General anaesthesia combined with endotracheal intubation and controlled ventilation is the most common form of anaesthesia technique applied for different surgical specialties. To provide ventilation during general anaesthesia or in patients needing mechanical ventilation in intensive care units, disposable cuffed ETT is commonly used. The idea of using cuffed endotracheal tube is to achieve a seal between the cuff and the trachea with a pressure sufficient enough to prevent aspiration but not so much that tracheal blood flow is impeded. An acceptable cuff pressure ranges from 20 to 30 cm H2O [1].
This pressure limit is determined in part by capillary blood pressure supplying the trachea, which is approximately 48 cm H2O and the minimum occlusive intra-cuff pressure required for positive pressure ventilation, to prevent aspiration, i.e., approximately 20 cm H2O [1,2].
Thus, there is a narrow range of cuff pressures required to maintain a functionally safe seal without exceeding capillary blood pressure. There are many described methods of cuff inflation commonly employed; however the results are inconclusive. Two generally used methods of cuff inflation are JS and SG methods [3,4]. In the JS method, the ETT cuff is inflated to a sealing pressure until no leak can be heard from the mouth and also palpate the cuff pressure roughly by palpation of the pilot balloon. In SG method, the bell attachment of a stethoscope is used to auscultate for the presence of any leak (harsh breath sounds) around the tube.
Over inflation of the cuff may lead to ischemia, inflammation, ulceration, granulation and stenosis at the contact site between the cuff and the tracheal wall [4,5]. Moreover, postoperative sore throat is commoner in cases in which the endotracheal cuff pressure is elevated [5,6]. Also, this low risk complication can have legal implications [7]. Patients can also be at risk of aspiration if the cuff pressure is too low (<20 cm H2O).
Hence, to prevent the above complications and to improve quality of anaesthesia, we conducted the present study. We aimed to compare JS and SG methods of ETT cuff inflation with respect to the volume of air required to inflate the cuff, the manometric cuff pressure achieved by each method and also assess for the occurrence of postoperative sore throat after extubation in both the groups.
Materials and Methods
This was a prospective observational study done at a Tertiary Care Teaching Public Hospital after obtaining the Institutional Ethics Committee approval and Written and Informed valid consent of the patient. Study was conducted over a period of one and a half years from September 2012 to March 2014.
We studied one hundred patients ASA physical status 1 and 2 of both gender and aged between 18 – 60 years posted for elective surgeries under general anaesthesia with 50 each in both groups. In a previous study by Kumar RD and Hirsch NP, 64% of cuff pressures exceeded the recommended level of 30 cm H2O in the JS method of cuff inflation [3]. Targeting the same difference, with 95% confidence interval and 80% power, minimum sample size was calculated as 43 in each group using formula mentioned by Tilaki Hajian K [8]. We included 50 patients in each group. Also, patients undergoing emergency surgery and that with anticipated difficult intubation and pregnant as well as obese patients were excluded from the study.
Standard routine balanced general anaesthesia was administered and thereafter maintained with Sevoflurane in oxygen: air mixture and without nitrous oxide. After achieving standard intubating conditions, the trachea was intubated with a cuffed ETT; male patients received a tracheal tube with an internal diameter of 8.0 mm, and female patients received a tube of 7.0 mm internal diameter. The tracheal tube cuff was then inflated using one of two methods. In the JS method, the ETT cuff was inflated to a sealing pressure until no leak could be heard from the mouth and also palpated the cuff pressure roughly by palpation of the pilot balloon. In the SG method, the bell attachment of a stethoscope was used to auscultate over the thyroid lamina for the presence of any leak around the tube after cuff inflation that manifested in the form of harsh breath sounds during ventilation. The noted parameters included age, sex, Body Mass Index (BMI), Cormack and Lehane grade of intubation, ETT internal diameter, volume of air introduced into the cuff, cuff pressure achieved after cuff inflation and the occurrence of postoperative sore throat two hours after extubation. This was an observational study and grouping was done after data collection for the purpose of analysis.
Statistical Analysis
Appropriate statistical tests (parametric and non-parametric) were applied for the available data. A p-value of less than 0.05 was considered to be statistically significant. Sample size was also calculated accordingly [8].
Qualitative and quantitative data were represented in form of frequency and percentage and mean ± SD and median and IQR (Interquartile range) respectively. Association between qualitative variables was assessed by Chi-Square test with Continuity Correction for all 2 X 2 tables. Analysis of quantitative data between the two groups was done using Unpaired t-test if data passed ‘Normality test’ and by Mann-Whitney Test if data failed the test. Results were graphically represented where considered necessary. SPSS Version 17 was used for analysis. Microsoft Word and Excel were used for data representation.
Results
We studied 100 patients with 50 each in two groups JS or SG method of cuff inflation. The two groups were compared on the basis of multiple variables viz., age, sex, BMI, Cormack and Lehane grade of intubation, ETT internal diameter, volume of air introduced into the cuff, cuff pressure achieved and post-extubation sore throat [Table/Fig-1,2].
