Vocal Hoarseness in Rheumatoid Arthritis: Early Recognition is Critical
James Benjamin Gleason1, Anas Hadeh2
1 Fellow, Department of Pulmonary and Critical Care Medicine, Cleveland ClinicFlorida, Weston, Florida, USA.
2 Attending Physician, Department of Pulmonary and Critical Care Medicine, Cleveland ClinicFlorida, Weston, Florida, USA.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. James Benjamin Gleason, 2950, Cleveland Clinic BLVD, Weston, Florida-33331, USA.
E-mail: gleasoj@ccf.org
Airway emergency, Bilateral vocal cord paralysis, Cricoarytenoid arthritis
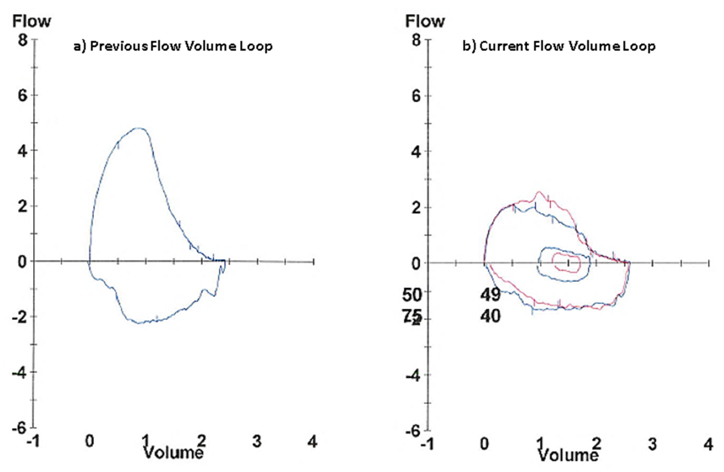
A 76-year-old male with severe refractory rheumatoid arthritis [Table/Fig-1] developed hoarseness of his voice and difficulty in speaking. His symptoms progressed to increasingly noisy breathing, exertional dyspnea and finally inspiratory stridor. He underwent evaluation with pulmonary function testing which demonstrated flow-volume loops consistent with a new variable upper airway obstruction [Table/Fig-2]. Laryngoscopy was performed and revealed that both vocal cords in the median (adducted) position with only a small residual airway at the posterior commissure [Table/Fig-3]. This patient’s critical airway obstruction was an indication for urgent tracheostomy. Bilateral vocal cord paralysis, an infrequent but life threatening complication of rheumatoid arthritis [1,2], results from cricoarytenoid arthritis and should be considered by clinicians in those with rheumatoid arthritis and vocal hoarseness or dyspnea. The chronic inflammatory changes to the cricoarytenoid joint results in ankylosis and decreased mobility of both vocal cords [3,4]. Less serious laryngeal complications of rheumatoid arthritis such as oedema, myositis, epiglottitis, and rheumatoid nodules are frequently found but are not airway emergencies. Early recognition of the condition we described was paramount and timely surgical intervention is necessary for the immediate resolution of obstruction and dyspnea due to median position bilateral vocal cord paralysis.
Typical rheumatoid arthritis related ulnar deviation of metacarpophalangeal joints and swan neck deformities of the fingers.

a) Previous flow-volume loop with mild obstruction; b) Current flow-volume loop demonstrating plateau of the inspiratory arm consistent with variable upper airway obstruction.
Both vocal cords fixed in the adducted position during both inspiration and exhalation consistent with bilateral vocal cord paralysis. (Images left to right)

[1]. Braverman I, Malatskey S, Avior G, Bilateral vocal cord paralysis due to rheumatoid arthritisHarefuah 2007 146(2):92-94. [Google Scholar]
[2]. Kolman J, Morris I, Cricoarytenoid arthritis: a cause of acute upper airway obstruction in rheumatoid arthritisCanadian Journal of Anaesthesia 2002 49(7):729-32. [Google Scholar]
[3]. Bienenstock H, Ehrlich GE, Freyberg RH, Rheumatoid arthritis of the cricoarytenoid joint: a clinicopathologic studyArthritis & Rheumatism 1963 6(1):48-63. [Google Scholar]
[4]. Voulgari PV, Papazisi D, Bai M, Zagorianakou P, Assimakopoulos D, Drosos AA, Laryngeal involvement in rheumatoid arthritisRheumatology International 2005 25(5):321-25. [Google Scholar]