Congenital Bilobed Gallbladder with Phrygian Cap Presenting as Calculus Cholecystitis
N.S. Kannan1, Usha Kannan2, C.P. Ganesh Babu3
1 Associate Professor, Department of General Surgery, Mahatma Gandhi Medical College & Research Institute, Pillaiyarkuppam, Pondicherry, India.
2 Assistant Professor, Department of Anatomy, Mahatma Gandhi Medical College & Research Institute, Pillaiyarkuppam, Pondicherry, India.
3 Professor, Department of General Surgery, Mahatma Gandhi Medical College & Research Institute, Pillaiyarkuppam, Pondicherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. N.S.Kannan, Associate Professor, Department of General Surgery, Mahatma Gandhi Medical College & Research Institute, Pillaiyarkuppam, Pondicherry-607402, India. Phone : 9843330521, E-mail : drnskannan@yahoo.co.in
The incidence of congenital bilobed gall bladder is 1 in 3000 to 4000. A Phrygian cap is a congenital abnormality of the gallbladder with an incidence of 4%. Preferred mode of diagnosis for Phrygian cap is cholescintigraphy and multi phase MRI, as Ultrasonography and CT are not always conclusive. The estimated prevalence of gallstone disease in India has been reported as 2% to 29%. A case of bilobed gall bladder with Phrygian cap in both the lobes and pigment gallstone in one of the lobes presenting as calculus cholecystitis is reported for its rarity and difficulty in arriving at correct preoperaive diagnosis
Congenital gallbladder anomaly, Cholescintigraphy, Hepatobiliary imaging, Multi phase MRI
Case Report
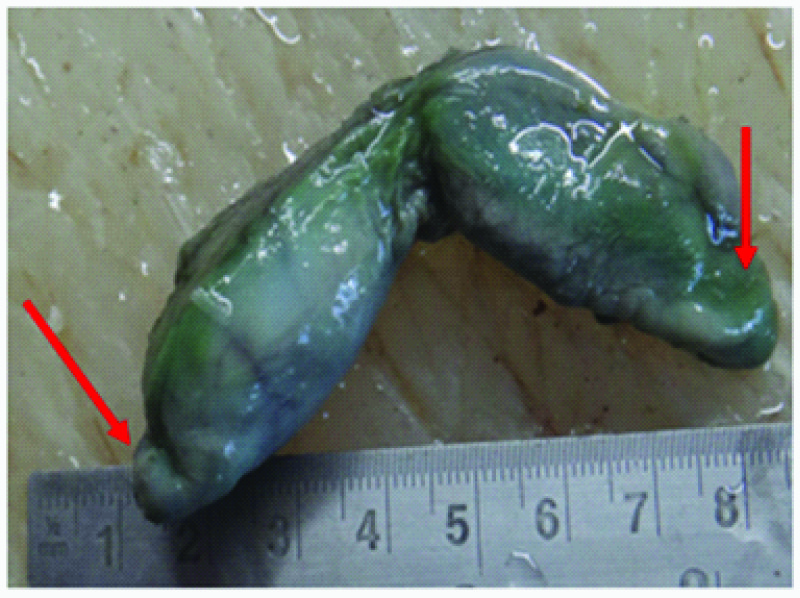
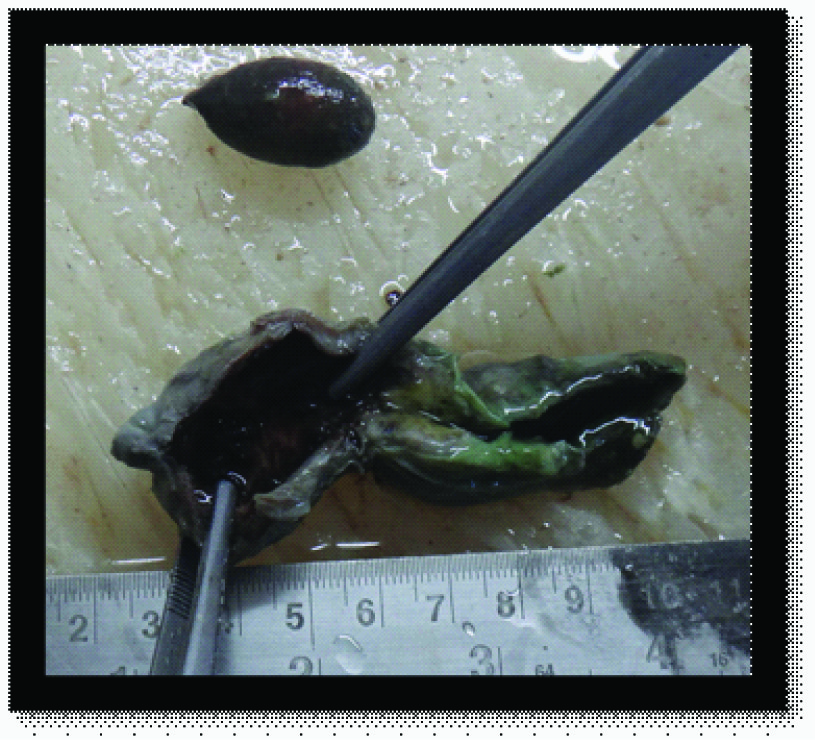
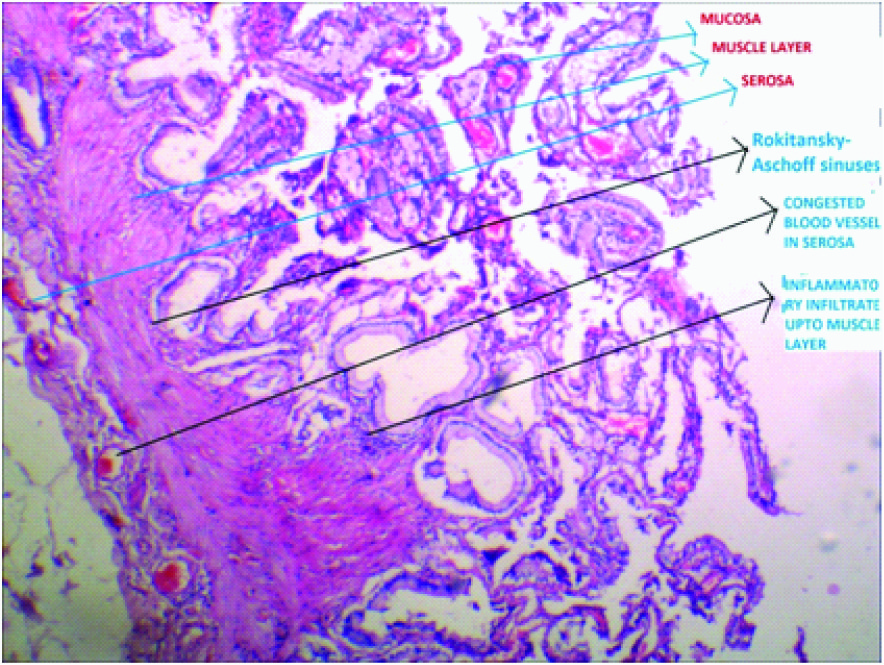
A 55-year-old male, presented with right upper abdominal pain radiating to the right shoulder associated with regurgitation and belching with no other abdominal or systemic symptoms. On clinical examination, abdomen was soft with tenderness in the right hypochondrium and no other positive abdominal findings. Ultrasound examination showed a 30mm single calculus in the gall bladder with wall thickening [Table/Fig-1]. Due to persistence of symptoms, patient was posted for elective cholecystectomy. Right subcostal, muscle splitting technique was done to access the abdomen. Intra-operatively, the gall bladder was found to be bilobed with Phrygian cap in both the lobes. Resected specimen is shown in [Table/Fig-2]. One of the lobes was lodging a pigmented stone measuring 3x1cm [Table/Fig-3]. Rest of the abdomen was normal. Cholecystectomy was done and abdomen closed in layers. Histopathological examination showed chronic cholecystitis [Table/Fig-4]. Postoperative period was uneventful.
