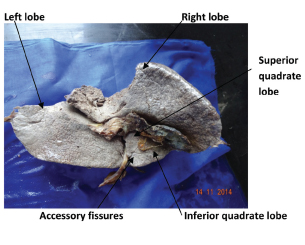
Total 80 embalmed human livers were evacuated in this study among which 14 livers (17.5%) were normal in their external appearance. However, 66(82.5%) specimens showed anomalies in fissures, lobes, shape and size of lobe, six types of variations according to Netter’s classification [Table/Fig-1] [3]. Ten (12.5%) specimens had accessory fissures on the different lobes, which resulted in the formation of accessory lobes [Table/Fig-2]. A complete transverse fissure dividing quadrate lobe into a superior and an inferior lobe were seen in 6(7.5%) specimens [Table/Fig-3].
Showing accessory fissure on right lobe;
Showing accessory fissure with superior and inferior quadrate lobe.
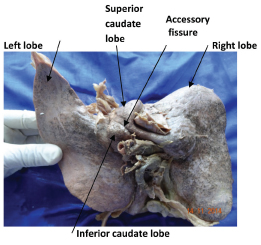
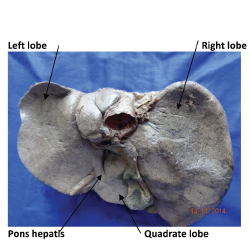
A complete transverse fissure dividing caudate lobe into a superior and an inferior lobe were seen in 3(3.7%) specimens [Table/Fig-4]. Variable size and shape of pons hepatis joining the left lobe with quadrate lobe was seen in 1(1.25%) specimen [Table/Fig-5].
Showing accessory fissure with superior and inferior caudate lobe;
Showing pons hepatis connecting left lobe with quadrate lobe.
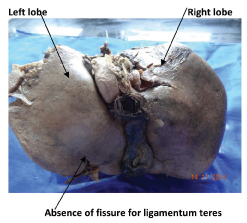
Absence of fissure for ligamentum teres was seen in 9(11.2%) specimens [Table/Fig-6]
Showing absence of fissure for ligamentum teres;
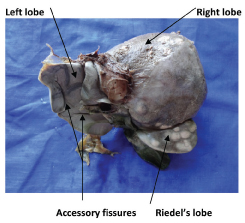
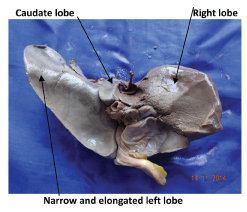
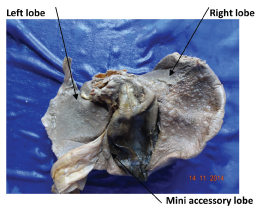
The Riedel’s lobe was present in 1(1.25%) specimen [Table/Fig-7]. Elongated left lobe present in 10(12.5%) specimen [Table/Fig-8] while a mini accessory lobe above quadrate lobe was seen in 3(3.7%) specimens [Table/Fig-9]. Large papillary process was present in 1(1.25%) specimen [Table/Fig-10]. Type 1 (Very small left lobe, deep costal impressions) was present in 14 (17.5 %) specimens [Table/Fig-11]. Type 4 (Tongue like process of right lobe) was present in 1 (1.25 %) specimen [Table/Fig-12]. Type 5 (Very deep renal impression and corset constriction) was present in 1 (1.25%) specimen [Table/Fig-13]. Type 6 (Diaphragmatic grooves) was present in 6 (7.5%) specimens [Table/Fig-14]. Type 2 (Complete atrophy of left lobe) and Type 3 (Transverse saddle like liver, relatively large left lobe) were not found in any of the livers.
Showing Riedel’s lobe with accessory fissures and large gall bladder.
Showing a narrow and elongated left lobe;
Showing mini accessory lobe.
Showing large papillary process and a very long caudate process;
Netter’s Type-1 showing very small left lobe with deep costal impressions.
Netter’s Type-4 showing tongue like process on right lobe.
Netter’s Type-5 showing very deep renal Impression and corset constriction.
Netter’s Type-6 showing very deep diaphragmatic grooves.

Discussion
The common congenital anomalies in liver are agenesis of the lobes, absence of segments, deformed lobes, smaller lobes, atrophy of the lobes and hypoplastic lobes. It is mainly due to defective development or excessive development and sometimes these deformities are present with abnormality of diaphragm and suspensory apparatus of the liver [4]. The other rarest abnormalities are seen in lobar and segmental part of liver. It has recently been reported that some apparent morphological changes detected during advanced imaging examinations may actually be pseudo-lesions resulting from perfusion defects, focal fatty infiltrations and other causes, and may not represent true parenchymatous lesions [5].
Accessory fissures were seen on right lobe, quadrate lobe and caudate lobe. According to Auh YH et al., the accessory hepatic fissures are potential sources of diagnostic errors during imaging. Any collection of fluid in these fissures may be mistaken for a liver cyst, intrahepatic haematoma or liver abscess. Implantation of peritoneally disseminated tumour cells into these spaces may mimic intrahepatic focal lesions [6]. According to Torzilli G et al. used intraoperative ultrasonography during liver surgery and detected location and extent of the lesions to reduce more tissue dissections and iatrogenic trauma, so knowledge of variations in liver is important during radiological investigation and surgery [7].
Demarcation of right and left lobes anteriorly is along the line of attachment of the falciform ligament, posteriorly it is along the line of attachment of the ligamentum venosum and inferiorly along the fissure for the ligamentum teres, so these demarcations are important for division of right and left lobe of liver. Joshi SD et al., studied 90 specimens of liver and he observed that 30% of liver had variable diameter of pons hepatis, joining quadrate lobe and left lobe, which bridges the fissure for ligamentum teres, so normal appearance of the fissure would not be possible as well as diameter of both right and left lobe of liver may be mistaken [8]. Patil S et al., also observed similar findings in 10% specimen out of 50 liver specimens [9].
