Bile Duct Adenocarcinoma with Acute on Chronic Pancreatitis: A Rare Complication of Long Standing Choledochal Cyst
Ashish Gupta1, Lileswar Kaman2
1 Senior Medical Officer, Department of Hospital Administration, PGIMER, Chandigarh, India.
2 Professor, Department of General Surgery, Chandigarh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Lileswar Kaman, Professor, Department of General Surgery, PGIMER, Chandigarh-160012, India.
E-mail: drashish0403@yahoo.in
Cholangiocarcinoma, Cholangitis, Obstructive jaundice
Cholangiocarcinoma rarely develops in a long standing choledochal cyst. Its association with cholangitis, gall stones and pancreatitis is well known. However, occurrence of choledochal cyst with adenocarcinoma with pancreatitis changes is rarely reported.
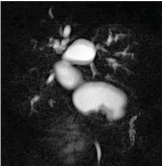
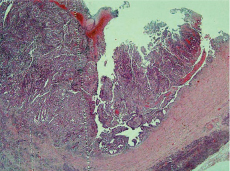
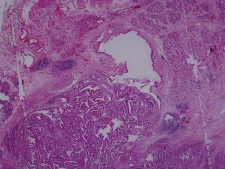
A 46-year-old female presented to surgical outpatient with obstructive jaundice, pain abdomen with loss of weight and appetite for the past two months. She also had complaints of fever with chills and rigors. On clinical examination, there was hepatomegaly without clinical evidence of metastatic disease. Liver function tests were Bilirubin Total/Direct 14/7(gm%), SGOT/SGPT/ALP- 166/149/1076 (IU/dl). Total leucocyte count of the patient was 19000 cells/dl. Ultrasound of the patient revealed a type IV A choledochal cyst. Magnetic Resonance Cholangiopancreatography (MRCP) confirmed the type IV A choledochal cyst with mucosal thickening on the lateral wall [Table/Fig-1]. Carbohydrate antigen 19.9 was 463 (N=0-37u/ml). She was started on intravenous piperacillin and tazobactam at a dose of 4.5 gm eighth hourly. She responded to conservative management and was planned for surgery after optimization. Intraoperatively there was cystic dilatation of the extrahepatic bile duct 10 by 6 cm in size with thickening of the lower end of the Common Bile Duct (CBD). There was no metastasis in the abdomen. A classical Pancreaticoduodenectomy was performed and specimen showing the thickened CBD wall [Table/Fig-2]. Histopathology of the specimen confirmed thickening with adenocarcinoma of choledochal cyst [Table/Fig-3]. Acute on chronic pancreatitis changes with infiltration of pancreas by tumor cells was present in the specimen. [Table/Fig-4]. The resection margins were free of tumour. She has received gemcitabine based chemotherapy and is doing well after two years of follow up.
MRCP showing the choledochal cyst with mucosal thickening of the wall.
Gross Pancreaticoduodenectomy specimen showing the thickened CBD wall

Photomicrograph (10x) showing the cyst infiltrated by malignant cells;
Photomicrograph (10x) showing the acute on chronic changes with infiltration of pancreas by malignant cells.
Choledochal cyst when diagnosed late in life, carries risk of developing malignancy. The life time association of cholangiocarcinoma with choledochal cyst is 20-25% [1]. The risk increases with the duration of the undiagnosed cyst. The typical malignancy is adenocarcinoma of the bile duct, less commonly squamous cell carcinoma [2]. Prior drainage of cyst without excision also increases the risk [3]. The malignancy may also involve the pancreatic duct, gall bladder or intrahepatic ducts. Choledochal cyst with nodular thickening as in present case is a marker of malignant transformation [4].
The carcinoma can arise even after excision of type IV A cyst. This may arise in intrapancreatic portion or even dilated intrahepatic ducts [5]. Hence, the extent of surgery for type IV A cyst is debatable [6]. However in the present case pancreatic head was also excised so the recurrence can arise from intrahepatic bile ducts or from the anastomotic site.
Management of Cholangiocarcinoma depends upon the level of the cancer. Distal CBD carcinoma mandates pancreaticoduodenectomy while proximal tumours require hepatectomy with caudate lobe resection [7]. Adjuvant treatment includes radiotherapy and chemotherapy. Gemcitabine-based chemotherapy has improved the survival in patients with advanced cholangiocarcinoma [8]. Chaturvedi A et al., opined the poor prognosis of cholangiocarcinoma mainly because of advanced stage and late detection. Our patient is disease free two years after the index surgery [3].
Cholangiocarcinoma along with acute on chronic pancreatitis are etiologically related in this index case. Both of them are well known complications of the neglected choledochal cysts. Simultaneous occurrence of both of these entities has rarely been reported in literature. The unique presentation in this index patient emphasizes the importance of early detection and excision of these congenital malformations with a roux en Y bilioenteric bypass.
[1]. De Vries JS, De Vries S, Aronson DC, Bosman DK, Rauws EA, Bosma A, Choledochal cysts: age of presentation, symptoms, and late complications related to Todani’s classificationJournal of Pediatric Surgery 2002 37(11):1568-73. [Google Scholar]
[2]. Lee TS, Kim HK, Ahn HM, Lee UJ, Choi YC, John BM, A case of early bile duct cancer arising from villous adenoma in choledochal cystKorean J Gastroenterol 2009 54:55-59. [Google Scholar]
[3]. Chaturvedi A, Singh J, Rastogi V, Case report: Cholangiocarcinoma in a choledochal cystIndian J Radiol Imaging 2008 18:236-38. [Google Scholar]
[4]. Yoshida H, Itai Y, Minami M, Kokubo T, Ohtomo K, Kuroda A, Biliary malignancies occurring in choledochal cystsRadiology 1989 173(2):389-92. [Google Scholar]
[5]. Ando H, Kaneko K, Ito T, Watanabe Y, Seo T, Harada T, Complete excision of the intrapancreatic portion of choledochal cystsJournal of the American College of Surgeons 1996 183(4):317-21. [Google Scholar]
[6]. Lopez RR, Pinson CW, Campbell JR, Harrison M, Katon RM, Variation in management based on type of choledochal cystThe American journal of surgery 1991 161(5):612-15. [Google Scholar]
[7]. Nakeeb A, Pitt HA, Sohn TA, Coleman J, Abrams RA, Piantadosi S, Cholangiocarcinoma. A spectrum of intrahepatic, perihilar, and distal tumoursAnnals of Surgery 1996 224(4):463 [Google Scholar]
[8]. Dasanu CA, Majumder S, Trikudanathan G, Emerging pharmacotherapeutic strategies for cholangiocarcinomaExpert Opin Pharmacother 2011 12:1865-74. [Google Scholar]