Comparison of various variables between the JS and SG cases viz. age, BMI, ET tube size, volume of air introduced into cuff, cuff pressure achieved.
| Variables | Method of Cuff inflation | Mean | SD | Median | IQR | t-value | p-value |
|---|
| Age (years)# | JS | 40.44 | 6.38 | 38.50 | 12.00 | -0.2 | 0.841 |
| SG | 40.68 | 7.06 | 40.00 | 11.00 | Difference is not significant |
| Body Mass Index (BMI) | JS | 22.92 | 1.26 | 22.90 | 2.05 | 0.114 | 0.91 |
| SG | 22.90 | 1.20 | 23.00 | 1.85 | Difference is not significant |
| ET Tube size (mm)# | JS | 7.74 | 0.74 | 7.75 | 1.50 | -0.495 | 0.621 |
| SG | 7.68 | 0.73 | 7.00 | 1.50 | Difference is not significant |
| Volume of air introduced (ml)# | JS | 6.79 | 1.09 | 6.50 | 1.25 | -8.095 | 5.71E- 16 |
| SG | 4.95 | 0.44 | 5.00 | 1.00 | Difference is significant |
| Cuff pressure (cm H2O)# | JS | 38.80 | 5.93 | 39.00 | 10.00 | -7.633 | 2.29E- 14 |
| SG | 29.64 | 1.84 | 30.00 | 2.00 | Difference is significant |
JS - Just seal. SG- Stethoscope guided. Unpaired t-test applied.
Data failed ‘Normality’ test. Hence Mann-Whitney test applied. t-value replaced by Z-value. Note: IQR= Interquartile Range (i.e., 75th Percentile-25th Percentile). SD= Standard deviation.
Association between the two groups on the basis of incidence of postoperative sore throat.
| Sore throat two hours after extuba- tion | | Method of cuff inflation | Total | |
|---|
| Just Seal | Stethoscope Guided |
|---|
| Yes | No. | 27 | 6 | 33 | | |
| % | 54.0% | 12.0% | 33.0% | | |
| No | No. | 23 | 44 | 67 | | |
| % | 46.0% | 88.0% | 67.0% | | |
| Total | No. | 50 | 50 | 100 | | |
| % | 100% | 100% | 100% | | |
| Chi-Square Tests | Value | Df | p-value | Association is |
| Pearson Chi- Square | 19.946 | 1 | 7.97E-06 (0.00000797) | Significant |
| Continuity Correction | 18.091 | 1 | 2.11E-05 (0.0000211) | Significant |
Chi-square tests used
Both the groups were comparable with respect to demographic parameters like age, sex and BMI. However, the volume of air introduced into the ETT cuff was significantly higher in the JS Group than that in the SG Group. The mean volume injected in JS method was 6.79 ml and in the SG method was 4.95 ml whereas the medians in both groups were 6.50 ml and 5.00 ml respectively. The minimum volume injected in JS group was 5.00 ml and the maximum was 9.00 ml. Minimum and maximum volumes in SG method were 4.00 ml and 5.50 ml respectively. Both the groups were compared on this variable with the Mann-Whitney test and significant difference was found (p-value <0.05) [Table/Fig-1,3].
Association between volume of air introduced (ml) into the cuff and cuff pressure achieved (cm H2O) in ‘Just Seal’ and ‘Stethoscope guided’ Methods (Median value).
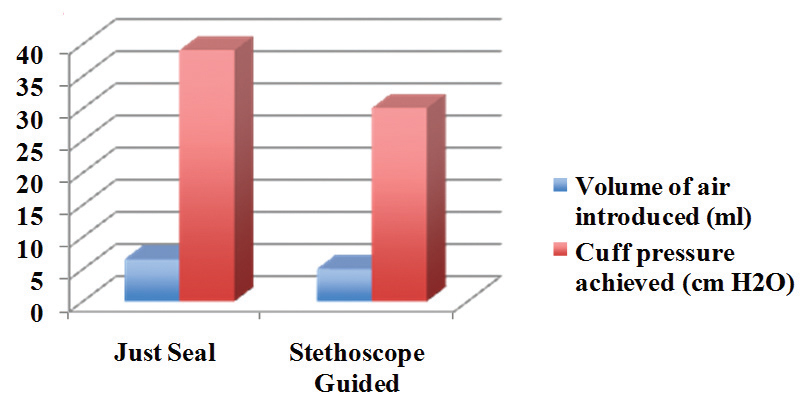
Similarly, the mean cuff pressure was 38.80 cm H2O in the JS Group and 29.64 cm H2O in the SG Group whereas the median pressure was 39.00 cm H2O in the former group and 30.00 cm H2O in the latter. The minimum cuff pressure achieved in the JS Group was 30.00 and the maximum was 50.00; on the other hand, minimum and maximum pressures in the SG method were 26.00 and 34.00 respectively. Only the SG method was able to achieve cuff pressure around the recommended range of 20-30 cm H2O [Table/Fig-1,3].
The incidence of sore-throat was 54% in the JS group and only 12% in the SG one. The two groups were compared by Pearson chi-square test and the difference was found to be significant (p-value < 0.05) thereby making the occurrence of sore-throat significantly higher in the JS group [Table/Fig-2].