Ultrasound picture showing 30mm gall stone

Resected bilobed-gall bladder with Phrygian caps in each lobes.
Bilobed-gall bladder with Phrygian caps in each lobe, cut open after resection shows a single pigmented gall stone in one of the lobes
Hitopathology showing chronic cholecystitis
Discussion
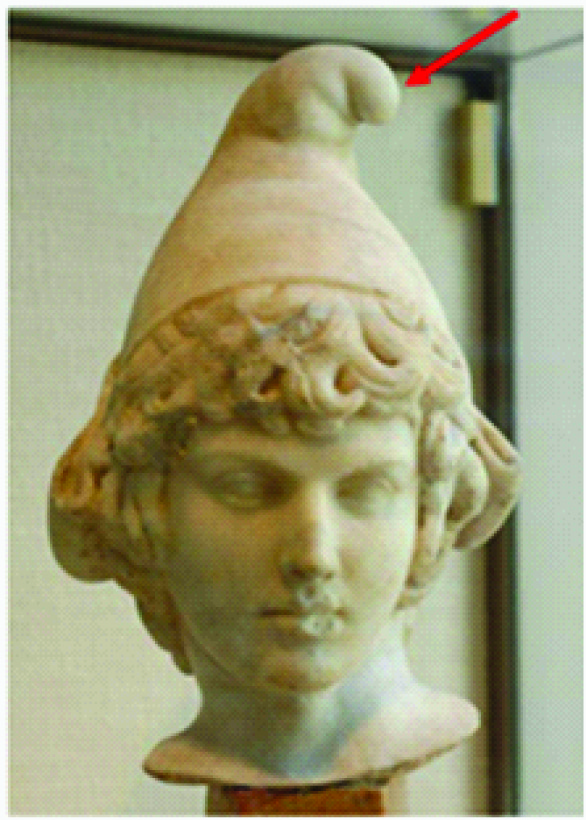
The incidence of congenital bilobed gall bladder is 1 in 3000 to 4000 [1]. The estimated prevalence of gallstone disease in India has been reported as 2% to 29% [2]. A Phrygian cap is a congenital abnormality of the gallbladder with an incidence of 4% [3]. It is named after the headgear worn by ancient Greek slaves as a sign of liberation /a head garment worn by inhabitants of Phrygia (modern Turkey) 1200 - 700 BC [Table/Fig-5]. It was first described by Boyden EA in 1935 [4]. This deformity is characterized by a fold of the gallbladder between the body and fundus. It is the most common congenital anomaly of the gallbladder and can simulate a mass in the liver during hepatobiliary imaging [4,5], which may suggest a tumour. It can also simulate a duplication of the gallbladder [6]. It is a benign anatomical abnormality, per se usually asymptomatic unless complicated with calculus or a calculus cholecystitis. Gall bladder with Phrygian cap deformity can lead to misdiagnosis of gall bladder stones on B-mode ultrasonography. Preferred mode of diagnosis for Phrygian cap is cholescintigraphy and multi phase MRI, as Ultrasonography and CT are not always conclusive. It is therefore important to use proper imaging techniques to differentiate between a Phrygian cap and other diagnoses [7]. Phrygian cap has to be differentiated from septate gallbladder [8], hour glass gall bladder [9], bilobed gallbladder [10] and other congenital anomalies of gall bladder [11]. Prophylactic cholecystectomy is not indicated in patients with Phrygian cap deformity alone as it is of no pathological significance. Surgery is done only for patients with symptoms or complications of gall bladder disease irrespective of Phrygian cap deformity. Extensive literature search has not shown any report of bilobed gall bladder with Phrygian cap deformity in both the lobes in human being. However this has been reported in monkeys [12].
A head garment worn by inhabitants of Phrygia (modern Turkey) 1200 - 700
Conclusion