In the present study, similar finding was seen only in one liver specimen. Absence of fissure for ligamentum teres was present in 11.2% specimens and in 9.7% cases out of 41 livers by Muktyaz H and Nema U [2].
Major fissures like accessory hepatic fissure can be single or multiple and do not extend beyond the upper part of liver [8]. It is mainly due to invagination of musculature of diaphragm into the upper part of right lobe of liver and commonly seen in elderly patients. Subdiaphragmatic fat and the peritoneum accompany the muscular diaphragm in the accessory fissure and therefore when ascites is present, it can extend into the accessory fissures. On sectional imaging modalities, the accessory fissures are seen as single or multiple thin lines projecting inward from the periphery of the liver [8].
Diaphragmatic sulci develop from irregular growth of liver parenchyma caused due to resistance by different bundles of the diaphragm muscle. But recently, radiological and corrosion cast studies indicate the formation of sulci due to existing poor zones of liver parenchyma which are represented as portal fissures between the adjacent sagittal portal territories. Macchi V et al., suggested that the diaphragmatic sulci could be a good landmark for projection of the portal fissures and of the hepatic veins with their tributaries running through them [10].
Prominent vertical groove on anterosuperior surface were found in 6% of the liver by Joshi SD et al., [8]. A higher incidence of these grooves was observed by Macchi et al., [10]. In present study diaphragmatic sulci present in 7.5% specimens [Table/Fig-1].
Accessory lobe of liver is one of the most common morphological variations in the liver and it is usually asymptomatic. According to Collan Y et al., the liver parenchyma in communication with main liver is known as an accessory lobe and without communication is known as ectopic liver [11]. Sato S et al., have done 1800 laparoscopies and found congenital anomalies in 19% cases out of this 0.7% were accessory lobe and ectopic lobe of liver [12]. Embryologically the lungs and liver are derived from endodermal diverticuli of the foregut and are in close proximity. Accessory lobes are most commonly found on the under surface of the liver, but have also been seen on the gall bladder surface.
It is a tongue like projection of the right lobe of the liver and it is a simple anatomical variation [13].
Defective development of the left lobe of liver can lead to conditions like gastric volvulus. In contrast, defective development of the right lobe can remain clinically latent or progress to portal hypertension. Excessive development of the liver creates accessory lobes of liver which causes torsion [3]. It arises from right lobe of liver and may project in any direction. Riedel’s lobe is one of the good examples of a sessile accessory lobe which descends downwards along the right lateral surface and gives tongue like projection.
Presence of accessory lobes requires attention when there is torsion or metastasis occurring in them. Torsion of the accessory lobes is a surgical emergency and attended as early as possible [9,10]. Embryologically accessory lobes are formed by the displacement of the primitive rudiment of the organ, or by persistence of the mesodermal septa during proliferation [14], which occurs due to defective formation of the caudal foregut and hepatic bud in the third month of the intrauterine life [15].
A small sized accessory lobe is very important surgically and radiologically as it might be mistaken as lymph node, and be accidentally removed during the surgery or while dissection around the porta hepatis. This might lead to excessive bleeding in abdomen due to damage to lobes or vascular pedicle [15]. In our study, mini accessory lobes were present in 3.7% specimen.
It has been observed that on computed tomography, a normal sized or small papillary process may be mistaken for enlarged portahepatis nodes. Joshi SD et al., found notching along the inferior border of the caudate lobe in 18% of the livers and prominent papillary process in 32% [8].
In present study, prominent papillary process and long caudate process were seen in 1.25% specimen similar to findings of Nayak BS [16] [Table/Fig-15].
Comparison between present study and other studies showing variations in morphological features of liver.
| Morphological features | Joshi SD et al., [8] | Muktyaz H and nema U [2] | Patil S et al., [9] | Nayak BS [16] | Present Study |
|---|
| Accessory Fissures | 30% | 12.1% | 10% | 1.81% | 12.5% |
| Accessory Fissures on caudate lobe | - | - | - | - | 3.7% |
| Superior And Inferior Quadrate Lobe | 20% | - | 4% | - | 7.5% |
| Pons hepatis connecting left lobe with quadrate lobe | 30% | - | 10% | - | 1.25% |
| Absence of fissure for ligamentum teres | - | 9.7% | 4% | 1.81% | 11.2% |
| Riedel’s lobe present | - | - | - | - | 1.25% |
| Elongated left lobe present | - | - | - | 1.81% | 12.5% |
| Mini accessory lobe present | - | - | 2% | - | 3.7% |
| Large papillary process | 32% | - | - | 1.81% | 1.25% |
Aktan ZA et al., observed an absence of the caudate lobe in 7.41% of 54 livers [17]. Muktyaz H and Nema U found absence of the quadrate lobe in 1(2.4%) liver out of 41 livers studied. We did not find an absence of the caudate and quadrate lobe in our study [2].
Limitation
The sample size of our study was small and only those organs were included which were donated cadavers. Autopsy organs and paediatric organs were excluded. We could not perform a gender based study.
Conclusion
This study highlights the frequent occurrence of morphological variations on the surface of the liver. Now a days, these type of morphological variations are very important in cases of laparoscopic removal or thermal ablation of liver mass, So the knowledge of this kind of variations are important for surgeons and gastroenterologists in planning and performing the surgical procedures, for the radiologists to prevent a possible misdiagnosis and for the anatomists to find out new variants.