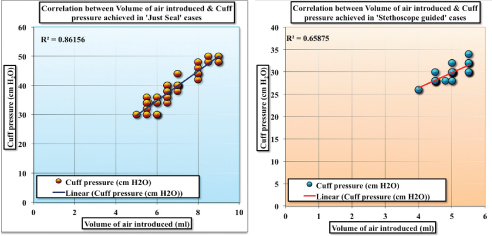
The association between volume of air introduced to inflate the endotracheal tube cuff (ml) and the resultant cuff pressure achieved (cm H2O) was studied and there was found to be a linear correlation between the two variables [Table/Fig-4].
Association between volume of air introduced to inflate the ETT cuff (ml) and the resultant cuff pressure achieved (cm H2O) in ‘Just Seal’ and ‘Stetho-scope Guided’ cases.
Discussion
Both the JS and SG groups were comparable with respect to parameters viz. age, sex, BMI, ETT size and Cormack Lehane grade of intubation. However, the volume of air introduced into the ETT cuff was significantly higher in the JS Group than that in the SG Group. Kumar RD and Hirsch NP in their evaluation of stethoscope-guided inflation of tracheal tube cuffs had measured the volumes of air introduced for inflation of the cuffs [3]. They had found that the volume of air was an insignificant finding but our study had demonstrated it otherwise.
Cuff pressure measured in the JS Group was significantly higher than that in the SG Group. This was in accordance with the study conducted by Kumar RD and Hirsch NP who had evaluated SG inflation of tracheal tube cuffs and found that the standard JS method was unreliable for inflating cuffs consistently to less than 30 cm H2O [3].
Sengupta P et al., had also studied the required volume to produce an appropriate cuff pressure and found that the crude method of palpation of the pilot balloon for adequate inflation and readjustment by inflating just enough to stop an audible leak is incapable of achieving an adequate pressure [5].
Post extubation patients commonly complain of sore-throat and hoarseness of voice. This is related to the cuff pressure developed and its effect on the tracheal mucosal blood flow. In our study, we asked patients for complaint of sore-throat (that is slightly more common than hoarseness) two hours after extubation. The incidence was significantly higher in the JS method than in the SG.
This was similar to the study of McHardy FE et al., who had studied the cause, prevention and treatment of postoperative sore throat and recommended that intracuff pressure should be maintained at a lower level of around 26 cm H2O that helps to reduce incidence of post extubation airway related complications like sore throat [9].
Suzuki N et al., had studied postoperative hoarseness and sore throat after tracheal intubation and effect of low intracuff pressure of the endotracheal tube [10]. They had recommended a cuff pressure of less than 33 cm H2O and monitoring of this cuff pressure with a pressure gauge.
Thus, our study was successful at deducing significant differences in the ETT cuff pressure achieved between two common methods of cuff inflation thereby serving its purpose and providing us with valuable information related to secure and safe management of the airway both during and post anaesthesia.
limitation
The present study was not without limitations as the ETT cuff pressure was measured just once immediately after induction of anaesthesia. Although nitrous oxide that has a property of diffusing into pre air filled spaces, was not used in this study, still changes in the cuff volume and possible rise in the cuff pressure later during anaesthesia could not be guaranteed.
The patient may have a number of complaints post extubation viz., sore throat, hoarseness, dryness of the mouth, dysphagia etc. In our study, only sore throat was considered because it was common than the most. Besides, raised ETT cuff pressure being an important factor in the causation of post extubation complications, the role of other factors e.g., presence of a nasogastric tube, multiple attempts at intubation etc., could not be ruled out.
Also, advanced methods to guide cuff inflation are available e.g., pressure volume loop closure that have shown promising results in effectively sealing the airway and achieving lower ETT cuff pressure and resultant lesser cuff related complications [11,12].
Conclusion
The volume of air required to inflate the ETT cuff was more in the ‘JS’ Group than the ‘SG’. The resultant cuff pressure attained after inflation with air was more in the former group than the latter. Incidence of post extubation complications like sore throat was more common in the JS Group.
Thus, the SG method of ETT cuff inflation is found to be superior to the JS in terms of achieving cuff pressures within the recommended range and the consequent lesser occurrence of complications.
It is a simple, reproducible, safe and rapid technique that produces reliable cuff pressures below the recommended maximum limit of 30 cm H2O. In contrast, cuff inflation by just sealing produces cuff pressures consistently in a range higher than that advocated.
Endotracheal tube cuff inflation under the guidance of a stethoscope is an effective and dependable technique for ensuring optimal tracheal cuff pressures and so we suggest its use as a standard and routine procedure that would serve as an accomplishment towards excellence in Anaesthesiology and Critical Care.
JS - Just seal. SG- Stethoscope guided. Unpaired t-test applied.
#Data failed ‘Normality’ test. Hence Mann-Whitney test applied. t-value replaced by Z-value. Note: IQR= Interquartile Range (i.e., 75th Percentile-25th Percentile). SD= Standard deviation.
Chi-square tests used