This case report is presented for the following points: (1). Phrygian cap is a congenital abnormality of the gallbladder and has an incidence of 4%. The incidence of congenital bilobed gall bladder is 1 in 3000 to 4000. (2). Gall bladder with Phrygian cap deformity can lead to misdiagnosis of gall bladder stones or a mass in the liver during hepatobiliary imaging which may suggest a tumour. on B-mode ultrasonography. Preferred mode of diagnosis for Phrygian cap is cholescintigraphy and multi phase MRI. (3). Extensive literature search has not shown any report in human being of rare combination of two congenital abnormalities i.e. bilobed gall bladder with Phrygian cap in both the lobes as in our case. (4). Prophylactic cholecystectomy is not indicated in patients with Phrygian cap deformity alone as it is of no pathological significance. Surgery is done only for patients with symptoms or complications of gall bladder disease irrespective of Phrygian cap deformity.
[1]. Boyden EA, The accessory gallbladder-an embryological and comparative study of aberrant biliary vesicles occurring in man and domestic mammalsAm J Anast 1926 38:177-231. [Google Scholar]
[2]. Khurro MS, Mahajan R, Zargar SA, Javid G, Prevalence of biliary tract disease in India: a sonographic study in adult population in KashmirGut 1989 30:201-05. [Google Scholar]
[3]. De Csepel J, Carroccio A, Pomp A, Soft-tissue images. ‘Phrygian cap’ gallbladderCan J Surg 2003 46:50-1. [Google Scholar]
[4]. Boyden EA, The phrygian cap in cholecystography: a congenital anomaly of the gallbladderAm J Radiol 1935 33:589 [Google Scholar]
[5]. Smergel EM, Maurer AH, Phrygian cap simulating mass lesion in hepatobiliary scintigraphyClin Nucl Med 1984 9:131-33. [Google Scholar]
[6]. Dalal S, Chauhan TS, Kumar R, Choudhury SR, Pseudo-duplication of the gall bladder due to Phrygian cap – a case reportInternet J Surg 2013 29:8 [Google Scholar]
[7]. Van Kamp M-JS, Bouman DE, Steenvoorde P, Klaase JM, A Phrygian CapCase Rep Gastroenterol 2013 7(2):347-51. [Google Scholar]
[8]. Mohan B, Septate gallbladderCanadian Journal of Surgery 1965 8:84 [Google Scholar]
[9]. Harlaftis N, Gray SW, Skandalakis JE, Multiple gallbladdersSurgery,Gynecology & Obstetrics 1977 145:928 [Google Scholar]
[10]. Hobby JAE, Bilobed gallbladderBr J Surg 1970 57:870-72. [Google Scholar]
[11]. Gross RE, Congenital anomalies of the gallbladder: a review of 148 cases with report of a double gall bladder Arch Surg 1936 32:131-62. [Google Scholar]
[12]. Kirkman H, A simian, deeply cleft, bilobed gall bladder with a Phrygian capAnat Rec 1946 95:423-47. [Google Scholar]